You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5819)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- Ati Maternal Newborn Proctored Exam 2023 With NGN Questions and Answers & Rationales (Verified Full Exam)Document6 pagesAti Maternal Newborn Proctored Exam 2023 With NGN Questions and Answers & Rationales (Verified Full Exam)marcuskenyatta275No ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- COVID 19 Guideline To Resume Paediatric Dental Services in MalaysiaDocument29 pagesCOVID 19 Guideline To Resume Paediatric Dental Services in MalaysiaEnrita DianNo ratings yet
- Epidemiologie Study of Idiopathie Enamel Hypomineralization in Permanent Teeth of Swedish ChildrenDocument8 pagesEpidemiologie Study of Idiopathie Enamel Hypomineralization in Permanent Teeth of Swedish ChildrenEnrita DianNo ratings yet
- Avocet B: Knit in - Skill LevelDocument3 pagesAvocet B: Knit in - Skill LevelEnrita DianNo ratings yet
- Knit Top Down PulloverDocument3 pagesKnit Top Down PulloverEnrita DianNo ratings yet
- P Acutepainmgmt PDFDocument3 pagesP Acutepainmgmt PDFEnrita DianNo ratings yet
- Pak0425 012327MDocument2 pagesPak0425 012327MEnrita DianNo ratings yet
- Behavior Guidance For The Pediatric Dental Patient: Latest RevisionDocument14 pagesBehavior Guidance For The Pediatric Dental Patient: Latest RevisionEnrita DianNo ratings yet
- Materials 01 04Document20 pagesMaterials 01 04mysterioushumaneNo ratings yet
- Syllabus - MCH Course 2019 FINAL 1 1Document8 pagesSyllabus - MCH Course 2019 FINAL 1 1Nur Fatima SanaaniNo ratings yet
- MODULE 7 PART 1 SEXUAL SELF ViBe 2nd TERM 2022 PDFDocument38 pagesMODULE 7 PART 1 SEXUAL SELF ViBe 2nd TERM 2022 PDFGILBERT BANTANo ratings yet
- My ThesisDocument144 pagesMy ThesisHendroNo ratings yet
- HydroxychloroquineDocument4 pagesHydroxychloroquineashruNo ratings yet
- Fear of Childbirth: Mothers' Experiences of Team-Midwifery Care - A Follow-Up StudyDocument8 pagesFear of Childbirth: Mothers' Experiences of Team-Midwifery Care - A Follow-Up Studyyayusuk desamtaNo ratings yet
- Management of Infants BornDocument6 pagesManagement of Infants BornDiana FlorezNo ratings yet
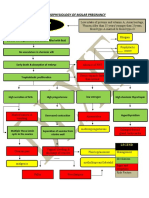
- Partial Mole or Complete Mole: Pathophysiology of Molar PregnancyDocument1 pagePartial Mole or Complete Mole: Pathophysiology of Molar PregnancyKristian Karl Bautista Kiw-isNo ratings yet
- Emedica MRCGP AKT Curriculum ChecklistDocument42 pagesEmedica MRCGP AKT Curriculum ChecklistSana Mustafa100% (1)
- Project Augustine AbisolaDocument59 pagesProject Augustine AbisolaRoseline Omoare100% (1)
- Tilly's Care StudyDocument105 pagesTilly's Care StudyRichmond AnaneNo ratings yet
- 'Dokumen - Tips Kode Icd ObgynDocument4 pages'Dokumen - Tips Kode Icd ObgynFebriolla SafitryNo ratings yet
- Test Bank For Larsens Human Embryology 5th Edition Gary Schoenwolf Steven Bleyl Philip Brauer Philippa Francis WestDocument3 pagesTest Bank For Larsens Human Embryology 5th Edition Gary Schoenwolf Steven Bleyl Philip Brauer Philippa Francis WestPauline Chavez100% (35)
- CSYah Tambo 2018 JIPHDocument12 pagesCSYah Tambo 2018 JIPHadhiniNo ratings yet
- The Process of ReproductionDocument4 pagesThe Process of ReproductionIvan BixenmanNo ratings yet
- Disrupting The Pathways of Social Determinants ofDocument10 pagesDisrupting The Pathways of Social Determinants ofIGA ABRAHAMNo ratings yet
- Nintynine Srinidhi r2 HealthcareDocument8 pagesNintynine Srinidhi r2 Healthcaresri nidhiNo ratings yet
- Presentation 1Document30 pagesPresentation 1John Darvin TanNo ratings yet
- Perineal LacerationDocument16 pagesPerineal Lacerationbasman1212No ratings yet
- Rubella On 22-2-2018Document48 pagesRubella On 22-2-2018farigNo ratings yet
- Aqa Combisci Bio Paper 2 1650625 PDFDocument6 pagesAqa Combisci Bio Paper 2 1650625 PDFCuthbert YedwaNo ratings yet
- ART20176809Document5 pagesART20176809dkhatri01No ratings yet
- Currens Math For Meds Dosages and Solutions 11th Edition Curren Test BankDocument36 pagesCurrens Math For Meds Dosages and Solutions 11th Edition Curren Test Banksynechia.goblinqrs4v100% (33)
- Swinging, Sucking (5S'S) Terhadap Skala Nyeri DanDocument7 pagesSwinging, Sucking (5S'S) Terhadap Skala Nyeri DanpetronelaNo ratings yet
- Hemolytic Disease of The NewbornDocument43 pagesHemolytic Disease of The Newbornalibayaty1No ratings yet
- Science Module For Grade 10: Guagua National Colleges, Inc. Guagua, PampangaDocument62 pagesScience Module For Grade 10: Guagua National Colleges, Inc. Guagua, PampangaNorman Punla SantosNo ratings yet
- Fetal and Neonatal PhysiologyDocument7 pagesFetal and Neonatal PhysiologyGabby ElardoNo ratings yet
- Premium Policy Wording Revolut Payments UAB en 05.03.2021 PDFDocument54 pagesPremium Policy Wording Revolut Payments UAB en 05.03.2021 PDFlfsab 1171No ratings yet
- Pathomecanik Sij ProblemDocument10 pagesPathomecanik Sij ProblemDonny HendrawanNo ratings yet