You might also like
- Iron-Restricted Anemias: Causes and TreatmentDocument7 pagesIron-Restricted Anemias: Causes and TreatmentAlanah JaneNo ratings yet
- Water Soluble Vitamins: Folic Acid and Vitamin B12Document85 pagesWater Soluble Vitamins: Folic Acid and Vitamin B12amiNo ratings yet
- Deficiency of Iron: First Semester A.Y. 2015-2016Document8 pagesDeficiency of Iron: First Semester A.Y. 2015-2016emely p. tangoNo ratings yet
- Blood DisordersDocument3 pagesBlood DisorderswastiNo ratings yet
- Chapter 20 HemaDocument9 pagesChapter 20 HemaEMETERIO TUTOR IIINo ratings yet
- Blood Loss: Acute Chronic Inadequate Production of Normal Blood CellsDocument11 pagesBlood Loss: Acute Chronic Inadequate Production of Normal Blood CellsSheila Amor BodegasNo ratings yet
- Megaloblastic AnemiaDocument7 pagesMegaloblastic AnemiaEmilio AldreteNo ratings yet
- 6 Iron Deficiency AnemiaDocument3 pages6 Iron Deficiency AnemiaMelita SabellinaNo ratings yet
- Disorders of Iron Kinetics and Heme Metabolism ConceptsDocument12 pagesDisorders of Iron Kinetics and Heme Metabolism ConceptsJoanne JardinNo ratings yet
- What Causes Iron-Deficiency Anemia?Document2 pagesWhat Causes Iron-Deficiency Anemia?AidaDesNo ratings yet
- IRON DEFICIENCY ANEMIA ETIOLOGY AND CLINICAL SIGNSDocument6 pagesIRON DEFICIENCY ANEMIA ETIOLOGY AND CLINICAL SIGNSahmedNo ratings yet
- AnemiaDocument3 pagesAnemiaGhadeer AbedNo ratings yet
- Pernicious Anemia - ECEDocument46 pagesPernicious Anemia - ECEaparna reddyNo ratings yet
- Anemia y Deficit de HierroDocument3 pagesAnemia y Deficit de HierroDayira De AlarcónNo ratings yet
- 1.4 Hematologic Disorder and PregnancyDocument5 pages1.4 Hematologic Disorder and Pregnancyyen.nursing02No ratings yet
- Studi KasusDocument61 pagesStudi KasusWilson GuantengNo ratings yet
- Prefinals Overall TopicDocument8 pagesPrefinals Overall TopicClarke GriffinNo ratings yet
- Iron Deficiency Anemia Risk Factors in ChildrenDocument19 pagesIron Deficiency Anemia Risk Factors in ChildrenNadiaa RamadhaniNo ratings yet
- Anemia Health EducationDocument16 pagesAnemia Health EducationSanjeet DuhanNo ratings yet
- RicketsDocument3 pagesRicketsSaloni GanganNo ratings yet
- Anemia and Hematologic Drugs - KatzungDocument4 pagesAnemia and Hematologic Drugs - Katzungsarguss14100% (1)
- AnemiaDocument38 pagesAnemiaMustafa Salam M.NooriNo ratings yet
- Anaemia Is: Anaemia I. Background of The ConditionDocument2 pagesAnaemia Is: Anaemia I. Background of The ConditionJanella Paz ReyesNo ratings yet
- Georgemar V. Arana Jr. June 20, 2014 Group III Pedia: Anemia 1) Iron Deficiency AnemiaDocument6 pagesGeorgemar V. Arana Jr. June 20, 2014 Group III Pedia: Anemia 1) Iron Deficiency AnemiageorgeNo ratings yet
- Anemie ArticolDocument13 pagesAnemie ArticolTatiana JalbaNo ratings yet
- AnemiaDocument10 pagesAnemiaBia Payawal100% (2)
- Ms Hematologic DisorderDocument12 pagesMs Hematologic DisorderNoreen PadillaNo ratings yet
- HEMATOLOGIC DISORDERS AND PREGNANCYDocument4 pagesHEMATOLOGIC DISORDERS AND PREGNANCYRebecca ApeladoNo ratings yet
- Treating Blood Cell Deficiencies and AnemiasDocument11 pagesTreating Blood Cell Deficiencies and AnemiasVaishali PrasharNo ratings yet
- HEMATOLOGYDocument10 pagesHEMATOLOGYJo Marchianne Pigar100% (8)
- General Features of Anemia and Iron Deficiency Anemia Class Note BMLT 3rdDocument2 pagesGeneral Features of Anemia and Iron Deficiency Anemia Class Note BMLT 3rdSubhasish BarikNo ratings yet
