You might also like
- Recurrent Intracranial Epidural Hematoma Following Ventriculoperitoneal Shunt in A ChildDocument2 pagesRecurrent Intracranial Epidural Hematoma Following Ventriculoperitoneal Shunt in A ChildwadejackNo ratings yet
- Recurrent Intracranial Epidural Hematoma Following Ventriculoperitoneal Shunt in A ChildDocument2 pagesRecurrent Intracranial Epidural Hematoma Following Ventriculoperitoneal Shunt in A ChildwadejackNo ratings yet
- Case Report: Contrast-Induced Encephalopathy Following Cerebral Angiography in A Hemodialysis PatientDocument4 pagesCase Report: Contrast-Induced Encephalopathy Following Cerebral Angiography in A Hemodialysis PatientAnaNo ratings yet
- Decompressive Hemicraniectomy in Malignant Infarction of Theinternal Carotid ArteryDocument5 pagesDecompressive Hemicraniectomy in Malignant Infarction of Theinternal Carotid ArteryPrathmesh MishraNo ratings yet
- Endovascular Management of Acute Epidural Hematomas: Clinical Experience With 80 CasesDocument7 pagesEndovascular Management of Acute Epidural Hematomas: Clinical Experience With 80 CasesDeby AnditaNo ratings yet
- 1 Abses SerebelumDocument6 pages1 Abses SerebelumseruniallisaaslimNo ratings yet
- Contrecoup Epidural HematomaDocument8 pagesContrecoup Epidural HematomaTrisna LaroehaNo ratings yet
- 4.3.1. Jurnal Stroke Hemoragik - Rosita Milandani - NIM 202311101168Document6 pages4.3.1. Jurnal Stroke Hemoragik - Rosita Milandani - NIM 202311101168RositaNo ratings yet
- Middle Meningeal Artery Embolization For Chronic Subdural Hematoma in Elderly Patients at High Risk of Surgical TreatmentDocument8 pagesMiddle Meningeal Artery Embolization For Chronic Subdural Hematoma in Elderly Patients at High Risk of Surgical TreatmentJUANNo ratings yet
- Epidural Hematoma: Continuing Education ActivityDocument16 pagesEpidural Hematoma: Continuing Education ActivityIka AriandanaNo ratings yet
- 2022 Perioperative Complications of Transvenous Embolization of Ruptured Intracranial Arteriovenous MalformationsDocument7 pages2022 Perioperative Complications of Transvenous Embolization of Ruptured Intracranial Arteriovenous MalformationsstaseaditNo ratings yet
- Practneurol 2020 002763Document12 pagesPractneurol 2020 002763Fitri ainun MalahayatiNo ratings yet
- Acute Intracerebral Haemorrhage - Pract Neurol (2021)Document12 pagesAcute Intracerebral Haemorrhage - Pract Neurol (2021)Billy Priyanto HNo ratings yet
- Acute Intracerebral Haemorrhage BMJ 2021Document12 pagesAcute Intracerebral Haemorrhage BMJ 2021Jennifer MorenoNo ratings yet
- Rare and Fatal Complication of Infective Endocarditis: Emergency Case SeriesDocument3 pagesRare and Fatal Complication of Infective Endocarditis: Emergency Case SeriesVika DamayNo ratings yet
- Anterior Acute Myocardial Infarction Complicated With Ventricular Septal Rupture: Case Reports and Literature ReviewDocument5 pagesAnterior Acute Myocardial Infarction Complicated With Ventricular Septal Rupture: Case Reports and Literature ReviewIJAR JOURNALNo ratings yet
- 1 s2.0 S1878875017319708 MainDocument4 pages1 s2.0 S1878875017319708 MainNikkie SalazarNo ratings yet
- Acute Cerebral Infarction Masked by A Brain Tumor: Kwo-Whei Lee Chung-Ping LoDocument6 pagesAcute Cerebral Infarction Masked by A Brain Tumor: Kwo-Whei Lee Chung-Ping LoCharina Geofhany DeboraNo ratings yet
