You might also like
- Breast Exam Guide for Medical StudentsDocument11 pagesBreast Exam Guide for Medical Studentscharlyn206No ratings yet
- Breast Exam: A Systematic ApproachDocument3 pagesBreast Exam: A Systematic ApproachBearaphNo ratings yet
- Please Read 1F Simulations Compilations 1Document36 pagesPlease Read 1F Simulations Compilations 1mendozakaceeyNo ratings yet
- bmj00069 0040Document3 pagesbmj00069 0040hanh minhNo ratings yet
- Breast and Axillae AssessmentDocument146 pagesBreast and Axillae AssessmentFaith madayag100% (2)
- Module 6 Breast Axilla Assessment-Edited 0 0Document13 pagesModule 6 Breast Axilla Assessment-Edited 0 0Laila PasiganNo ratings yet
- FMcase 1Document24 pagesFMcase 1Ryan Townsend100% (2)
- Assessment of The Breast: Jonalyn Sotero Esco RN., MANDocument41 pagesAssessment of The Breast: Jonalyn Sotero Esco RN., MANVan MaverickNo ratings yet
- BreastDocument3 pagesBreastUriel NateNo ratings yet
- Breast Examination - OSCE Guide - Geeky MedicsDocument6 pagesBreast Examination - OSCE Guide - Geeky MedicsJahangir AlamNo ratings yet
- Breast Assessment: Preparing The ClientDocument5 pagesBreast Assessment: Preparing The Clientshannon c. lewisNo ratings yet
- 04 New Obstetric ExaminationDocument44 pages04 New Obstetric Examinationfranny90No ratings yet
- CamaristaCM - BreastCancer (Questions and Answers)Document4 pagesCamaristaCM - BreastCancer (Questions and Answers)Coleen Mae CamaristaNo ratings yet
- Labor Process and Nursing Care GuideDocument9 pagesLabor Process and Nursing Care GuideMary Florence VelardeNo ratings yet
- What Are The Physical Examination On Monitoring The Labour?Document2 pagesWhat Are The Physical Examination On Monitoring The Labour?Nurfi Resni Fitra RamdaNo ratings yet
- Health Talk On BSFDocument11 pagesHealth Talk On BSFjyoti singh100% (1)
- STUDENT COPY Assessment of Breast and AxillaeDocument57 pagesSTUDENT COPY Assessment of Breast and AxillaeRosette Malenab de AsisNo ratings yet
- Colposcopy CourseDocument50 pagesColposcopy CourseNam Le100% (1)
- Nursing Care During LaborDocument12 pagesNursing Care During LaborJulianne B. Dela CruzNo ratings yet
- Breast Self Examination: o o o oDocument3 pagesBreast Self Examination: o o o oDalvin Roy WongNo ratings yet
- NCM 112 Skills Lab Cellular AberrationDocument10 pagesNCM 112 Skills Lab Cellular AberrationMeryville JacildoNo ratings yet
- Breast and Axillae SynthesisDocument3 pagesBreast and Axillae SynthesisEya BaldostamonNo ratings yet
- Amniocentrices (From The Greek Amnion For "Sac" and KenteDocument5 pagesAmniocentrices (From The Greek Amnion For "Sac" and KenteJohn Paolo Tamayo OrioNo ratings yet
- Breast Anatomy and Examination GuideDocument11 pagesBreast Anatomy and Examination GuideKrishna Faith P. DelaraNo ratings yet
- UNIT-VII Assessment of the Breast and AxillaDocument30 pagesUNIT-VII Assessment of the Breast and Axillaraima ayazNo ratings yet
- Prenatal Care: Understanding Pelvic Exams and Fetal AssessmentDocument9 pagesPrenatal Care: Understanding Pelvic Exams and Fetal AssessmentBinita ShakyaNo ratings yet
- Examination of The BreastDocument2 pagesExamination of The BreastAufi FillaNo ratings yet
- 175 Ultrasound in Pregnancy PDFDocument16 pages175 Ultrasound in Pregnancy PDFNestor FerrerNo ratings yet
- Breast Self ExaminationDocument4 pagesBreast Self ExaminationSagar HanamasagarNo ratings yet
- Retensio PlasentaDocument3 pagesRetensio PlasentaAnonymous c4GVTgkvNo ratings yet
- National College of Nursing: Procedure ONDocument6 pagesNational College of Nursing: Procedure ONSumit Yadav100% (1)
- A Cog Practice Bulletin 175 Ultrasound in PregnancyDocument16 pagesA Cog Practice Bulletin 175 Ultrasound in Pregnancyansel7No ratings yet
