You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- A Christian Perspective of Acupuncture: A Research Paper Submitted To DR Keith WarringtonDocument33 pagesA Christian Perspective of Acupuncture: A Research Paper Submitted To DR Keith WarringtonEric TNo ratings yet
- 14 Male Sexual Dysfunction LR1Document38 pages14 Male Sexual Dysfunction LR1Nur AnindyaNo ratings yet
- 2021 - WHO Key Technical Issues of Herbal Medicines With Reference To Interaction With Other Medicines With Others MedicinesDocument85 pages2021 - WHO Key Technical Issues of Herbal Medicines With Reference To Interaction With Other Medicines With Others MedicinesGabriela AlmeidaNo ratings yet
- 2008 - Neurofibromatoses - KaufmnanDocument203 pages2008 - Neurofibromatoses - KaufmnanPablo Antonio Antonio100% (1)
- Usg TemplatesDocument53 pagesUsg Templatessubha1b9448No ratings yet
- Nursing Care Plan For HemorrhoidsDocument3 pagesNursing Care Plan For HemorrhoidsFaith Marfil100% (2)
- CVA Case PresentationDocument25 pagesCVA Case PresentationChucky VergaraNo ratings yet
- J Jor 2020 03 058Document42 pagesJ Jor 2020 03 058Luis HerreraNo ratings yet
- Clinical Biomechanics: Thomas J. Kibsgård, Olav Røise, Bengt Sturesson, Stephan M. Röhrl, Britt StugeDocument6 pagesClinical Biomechanics: Thomas J. Kibsgård, Olav Røise, Bengt Sturesson, Stephan M. Röhrl, Britt StugeLuis HerreraNo ratings yet
- Contemporary Clinical Trials CommunicationsDocument8 pagesContemporary Clinical Trials CommunicationsLuis HerreraNo ratings yet
- Síntomas en Las Piernas Asociados Con El Trastorno de La Articulación Sacroilíaca y El Dolor RelacionadoDocument4 pagesSíntomas en Las Piernas Asociados Con El Trastorno de La Articulación Sacroilíaca y El Dolor RelacionadoLuis HerreraNo ratings yet
- Spondylosis, Cervical and LumbarDocument1 pageSpondylosis, Cervical and LumbarLuis HerreraNo ratings yet
- Sacroiliac Joint PainDocument5 pagesSacroiliac Joint PainLuis HerreraNo ratings yet
- Escala de Diagnóstico (SI5) de Disfunción de La Articulación Sacroiliaca Estudio PilotoDocument8 pagesEscala de Diagnóstico (SI5) de Disfunción de La Articulación Sacroiliaca Estudio PilotoLuis HerreraNo ratings yet
- CF120 Plus PDFDocument2 pagesCF120 Plus PDFLuis HerreraNo ratings yet
- Grade II Spondylolisthesis Reverse Bohlman Procedure With TransdiscalDocument9 pagesGrade II Spondylolisthesis Reverse Bohlman Procedure With TransdiscalLuis HerreraNo ratings yet
- V8 GTS Product Sheet PDFDocument2 pagesV8 GTS Product Sheet PDFLuis HerreraNo ratings yet
- A Guide: Christian Medical CollegeDocument75 pagesA Guide: Christian Medical CollegeSanjay Kumar SekhardeoNo ratings yet
- Tracheostomy Care - An Evidence-Based Guide - American Nurse TodayDocument4 pagesTracheostomy Care - An Evidence-Based Guide - American Nurse TodayZulaikah Nur IstiqomahNo ratings yet
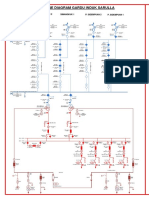
- SLD Gi SarullaDocument1 pageSLD Gi SarullasacilatwaeNo ratings yet
- Cutaneous Angiosarcoma: The Role of Dermoscopy To Reduce The Risk of A Delayed DiagnosisDocument2 pagesCutaneous Angiosarcoma: The Role of Dermoscopy To Reduce The Risk of A Delayed DiagnosisJosé JúniorNo ratings yet
- Specialised Traditions of Knowledge and Health Delivery-1Document40 pagesSpecialised Traditions of Knowledge and Health Delivery-1Theophilus BaidooNo ratings yet
- Buscopan-Drug StudyDocument2 pagesBuscopan-Drug StudyJoan QuebalayanNo ratings yet
- Welcome To The University of Göttingen: Guide For International ResearchersDocument79 pagesWelcome To The University of Göttingen: Guide For International Researchersdapias09No ratings yet
- Treatment For Gangrene A. DryDocument2 pagesTreatment For Gangrene A. DryKey LomonovNo ratings yet
- A Simplified Appendicitis ScoreDocument6 pagesA Simplified Appendicitis ScoreDenny TombengNo ratings yet
- Notes: Last Name First Name Middle Name Age Sex Address Contact NODocument108 pagesNotes: Last Name First Name Middle Name Age Sex Address Contact NOSample BakeshopNo ratings yet
- Metamizole A Review Profile of A Well Known Forgotten Drug Part II Clinical Profile PDFDocument16 pagesMetamizole A Review Profile of A Well Known Forgotten Drug Part II Clinical Profile PDFcristirusu23No ratings yet
- NCP AnxietyDocument1 pageNCP AnxietyGrace MellaineNo ratings yet
- Bahan CA 1Document11 pagesBahan CA 1fk unswagatiNo ratings yet
- Bolgan DR - Ssa Loretta-Meccanismo D'induzione Del Danno Da Vaccini A mRNADocument34 pagesBolgan DR - Ssa Loretta-Meccanismo D'induzione Del Danno Da Vaccini A mRNAgiordana214No ratings yet
- Acute Fatty Liver of Pregnancy - NEJMDocument2 pagesAcute Fatty Liver of Pregnancy - NEJMJing CruzNo ratings yet
- Benign Paroxysmal Positional VertigoDocument8 pagesBenign Paroxysmal Positional VertigoSubynk RidwanNo ratings yet
- P1 Referral Letter: "Dhanwantri" ModuleDocument5 pagesP1 Referral Letter: "Dhanwantri" Modulerajput sanjeevNo ratings yet
- Mebo OintmentDocument17 pagesMebo OintmentFarahNo ratings yet
- Fmge Important TopicsDocument33 pagesFmge Important Topicsdocprash100% (1)
- Non Hodgkin Lymphoma in ChildrenDocument4 pagesNon Hodgkin Lymphoma in ChildrenMilzan MurtadhaNo ratings yet
- Pizotifen To Prevent Migraine Headaches 1Document2 pagesPizotifen To Prevent Migraine Headaches 1William ImpNo ratings yet
- Periodic Health Examination national guideline وقايهDocument56 pagesPeriodic Health Examination national guideline وقايهMohammed AbdulbaqiNo ratings yet
- Chapter 2 SolutionDocument3 pagesChapter 2 SolutionAdam EdNo ratings yet