- Acute Aortic Dissection Type A Extended, Complicated Extensive Stroke About A Case, and Literature ReviewDocument31 pagesAcute Aortic Dissection Type A Extended, Complicated Extensive Stroke About A Case, and Literature ReviewIJAR JOURNALNo ratings yet
- Acute Aortic Dissection Type A Extended, Complicated Extensive Stroke About A Case, and Literature ReviewDocument31 pagesAcute Aortic Dissection Type A Extended, Complicated Extensive Stroke About A Case, and Literature ReviewIJAR JOURNALNo ratings yet
- ACV HemorrágicoDocument12 pagesACV HemorrágicoLUIS FELIPE ARTEAGA ARREDONDONo ratings yet
- Video: FocusDocument2 pagesVideo: Focusivonne perezNo ratings yet
- A Rural Area Problem of Large Epidural Hematoma With HerniationDocument5 pagesA Rural Area Problem of Large Epidural Hematoma With Herniationrian00019No ratings yet
- 128 FullDocument12 pages128 FullYovita LimiawanNo ratings yet
- 4275 15730 1 PBDocument3 pages4275 15730 1 PBNiarsari A. PutriNo ratings yet
- Acute Intracerebral HaemorrhageDocument12 pagesAcute Intracerebral HaemorrhageZARF27No ratings yet
- Traumatic Bilateral Jugular Vein Thrombosis Case Report and Review of The LiteratureDocument4 pagesTraumatic Bilateral Jugular Vein Thrombosis Case Report and Review of The LiteratureMesay AssefaNo ratings yet
- Acute Intracerebral HeamorrhageDocument12 pagesAcute Intracerebral HeamorrhagePaul CalderónNo ratings yet
- Cerebral Abscess and Mycotic Aneurysm As A Consequence of Infective Endocarditis: A Case ReportDocument7 pagesCerebral Abscess and Mycotic Aneurysm As A Consequence of Infective Endocarditis: A Case ReportIJAR JOURNALNo ratings yet
- 128 FullDocument12 pages128 FullMarlen Adriana Hilario GómezNo ratings yet
- Journal Reading Radiology Gita Kristy Saraswati 1810221010Document43 pagesJournal Reading Radiology Gita Kristy Saraswati 1810221010Ara Runa ConstellatiaNo ratings yet
- (26941902 - Journal of Neurosurgery - Case Lessons) Traumatic Aneurysm at The Superior Cerebellar Artery - Illustrative CaseDocument5 pages(26941902 - Journal of Neurosurgery - Case Lessons) Traumatic Aneurysm at The Superior Cerebellar Artery - Illustrative CaseCharles MorrisonNo ratings yet
- Conclusion: Long-Term Follow-Up ForDocument31 pagesConclusion: Long-Term Follow-Up ForHima HuNo ratings yet
- Surgical Neurology International: Cordectomy For Intramedullary Spinal Cord Glioblastoma With A 12 Year SurvivalDocument5 pagesSurgical Neurology International: Cordectomy For Intramedullary Spinal Cord Glioblastoma With A 12 Year Survivallucasnegromonte0001No ratings yet
- Grupo 2 - INTERHEMISPHERIC SUBDURAL HAEMATOMADocument5 pagesGrupo 2 - INTERHEMISPHERIC SUBDURAL HAEMATOMAMarihan Paula Ticona PazNo ratings yet
- Background: Post-Traumatic Acute Subdural Hematomas Generally Appear Hyperdense On A ComputedDocument3 pagesBackground: Post-Traumatic Acute Subdural Hematomas Generally Appear Hyperdense On A ComputedJefta AlfatraNo ratings yet
- Practneurol 2020 002763Document12 pagesPractneurol 2020 002763Edgar MoralesNo ratings yet
- Neurocritical Management of Traumatic Acute Subdural HematomasDocument13 pagesNeurocritical Management of Traumatic Acute Subdural HematomasLiana Ika SuwandyNo ratings yet
- The Features of ECG and Echocg Functional Parameters in Children With Congenital Heart Disease in The Postoperative PeriodDocument5 pagesThe Features of ECG and Echocg Functional Parameters in Children With Congenital Heart Disease in The Postoperative PeriodCentral Asian StudiesNo ratings yet