- Ring Pessary Effective For Advanced POPDocument8 pagesRing Pessary Effective For Advanced POPputri vinia /ilove cuteNo ratings yet
- 1 GYNE 3 - History, PE, Prevention Interaction of Disease and PhysiologyDocument6 pages1 GYNE 3 - History, PE, Prevention Interaction of Disease and PhysiologyIrene FranzNo ratings yet
- Health-Assessment-Breast-and-AxillaDocument27 pagesHealth-Assessment-Breast-and-AxillaMary Jane M. MorenoNo ratings yet
- Definition: Related Diagnostic TestsDocument8 pagesDefinition: Related Diagnostic TestsQuinn Xylon VillanuevaNo ratings yet
- Breast ModuleDocument2 pagesBreast ModuleDasha Vee100% (1)
- Normal LaborDocument27 pagesNormal LaborRamil BonifacioNo ratings yet
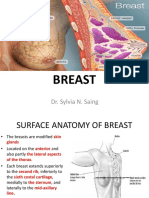
- Breast: Dr. Sylvia N. SaingDocument26 pagesBreast: Dr. Sylvia N. SaingRichard 151289100% (1)
- Emergency Nursing ChecklistDocument6 pagesEmergency Nursing ChecklistMark DomingoNo ratings yet
- Understanding Breast DisordersDocument13 pagesUnderstanding Breast DisordersCalimlim KimNo ratings yet
- Full Term Newborn Delivery Stages and IndicationsDocument34 pagesFull Term Newborn Delivery Stages and IndicationsAaliyaan KhanNo ratings yet
- SDP Vs AFIDocument5 pagesSDP Vs AFINuzma AnbiaNo ratings yet
- How To Measure Cervical Length: Karl Oliver Kagan and Jiri SonekDocument14 pagesHow To Measure Cervical Length: Karl Oliver Kagan and Jiri SoneknidoNo ratings yet
- Apple Peel Small Bowel, A Review of Four Cases: Surgical and Radiographic AspectsDocument8 pagesApple Peel Small Bowel, A Review of Four Cases: Surgical and Radiographic AspectsraecmyNo ratings yet
- Cord Clamping - Physiologic ApproachDocument13 pagesCord Clamping - Physiologic ApproachravyryNo ratings yet
- Leopold's maneuvers determine fetal positionDocument39 pagesLeopold's maneuvers determine fetal positionJayrelle D. SafranNo ratings yet
- Hysteroscopic Differences in Blighted Ovum and Viable PregnancyDocument5 pagesHysteroscopic Differences in Blighted Ovum and Viable PregnancyAgudisarfNo ratings yet
- Heimlich Maneuver PDFDocument7 pagesHeimlich Maneuver PDFMark DomingoNo ratings yet
- Screening of Breast CancerDocument19 pagesScreening of Breast CancerIncredible DivineNo ratings yet
- Self Breast ExaminationDocument11 pagesSelf Breast ExaminationJairene Dave Martinez Cambalon100% (2)
- Teach MeDocument5 pagesTeach Medryasmin95No ratings yet
- Back Et Al - 2017 - Emergent Ultrasound Evaluation of The Pediatric Female PelvisDocument10 pagesBack Et Al - 2017 - Emergent Ultrasound Evaluation of The Pediatric Female PelvisBerry BancinNo ratings yet
- Placenta AccretaDocument5 pagesPlacenta AccretaF3rcitaNo ratings yet
- Effectiveness of Delayed Absorbable Monofila - 2014 - Taiwanese Journal of ObsteDocument3 pagesEffectiveness of Delayed Absorbable Monofila - 2014 - Taiwanese Journal of ObsteSami KahtaniNo ratings yet
- Cervical incompetence diagnosis and managementDocument40 pagesCervical incompetence diagnosis and managementCristian AlbuNo ratings yet
- Physiology of Pregnancy. Perinatal Care of Fetus. Methods of Examination of Pregnant Women.Document15 pagesPhysiology of Pregnancy. Perinatal Care of Fetus. Methods of Examination of Pregnant Women.Erwin SiahaanNo ratings yet
- Breast and AxillaeDocument4 pagesBreast and AxillaeDanesse CapitlyNo ratings yet
- Dental Management of the Pregnant PatientFrom EverandDental Management of the Pregnant PatientChristos A. SkouterisNo ratings yet
- History and Physical Assessment of the Integumentary SystemDocument84 pagesHistory and Physical Assessment of the Integumentary SystemNilakshi Barik MandalNo ratings yet