- Amyron - Article - 27 1 14Document5 pagesAmyron - Article - 27 1 14Waqar100% (1)
- Vitamin B12 DeficiencyDocument2 pagesVitamin B12 DeficiencyFarina AcostaNo ratings yet
- Pharma E5 Ratio PDFDocument35 pagesPharma E5 Ratio PDFJoey RosalesNo ratings yet
- What Are The Causes of Nutritional Anemia, What Measures Would You Take To Prevent?Document2 pagesWhat Are The Causes of Nutritional Anemia, What Measures Would You Take To Prevent?Kelvin MaikanaNo ratings yet
- English Test 2 Write Down Illnesses Caused by Nutrional Disorders and Symptom and Threatment!Document2 pagesEnglish Test 2 Write Down Illnesses Caused by Nutrional Disorders and Symptom and Threatment!AllaftaNo ratings yet
- Agents Used Anemias: John Hommer E. Dy, MDDocument48 pagesAgents Used Anemias: John Hommer E. Dy, MDhommercuteNo ratings yet
- (Pernicious Anemia) Group 4Document2 pages(Pernicious Anemia) Group 4raven 37No ratings yet
- Micronutrients ExplainedDocument10 pagesMicronutrients ExplainedKaye Hayakawa CaibiganNo ratings yet
- Anemia, Ida 1Document131 pagesAnemia, Ida 1zaha shamseerNo ratings yet
- Vitamin B12: Harsha Vardhini.SDocument17 pagesVitamin B12: Harsha Vardhini.SScindiaaNo ratings yet
- Micronutrients in childhood nutrition: Focus on iron, zinc and vitamin ADocument9 pagesMicronutrients in childhood nutrition: Focus on iron, zinc and vitamin AVia AnggraeniNo ratings yet
- Nutritional Anemia: Dr. Mardiana, M.Kes, SP - GK Department of Clinical Nutrition Hasanuddin University MakassarDocument77 pagesNutritional Anemia: Dr. Mardiana, M.Kes, SP - GK Department of Clinical Nutrition Hasanuddin University MakassarDianaNo ratings yet
- Diphyllobothrium Latum (FishDocument3 pagesDiphyllobothrium Latum (FishSabrina TolentinoNo ratings yet
- A. According To Cause: Iron Deficiency AnemiaDocument11 pagesA. According To Cause: Iron Deficiency AnemiaEmilene VillanuevaNo ratings yet
- Hematologic Drugs (IRON)Document1 pageHematologic Drugs (IRON)Kyrriel CNo ratings yet
- Malnutrition and Its Oral Outcome - A Review: Abst TDocument3 pagesMalnutrition and Its Oral Outcome - A Review: Abst TNur YanahNo ratings yet
- Neen1 U2 A2 VesrDocument7 pagesNeen1 U2 A2 VesrMonse SanchezNo ratings yet
- HAEMATINICSDocument50 pagesHAEMATINICSvimalaNo ratings yet
- Iron and Vitamin B12 Supplement Nursing ResponsibilitiesDocument2 pagesIron and Vitamin B12 Supplement Nursing ResponsibilitiesmayanngeloNo ratings yet
- AnemiaDocument5 pagesAnemiaIssah IssahNo ratings yet
- Lesson Plan On Iron Deficiency AnemiaDocument29 pagesLesson Plan On Iron Deficiency AnemiaGLOBAL INFO-TECH KUMBAKONAMNo ratings yet
- Case Study 7Document2 pagesCase Study 7mmasi dennisNo ratings yet
- Macrocytic AnemiasDocument7 pagesMacrocytic AnemiasMohona Rahman KhanNo ratings yet
- Vitamin B12 in Vegetarian DietsDocument4 pagesVitamin B12 in Vegetarian DietsJesica DiazNo ratings yet
- Iron Deficiency AnemiaDocument17 pagesIron Deficiency Anemiaمصطفى عبد الرزاق ورد حسينNo ratings yet
- Iron Deficiency Anemia 2023Document46 pagesIron Deficiency Anemia 2023CITLALI YATZIL SANDOVAL CATALAN100% (1)
- Iron's Role in Hemoglobin and Myoglobin CyclesDocument45 pagesIron's Role in Hemoglobin and Myoglobin CyclesnajwaNo ratings yet
- Iron, Vitamin B and Folate: Key PointsDocument6 pagesIron, Vitamin B and Folate: Key PointsyennyNo ratings yet