- Eco Doppler Trascraneal 5Document15 pagesEco Doppler Trascraneal 5David Sebastian Boada PeñaNo ratings yet
- Main PDFDocument3 pagesMain PDFanton MDNo ratings yet
- 個案報告:游離齒突小骨導致後循環復發性中風Document6 pages個案報告:游離齒突小骨導致後循環復發性中風王湘淇No ratings yet
- Are Acute Subdural Hematomas Possible Without Head Trauma?: Case SeriesDocument5 pagesAre Acute Subdural Hematomas Possible Without Head Trauma?: Case SeriesYohanna YohannaNo ratings yet
- 1 Neurosurgery Cases and ReviewsDocument5 pages1 Neurosurgery Cases and ReviewsintodoieblissNo ratings yet
- EN07 Sindrom CushingDocument8 pagesEN07 Sindrom CushingAryanto AntoNo ratings yet
- Multiple Cerebral Aneurysms Originating From Previously Resected Cardiac MyxomaDocument4 pagesMultiple Cerebral Aneurysms Originating From Previously Resected Cardiac MyxomaRevista Angolana de Ciências da SaúdeNo ratings yet
- Lee Et Al 2023 Concurrent Acute Ischemic Stroke and Myocardial Infarction Associated With Atrial FibrillationDocument5 pagesLee Et Al 2023 Concurrent Acute Ischemic Stroke and Myocardial Infarction Associated With Atrial FibrillationBlackswannnNo ratings yet
- EDH Jurnal 3Document6 pagesEDH Jurnal 3Rizky AdityaNo ratings yet
- Letters: Safety of Angioplasty For Intracranial Artery ReferencesDocument5 pagesLetters: Safety of Angioplasty For Intracranial Artery Referencesaula nisafitriNo ratings yet
- Medi 98 E18430Document2 pagesMedi 98 E18430Anonymous tG35SYROzENo ratings yet
- 1 s2.0 S1572346110003442 MainDocument3 pages1 s2.0 S1572346110003442 MainAulia putriNo ratings yet
- 2694 1902 Article CASE2263Document4 pages2694 1902 Article CASE2263Aleksandar DimovskiNo ratings yet
- Value of Repeated Imaging in Patients With A Stroke Who Are Transferred For Endovascular TreatmentDocument5 pagesValue of Repeated Imaging in Patients With A Stroke Who Are Transferred For Endovascular TreatmentRafika Ayu NadiaNo ratings yet
- Oamjms 9c 146Document5 pagesOamjms 9c 146Seno adipNo ratings yet
- CE (Ra1) F (SHU) PF1 (A SHU)Document5 pagesCE (Ra1) F (SHU) PF1 (A SHU)Anwesa ChakrabortyNo ratings yet
- Intracranial Haemorrhage (ICH) Occurs in About 5% of Patients With IEDocument5 pagesIntracranial Haemorrhage (ICH) Occurs in About 5% of Patients With IETnf-alpha DelusionNo ratings yet
- Choi 2013Document6 pagesChoi 2013arun gowdaNo ratings yet
- A Rare Case of Isolated Celiac Artery Dissection Diagnosed in The Emergency DepartmentDocument5 pagesA Rare Case of Isolated Celiac Artery Dissection Diagnosed in The Emergency DepartmentIJAR JOURNALNo ratings yet
- 852-Article Text-1602-1-10-20190613Document12 pages852-Article Text-1602-1-10-20190613anidar1245No ratings yet
- Cerebrovascular Complications of COVID-19: Brief ReportDocument5 pagesCerebrovascular Complications of COVID-19: Brief ReportAmandaNo ratings yet
- Neurophysiology of Deep Brain StimulationDocument33 pagesNeurophysiology of Deep Brain StimulationAik NoeraNo ratings yet
- LARIO Score For LVO - 2019Document5 pagesLARIO Score For LVO - 2019Aik NoeraNo ratings yet
- Deep Brain Stimulation: An Overview of History, Methods, and Future DevelopmentsDocument6 pagesDeep Brain Stimulation: An Overview of History, Methods, and Future DevelopmentsAik NoeraNo ratings yet
