You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5807)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Important Considerations For Measuring Human Body Temperature With Infrared ThermometersDocument27 pagesImportant Considerations For Measuring Human Body Temperature With Infrared ThermometersSelyun E OnnajNo ratings yet
- Safety Procedures and Guidelines Manual: March 2020Document233 pagesSafety Procedures and Guidelines Manual: March 2020Selyun E OnnajNo ratings yet
- Communication Plan Presentation: by Redroot Artists CooperativeDocument51 pagesCommunication Plan Presentation: by Redroot Artists CooperativeSelyun E OnnajNo ratings yet
- Webinar Understanding and Implementing Decision Rules in The New ISO-IEC 17025Document40 pagesWebinar Understanding and Implementing Decision Rules in The New ISO-IEC 17025Selyun E OnnajNo ratings yet
- Departmentofscience and Technology Regional Office No. IllDocument1 pageDepartmentofscience and Technology Regional Office No. IllSelyun E OnnajNo ratings yet
- Silvonen Presentation 3Document26 pagesSilvonen Presentation 3Selyun E OnnajNo ratings yet
- For Water Testing: Up To The Brim, No HeadspaceDocument4 pagesFor Water Testing: Up To The Brim, No HeadspaceSelyun E OnnajNo ratings yet
- Light Commercial Variable Air Volume (VAV) : Packaged Rooftops / 6 To 23 TonsDocument2 pagesLight Commercial Variable Air Volume (VAV) : Packaged Rooftops / 6 To 23 TonsSelyun E OnnajNo ratings yet
- Weatherexpert Ultra High Efficiency Gas Heat/Electric Cooling Packaged Variable Air Volume (Vav) RooftopDocument14 pagesWeatherexpert Ultra High Efficiency Gas Heat/Electric Cooling Packaged Variable Air Volume (Vav) RooftopSelyun E OnnajNo ratings yet
- Guide Specifications - 48Lc 14-26Document14 pagesGuide Specifications - 48Lc 14-26Selyun E OnnajNo ratings yet
- Safety Rules: Applicable Standard: N/A Employees Affected: All What Is It?Document4 pagesSafety Rules: Applicable Standard: N/A Employees Affected: All What Is It?Selyun E OnnajNo ratings yet
- AO006 2018 New Calibration FeesDocument11 pagesAO006 2018 New Calibration FeesSelyun E OnnajNo ratings yet
- Technology: Best Served ColdDocument1 pageTechnology: Best Served ColdSelyun E OnnajNo ratings yet
- Setting-Up of One-Stop Laboratory Services For Global Competitiveness (Onelab)Document2 pagesSetting-Up of One-Stop Laboratory Services For Global Competitiveness (Onelab)Selyun E OnnajNo ratings yet
- Weights and Measures - Norzagaray - 06 July 2017Document146 pagesWeights and Measures - Norzagaray - 06 July 2017Selyun E OnnajNo ratings yet
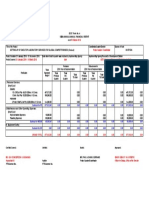
- DOST Form No. 4 Semi-Annual/Annual Financial Report As ofDocument1 pageDOST Form No. 4 Semi-Annual/Annual Financial Report As ofSelyun E OnnajNo ratings yet
- STII Terms of ReferenceDocument1 pageSTII Terms of ReferenceSelyun E OnnajNo ratings yet
- Sample Receiving PresentationDocument11 pagesSample Receiving PresentationSelyun E OnnajNo ratings yet
- Stakeholder Comments Form - Metrology BillDocument21 pagesStakeholder Comments Form - Metrology BillSelyun E OnnajNo ratings yet
- Waiver Funeral Benefit Ret01226 PDFDocument1 pageWaiver Funeral Benefit Ret01226 PDFSelyun E OnnajNo ratings yet
- Training Course On The Calibration of Weighbridges: (Draft Programme)Document2 pagesTraining Course On The Calibration of Weighbridges: (Draft Programme)Selyun E OnnajNo ratings yet
- Steps On Adding Footer and Header Inside Post PagesDocument3 pagesSteps On Adding Footer and Header Inside Post PagesSelyun E OnnajNo ratings yet
- A17.1-201X, Safety Code For Elevators and Escalators: March 2015 Draft For Public ReviewDocument53 pagesA17.1-201X, Safety Code For Elevators and Escalators: March 2015 Draft For Public ReviewSelyun E OnnajNo ratings yet