- Mentalhealthactppt 160524140542Document34 pagesMentalhealthactppt 160524140542Nilakshi Barik MandalNo ratings yet
- Pain AssessmentDocument12 pagesPain AssessmentFadhilah Asyifa DewantiNo ratings yet
- Pain Scale and Its Types: Quratulain Mughal Batch Iv Doctor of Physical Therapy Isra UniversityDocument11 pagesPain Scale and Its Types: Quratulain Mughal Batch Iv Doctor of Physical Therapy Isra UniversityNilakshi Barik MandalNo ratings yet
- Birth Injuries in Neonates: Pediatrics in Review November 2016Document15 pagesBirth Injuries in Neonates: Pediatrics in Review November 2016Nilakshi Barik MandalNo ratings yet
- Presented By: Sandeep Yadav M.Sc. (N) 1 Year KGMU LucknowDocument93 pagesPresented By: Sandeep Yadav M.Sc. (N) 1 Year KGMU LucknowNilakshi Barik MandalNo ratings yet
- Pptforphysical 130322221925 Phpapp01Document117 pagesPptforphysical 130322221925 Phpapp01Karen Mae Santiago AlcantaraNo ratings yet
- Clinical Examination: Plan of Conduction & Scheme of RecordingDocument112 pagesClinical Examination: Plan of Conduction & Scheme of RecordingNilakshi Barik MandalNo ratings yet
- New Format With Correct LayoutDocument3 pagesNew Format With Correct LayoutNilakshi Barik MandalNo ratings yet
- Gate Control TheoryDocument6 pagesGate Control TheoryNilakshi Barik MandalNo ratings yet
- Physical Examination: Presented To Mrs. Nisha Mane Assistant Professor D.Y.P.S.O.NDocument41 pagesPhysical Examination: Presented To Mrs. Nisha Mane Assistant Professor D.Y.P.S.O.NNilakshi Barik MandalNo ratings yet
- Clinical Examination: Plan of Conduction & Scheme of RecordingDocument112 pagesClinical Examination: Plan of Conduction & Scheme of RecordingNilakshi Barik MandalNo ratings yet
- Efficacy, Safety and Fertility Return of Implanon Contraceptive ImplantDocument4 pagesEfficacy, Safety and Fertility Return of Implanon Contraceptive ImplantNilakshi Barik MandalNo ratings yet
- Monica Rita Hendricks PDFDocument151 pagesMonica Rita Hendricks PDFNilakshi Barik MandalNo ratings yet
- Cardio Pulmonary Resuscitation Adult & Paediatric Definition of Cardiac ArrestDocument8 pagesCardio Pulmonary Resuscitation Adult & Paediatric Definition of Cardiac ArrestNilakshi Barik Mandal0% (1)
- Ijshr0038 PDFDocument9 pagesIjshr0038 PDFNilakshi Barik MandalNo ratings yet
- Medical Surgical Nursing AssignmentDocument166 pagesMedical Surgical Nursing AssignmentSonali Sengar0% (1)
- CamScanner Document ScansDocument48 pagesCamScanner Document ScansNilakshi Barik MandalNo ratings yet
- Ms. Nilakshi Barik Mandal Lecturer Oxford College of Nursing SciencesDocument11 pagesMs. Nilakshi Barik Mandal Lecturer Oxford College of Nursing SciencesNilakshi Barik MandalNo ratings yet
- Oral Hygiene: Mrs - NilakshiDocument11 pagesOral Hygiene: Mrs - NilakshiNilakshi Barik MandalNo ratings yet
- History and Physical Assessment of the Integumentary SystemDocument84 pagesHistory and Physical Assessment of the Integumentary SystemNilakshi Barik MandalNo ratings yet
- Pain Manage Me NT: Ms - Nilakshi Barik MandalDocument14 pagesPain Manage Me NT: Ms - Nilakshi Barik MandalNilakshi Barik MandalNo ratings yet
- PreconceptionDocument29 pagesPreconceptionNilakshi Barik MandalNo ratings yet
- Gate Contro L Theory: Ms - Nilakshi Barik MandalDocument6 pagesGate Contro L Theory: Ms - Nilakshi Barik MandalNilakshi Barik MandalNo ratings yet
- Fetal SkullDocument5 pagesFetal SkullNilakshi Barik MandalNo ratings yet
- Ms. Nilakshi Barik Mandal Lecturer Oxford College of Nursing SciencesDocument11 pagesMs. Nilakshi Barik Mandal Lecturer Oxford College of Nursing SciencesNilakshi Barik MandalNo ratings yet