- Pathophysiology of Dystonia: G. Madeo and A. PisaniDocument22 pagesPathophysiology of Dystonia: G. Madeo and A. PisaniAik NoeraNo ratings yet
- Anatomical Variations of A CommDocument4 pagesAnatomical Variations of A CommAik NoeraNo ratings yet
- Weight Loss Outcomes in Patients With Pain: ObesityDocument7 pagesWeight Loss Outcomes in Patients With Pain: ObesityAik NoeraNo ratings yet
- Neurotransmitter Dalam Fisiologi Saraf Otonom: Iwan Dwi Cahyono, Himawan Sasongko, Aria Dian PrimatikaDocument14 pagesNeurotransmitter Dalam Fisiologi Saraf Otonom: Iwan Dwi Cahyono, Himawan Sasongko, Aria Dian PrimatikaardianNo ratings yet
- Jcen 22 2 78Document7 pagesJcen 22 2 78Aik NoeraNo ratings yet
- The Holistic Approach In: 2 AnnouncementDocument1 pageThe Holistic Approach In: 2 AnnouncementAik NoeraNo ratings yet
- The Impact of Age On CognitionDocument11 pagesThe Impact of Age On CognitionDara Agusti MaulidyaNo ratings yet
- 100 Questions in Cardiology-, PDFDocument241 pages100 Questions in Cardiology-, PDFditairinaNo ratings yet
- The Role of Acetaminophen and Geohelminth Infection On The Incidence of Wheeze and EczemaDocument6 pagesThe Role of Acetaminophen and Geohelminth Infection On The Incidence of Wheeze and EczemaAik NoeraNo ratings yet
- Pohl 2016Document9 pagesPohl 2016Aik NoeraNo ratings yet
- Acute Disseminated Encephalomyelitis in 228 Patients: A Retrospective, Multicenter US StudyDocument10 pagesAcute Disseminated Encephalomyelitis in 228 Patients: A Retrospective, Multicenter US StudyAik NoeraNo ratings yet
- Case Report Rabies BARUDocument14 pagesCase Report Rabies BARUAik NoeraNo ratings yet
- Intracranial HaemorrhageDocument12 pagesIntracranial HaemorrhageAik NoeraNo ratings yet
- Efficacy of Hyperventilation, Blood Pressure Elevation, and Metabolic Suppression Therapy in Controlling Intracranial Pressure After Head InjuryDocument9 pagesEfficacy of Hyperventilation, Blood Pressure Elevation, and Metabolic Suppression Therapy in Controlling Intracranial Pressure After Head InjuryAik NoeraNo ratings yet
- Falciparum: Misdiagnosis of An Imported Case of Malaria Caused by PlasmodiumDocument3 pagesFalciparum: Misdiagnosis of An Imported Case of Malaria Caused by PlasmodiumAik NoeraNo ratings yet
- Documents StackDocument1 pageDocuments StackDan MNo ratings yet
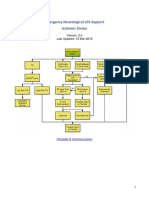
- Emergency Neurological Life Support Ischemic Stroke: Last Updated: 19-Mar-2016Document22 pagesEmergency Neurological Life Support Ischemic Stroke: Last Updated: 19-Mar-2016Aik NoeraNo ratings yet
- Journal Cerebellar AstrocytomaDocument18 pagesJournal Cerebellar AstrocytomaAik NoeraNo ratings yet
- Predicting Outcome After Traumatic Brain InjuryDocument11 pagesPredicting Outcome After Traumatic Brain InjuryAik NoeraNo ratings yet
- Toxic FurDocument8 pagesToxic FurOur Compass100% (2)
- Acute Myelogenous LeukemiaDocument8 pagesAcute Myelogenous LeukemiaAik NoeraNo ratings yet
- Fur - An Environmental Nightmare: Water & Air PollutionDocument3 pagesFur - An Environmental Nightmare: Water & Air PollutionAik NoeraNo ratings yet
- LO Radiologic Pattern of BronchopneumoniaDocument1 pageLO Radiologic Pattern of BronchopneumoniaAik NoeraNo ratings yet
- LINAC Radiosurgery and Radiotherapy Treatment of Acoustic NeuromasDocument21 pagesLINAC Radiosurgery and Radiotherapy Treatment of Acoustic NeuromasAik NoeraNo ratings yet