- Vitamin B12 Deficiency, A Simple Guide To The Condition, Treatment And Related DiseasesFrom EverandVitamin B12 Deficiency, A Simple Guide To The Condition, Treatment And Related DiseasesRating: 5 out of 5 stars5/5 (2)
- Assessment of The Respiratory SystemDocument49 pagesAssessment of The Respiratory SystemMariana Mikaela AlagarNo ratings yet
- Reproductive Health Issues & DisordersDocument2 pagesReproductive Health Issues & DisordersMariana Mikaela AlagarNo ratings yet
- CHN 20191005155441 PDFDocument30 pagesCHN 20191005155441 PDFMariana Mikaela AlagarNo ratings yet
- Significant History - Events Which Influenced The Community and Contextualize Assessment and TreatmentDocument2 pagesSignificant History - Events Which Influenced The Community and Contextualize Assessment and TreatmentMariana Mikaela AlagarNo ratings yet
- TraditionalandcurrentpracticesDocument2 pagesTraditionalandcurrentpracticesMariana Mikaela AlagarNo ratings yet
- TetracyclinesDocument2 pagesTetracyclinesMariana Mikaela AlagarNo ratings yet
- NCP For Parent and Child PDFDocument3 pagesNCP For Parent and Child PDFMariana Mikaela AlagarNo ratings yet
- BoweleliminationDocument7 pagesBoweleliminationMariana Mikaela AlagarNo ratings yet
- Jesuit Astronomer Riccioli Mapped the MoonDocument2 pagesJesuit Astronomer Riccioli Mapped the MoonMariana Mikaela AlagarNo ratings yet
- SDGDocument9 pagesSDGMariana Mikaela AlagarNo ratings yet
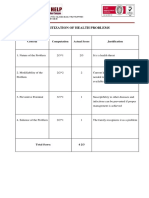
- PRIORITIZATIONDocument3 pagesPRIORITIZATIONMariana Mikaela AlagarNo ratings yet
- Male and Female He Created Them PDFDocument28 pagesMale and Female He Created Them PDFRLNo ratings yet
- BIOCHEMDocument7 pagesBIOCHEMMariana Mikaela AlagarNo ratings yet
- Maternal EffectsDocument2 pagesMaternal EffectsMariana Mikaela AlagarNo ratings yet
- Health Teaching PlanDocument2 pagesHealth Teaching PlanMariana Mikaela AlagarNo ratings yet
- Prioritizing Family Health ProblemsDocument3 pagesPrioritizing Family Health ProblemsMariana Mikaela AlagarNo ratings yet
- TetracyclinesDocument2 pagesTetracyclinesMariana Mikaela AlagarNo ratings yet
- Antibacterial Agents Pharmacotherapy With PenicillinDocument2 pagesAntibacterial Agents Pharmacotherapy With PenicillinMariana Mikaela AlagarNo ratings yet
- MicroparamikaDocument4 pagesMicroparamikaMariana Mikaela AlagarNo ratings yet
- Managing Discomforts During PregnancyDocument3 pagesManaging Discomforts During PregnancyMariana Mikaela AlagarNo ratings yet
- CN TableDocument2 pagesCN TableMariana Mikaela AlagarNo ratings yet
- Drug Route and Adult DoseDocument2 pagesDrug Route and Adult DoseMariana Mikaela AlagarNo ratings yet
- Traditional and Current Birthing Practices in the PhilippinesDocument2 pagesTraditional and Current Birthing Practices in the PhilippinesMariana Mikaela AlagarNo ratings yet
- 6 C'sDocument9 pages6 C'sMariana Mikaela AlagarNo ratings yet
- Comprehension EssayDocument2 pagesComprehension EssayMariana Mikaela AlagarNo ratings yet
- 5 Ps&leopold'sDocument4 pages5 Ps&leopold'sMariana Mikaela AlagarNo ratings yet
- Group 3 Photosynthesis CycleDocument7 pagesGroup 3 Photosynthesis CycleMariana Mikaela AlagarNo ratings yet
- Cigarette smoking is the leading preventable cause of death globallyDocument4 pagesCigarette smoking is the leading preventable cause of death globallyKyrel Ann B. MadriagaNo ratings yet
- The Little Book of The Little Book ofDocument38 pagesThe Little Book of The Little Book ofHani Gowai80% (5)