- Female PelvisDocument7 pagesFemale PelvisNilakshi Barik MandalNo ratings yet
- Nutrition Course PlanDocument7 pagesNutrition Course PlanNilakshi Barik MandalNo ratings yet
- BSc Nursing Unit Plan Nutrition 2019-20Document1 pageBSc Nursing Unit Plan Nutrition 2019-20Nilakshi Barik MandalNo ratings yet
- BreastDocument2 pagesBreastAdrian SantosNo ratings yet
- Axilla Boundaries and ContentDocument47 pagesAxilla Boundaries and Contentchzaheer72No ratings yet
- Axila: Mesole Samuel Bolaji (B.SC M.SC PHD (In-View) ) Course: Anatomy Course Code: Han 3010Document15 pagesAxila: Mesole Samuel Bolaji (B.SC M.SC PHD (In-View) ) Course: Anatomy Course Code: Han 3010Tinotenda KarumeNo ratings yet
- Body LinesDocument1 pageBody LinesAnonymous OAEuN9NE1sNo ratings yet
- 5 Axillary and Epitrochlear Lymph Node Dissection For MelanomaDocument11 pages5 Axillary and Epitrochlear Lymph Node Dissection For MelanomajuanrangoneNo ratings yet
- Surgical Anatomy of The Breast T-HAZEM - CompressedDocument28 pagesSurgical Anatomy of The Breast T-HAZEM - CompressedmohamedhazemelfollNo ratings yet
- Download ebook Selective Anatomy Prep Manual For Undergraduates Vol 1 2E Pdf full chapter pdfDocument67 pagesDownload ebook Selective Anatomy Prep Manual For Undergraduates Vol 1 2E Pdf full chapter pdfcharles.brewer536100% (24)
- Lecture FiveDocument35 pagesLecture FivePiniel MatewosNo ratings yet
- Tilak 2009/2010 ZimaDocument33 pagesTilak 2009/2010 Zima4outdoor.plNo ratings yet
- Breast Exam Detailed Skill SheetDocument1 pageBreast Exam Detailed Skill SheetMuhammed ElgasimNo ratings yet
- Understanding The SelfDocument24 pagesUnderstanding The Selfelvie dijanNo ratings yet
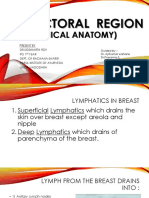
- Lymphatics of the Breast and Clinical Anatomy (39Document28 pagesLymphatics of the Breast and Clinical Anatomy (39SIDDHRATH ROYNo ratings yet
- Bathing An Adult ClientDocument8 pagesBathing An Adult ClientXoisagesNo ratings yet
- Hygiene and Health in IslamDocument37 pagesHygiene and Health in Islamالمدینہ اسلامک ریسرچ سینٹر کراچی100% (1)
- Breast AssessmentDocument3 pagesBreast Assessmenttaé pNo ratings yet
- Breast ExaminationDocument3 pagesBreast ExaminationShum Wing Hei JoanneNo ratings yet
- It Is A Pyramid-Shaped Space Between The Upper Part of The Arm and The Side of The ChestDocument25 pagesIt Is A Pyramid-Shaped Space Between The Upper Part of The Arm and The Side of The ChestMoaiadHusseinNo ratings yet
- Nine Locks - of The Human BodyDocument9 pagesNine Locks - of The Human BodyKalyan PingaliNo ratings yet
- Breast and Lymphatic SysytemDocument3 pagesBreast and Lymphatic SysytemJL RebeseNo ratings yet
- AXILLADocument8 pagesAXILLAImmunity RABOTANo ratings yet
- Locomotor Module Guide by MedAngleDocument15 pagesLocomotor Module Guide by MedAnglefqtyd8ypsjNo ratings yet
- CriolipóliseTM 908A新Document25 pagesCriolipóliseTM 908A新Cyber100% (2)
- Axilla and Cubital Fossa (AYY)Document19 pagesAxilla and Cubital Fossa (AYY)LeeMinhoNo ratings yet
- RTOG Breast Cancer Atlas For Radiation Therapy PlanningDocument71 pagesRTOG Breast Cancer Atlas For Radiation Therapy Planningdoctordoctor80No ratings yet
- The Axilla: Norah AlmudawiDocument14 pagesThe Axilla: Norah AlmudawiF-med440 imamNo ratings yet
- 4 AxillaDocument31 pages4 AxillaRamesh KumarNo ratings yet
- Breast (Mamma)Document69 pagesBreast (Mamma)Wealth AbiodunNo ratings yet
- Tanner Stage Calculator For BoysDocument11 pagesTanner Stage Calculator For BoysFootball Club Allianz0% (1)
- Breast and Axilla 2Document17 pagesBreast and Axilla 2Justine Nyangaresi100% (1)
- Breast Cancer Atlas For RT PlanningDocument26 pagesBreast Cancer Atlas For RT PlanningZuriNo ratings yet