- Schedule SympoDocument6 pagesSchedule SympoAik NoeraNo ratings yet
- Less - Known Botanical CosmeceuticalsDocument13 pagesLess - Known Botanical CosmeceuticalsSandra Marcela Pabón100% (1)
- Notes For PediatricsDocument38 pagesNotes For PediatricsadamsamillionNo ratings yet
- Neuromuscular Junction Blocking AgentsDocument9 pagesNeuromuscular Junction Blocking AgentsSyvNo ratings yet
- Papillary CarcinomaDocument7 pagesPapillary Carcinomarazik89No ratings yet
- Disseminated Intravascular Coagulation With PathophysiologyDocument18 pagesDisseminated Intravascular Coagulation With Pathophysiologymabec pagaduan100% (6)
- Oro-Antral CommunicationDocument65 pagesOro-Antral CommunicationNadila RNo ratings yet
- Childhood TB MCQ QuizDocument21 pagesChildhood TB MCQ QuizSaya Menang75% (4)
- Anesthesia in A Patient With Reactive Airways Case FileDocument2 pagesAnesthesia in A Patient With Reactive Airways Case Filehttps://medical-phd.blogspot.comNo ratings yet
- Anemia of Chronic Disease - Inflammation - UpToDateDocument36 pagesAnemia of Chronic Disease - Inflammation - UpToDateDomenica MurilloNo ratings yet
- ArthritisDocument18 pagesArthritisGEETA MOHAN100% (1)
- Cancer Pulmonar URPDocument76 pagesCancer Pulmonar URPLISBETH ONSIHUAY CASTRONo ratings yet
- Handbook of AnesthesiologyDocument176 pagesHandbook of AnesthesiologyarmelzahfauziNo ratings yet
- Topnotch Ent Supplement Handout Updated April 2016pdf PDFDocument15 pagesTopnotch Ent Supplement Handout Updated April 2016pdf PDFKenneth NuñezNo ratings yet
- The Top 300 Medicines of 2020Document9 pagesThe Top 300 Medicines of 2020Bonnie DebbarmaNo ratings yet
- Association of Vaginal Infections in Preterm Labour: Srilakshmi Yarlagadda, Sajana G., Prasuna J. L. NarraDocument6 pagesAssociation of Vaginal Infections in Preterm Labour: Srilakshmi Yarlagadda, Sajana G., Prasuna J. L. NarraNurRahMatNo ratings yet
- Solitary Thyroid NoduleDocument24 pagesSolitary Thyroid Nodulenontapat paesarochNo ratings yet
- Krok 2 2002-2003 TherapyDocument41 pagesKrok 2 2002-2003 TherapyAli ZeeshanNo ratings yet
- Dr. F. Lings Otolaryngology NotesDocument1,417 pagesDr. F. Lings Otolaryngology NotesAbouzr Mohammed Elsaid100% (3)
- MS CourseTask10Document2 pagesMS CourseTask10Aria67% (3)
- Daily Opd Summary 2023Document26 pagesDaily Opd Summary 2023JOMELYN MIELNo ratings yet
- Kasus Nyeri DadaDocument19 pagesKasus Nyeri DadaMuhammad Fachrurozi SidiqNo ratings yet
- Hipodens Non Enhancing Brain LesionDocument7 pagesHipodens Non Enhancing Brain LesionJuwita Valen RamadhanniaNo ratings yet
- Transient Tachypnea of The NewbornDocument53 pagesTransient Tachypnea of The NewbornAyah PaasaNo ratings yet
- Harrison - S Principles of Internal Medicine - Self PDFDocument27 pagesHarrison - S Principles of Internal Medicine - Self PDFSydrex Sarmiento0% (1)
- Science 9 - 1ST Monthly TestDocument2 pagesScience 9 - 1ST Monthly TestMaria JocosaNo ratings yet
- AFEM Approach To Abdominal Pain in AdultsDocument53 pagesAFEM Approach To Abdominal Pain in AdultsSaktai DiyamiNo ratings yet
- My SeminarDocument12 pagesMy SeminarAdeleye SeunNo ratings yet
- CU5Document13 pagesCU5kuu faal100% (3)
- Journal OsteochondromaDocument14 pagesJournal OsteochondromaAnggi CalapiNo ratings yet
- OPHTHALDocument8 pagesOPHTHALVarun ChandiramaniNo ratings yet