- Infant Deaths - Is There An Association With Vaccines - by Julian Gillespie, LLB, BJurisDocument11 pagesInfant Deaths - Is There An Association With Vaccines - by Julian Gillespie, LLB, BJurisSY LodhiNo ratings yet
- RD 1.1 - Pemeriksaan Radiologi Odontologi ForensikDocument52 pagesRD 1.1 - Pemeriksaan Radiologi Odontologi ForensikSanjeev AthiberanNo ratings yet
- Contemporary Approach To Dental CariesDocument465 pagesContemporary Approach To Dental CariesGeorgiana IlincaNo ratings yet
- Occupational English Test Oet Reading Test 04 Part A Text BookletDocument4 pagesOccupational English Test Oet Reading Test 04 Part A Text BookletAndreaNo ratings yet
- Over 40 Abs Solution Main GuideDocument71 pagesOver 40 Abs Solution Main Guidethe performer0% (1)
- Ghai 10ed CompetenciesDocument15 pagesGhai 10ed Competenciesghimansi50No ratings yet
- PH Form Tracks COVID-19 SymptomsDocument2 pagesPH Form Tracks COVID-19 SymptomsChristopher TorresNo ratings yet
- Developing Pharmacovigilance: New Challenges and OpportunitiesDocument32 pagesDeveloping Pharmacovigilance: New Challenges and Opportunitiesanisa rachmitaNo ratings yet
- Combination of 405 nm Laser and UV LED Reduces S. aureus BiofilmDocument17 pagesCombination of 405 nm Laser and UV LED Reduces S. aureus Biofilmbuattra nsferfile100% (1)
- EvaluationDocument2 pagesEvaluationdianwaqi00No ratings yet
- TCM Classical 5 Element Case StudyDocument4 pagesTCM Classical 5 Element Case StudyDrnarendra KumarNo ratings yet
- Bifascicular Block - LITFL - ECG Library DiagnosisDocument10 pagesBifascicular Block - LITFL - ECG Library DiagnosisKARTHICK GNo ratings yet
- Welding, Cutting & Grinding-1Document131 pagesWelding, Cutting & Grinding-1like saddamNo ratings yet
- B The Can Be Given IntramuscularDocument14 pagesB The Can Be Given IntramuscularHussein Ismail ZannounNo ratings yet
- Meeting Your Life's Money NeedsDocument55 pagesMeeting Your Life's Money NeedsAll India VideoNo ratings yet
- Micro Teaching On: Placenta PreviaDocument10 pagesMicro Teaching On: Placenta Previasuchismita pandaNo ratings yet
- Lung AbscessDocument30 pagesLung AbscessArmoured SpartanNo ratings yet
- Lec12 4th ClassDocument8 pagesLec12 4th ClassYaser JasNo ratings yet
- Things To Know About Life Sustaining Treatment4Document3 pagesThings To Know About Life Sustaining Treatment4DurgaPrasadNo ratings yet
- Nursing Care Plan for Patient with AcromegalyDocument3 pagesNursing Care Plan for Patient with AcromegalyKian HerreraNo ratings yet
- #591 Lot.85730 EinsertDocument2 pages#591 Lot.85730 Einsertjnyng222No ratings yet
- Trauma Dan Kegawatdaruratan MataDocument92 pagesTrauma Dan Kegawatdaruratan MataM Isyhaduul IslamNo ratings yet
- TransAmerica Cancer PlanDocument10 pagesTransAmerica Cancer PlanpreparebenefitsNo ratings yet
- KSADS DSM 5 Supp4 DevelopmentalDisruptiveDO FinalDocument28 pagesKSADS DSM 5 Supp4 DevelopmentalDisruptiveDO FinalKsenia Startseva-LoraNo ratings yet
- Impact of Covid-19 On Indian EconomyDocument17 pagesImpact of Covid-19 On Indian EconomyLabonita ChatterjeeNo ratings yet
- The Sleep-Deprived Human BrainDocument15 pagesThe Sleep-Deprived Human BrainHector AngelNo ratings yet
- The Science of Sleep: A Guide to Better SleepDocument2 pagesThe Science of Sleep: A Guide to Better SleepMark Anthony RaymundoNo ratings yet
- Physical Hazard: K3 - Tri Partuti - Teknik MetalurgiDocument33 pagesPhysical Hazard: K3 - Tri Partuti - Teknik MetalurgifalahNo ratings yet