You might also like
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- An Increasing of The Efficiency of Microbiological Synthesis of 1 3 Propanediol From Crude Glycerol by The Concentration of BiomassDocument7 pagesAn Increasing of The Efficiency of Microbiological Synthesis of 1 3 Propanediol From Crude Glycerol by The Concentration of BiomassMaruf MuhammadNo ratings yet
- Evaluation of Different Expression Systems For The Heterologous Expression of Pyranose 2 Oxidase From Trametes Multicolor in e ColiDocument9 pagesEvaluation of Different Expression Systems For The Heterologous Expression of Pyranose 2 Oxidase From Trametes Multicolor in e ColiMaruf MuhammadNo ratings yet
- Bioconversion of Xylose Hexoses and Biomass To Ethanol by A New Isolate of The White Rot Basidiomycete Trametes Versicolor PDFDocument9 pagesBioconversion of Xylose Hexoses and Biomass To Ethanol by A New Isolate of The White Rot Basidiomycete Trametes Versicolor PDFMaruf MuhammadNo ratings yet
- Covalent Immobilization of Microbial Naringinase Using Novel Thermally Stable Biopolymer For Hydrolysis of Naringin PDFDocument10 pagesCovalent Immobilization of Microbial Naringinase Using Novel Thermally Stable Biopolymer For Hydrolysis of Naringin PDFMaruf MuhammadNo ratings yet
- Genome Mining For Natural Product Biosynthetic Gene Clusters in The Subsection V CyanobacteriaDocument20 pagesGenome Mining For Natural Product Biosynthetic Gene Clusters in The Subsection V CyanobacteriaMaruf MuhammadNo ratings yet
- Identification of Opportunistic Pathogenic Bacteria in Drinking Water Samples of Different Rural Health Centers and Their Clinical Impacts On HumansDocument11 pagesIdentification of Opportunistic Pathogenic Bacteria in Drinking Water Samples of Different Rural Health Centers and Their Clinical Impacts On HumansMaruf MuhammadNo ratings yet
- Class Test-12 - English (Phrase)Document6 pagesClass Test-12 - English (Phrase)Maruf MuhammadNo ratings yet
- Carbon Dioxide Fixation by Calvin Cycle Enzymes Improves Ethanol Yield in YeastDocument12 pagesCarbon Dioxide Fixation by Calvin Cycle Enzymes Improves Ethanol Yield in YeastMaruf MuhammadNo ratings yet
- A Significant Number of Reported Absidia Corymbifera Lichtheimia Corymbifera Infections Are Caused by Lichtheimia Ramosa Syn Lichtheimia Hongkongensis An Emerging Cause of MucormycosisDocument8 pagesA Significant Number of Reported Absidia Corymbifera Lichtheimia Corymbifera Infections Are Caused by Lichtheimia Ramosa Syn Lichtheimia Hongkongensis An Emerging Cause of MucormycosisMaruf MuhammadNo ratings yet
- Cow Dung A Potential Biomass Substrate For The Production of Detergent Stable Dehairing Protease by Alkaliphilic Bacillus Subtilis Strain VVDocument9 pagesCow Dung A Potential Biomass Substrate For The Production of Detergent Stable Dehairing Protease by Alkaliphilic Bacillus Subtilis Strain VVMaruf MuhammadNo ratings yet
- Correlation Between Agar Plate Screening and Solid State Fermentation For The Prediction of Cellulase Production by Trichoderma StrainsDocument8 pagesCorrelation Between Agar Plate Screening and Solid State Fermentation For The Prediction of Cellulase Production by Trichoderma StrainsMaruf MuhammadNo ratings yet
- Biofilm Development During The Start Up Period of Anaerobic Biofilm Reactors The Biofilm Archaea Community Is Highly Dependent On The Support MaterialDocument8 pagesBiofilm Development During The Start Up Period of Anaerobic Biofilm Reactors The Biofilm Archaea Community Is Highly Dependent On The Support MaterialMaruf MuhammadNo ratings yet
- An Efficient Method For The Immobilization of Inulinase Using New Types of Polymers Containing Epoxy GroupsDocument12 pagesAn Efficient Method For The Immobilization of Inulinase Using New Types of Polymers Containing Epoxy GroupsMaruf MuhammadNo ratings yet
- Kinetic Characterization and Effect of Immobilized Thermostable Glucosidase in Alginate Gel Beads On Sugarcane JuiceDocument9 pagesKinetic Characterization and Effect of Immobilized Thermostable Glucosidase in Alginate Gel Beads On Sugarcane JuiceMaruf MuhammadNo ratings yet
- The Exometabolome of Clostridium Thermocellum Reveals Overflow Metabolism at High Cellulose LoadingDocument11 pagesThe Exometabolome of Clostridium Thermocellum Reveals Overflow Metabolism at High Cellulose LoadingMaruf MuhammadNo ratings yet
- Recycling of Sewage Sludge As Production Medium For Cellulase by A Bacillus Megaterium StrainDocument15 pagesRecycling of Sewage Sludge As Production Medium For Cellulase by A Bacillus Megaterium StrainMaruf MuhammadNo ratings yet
- High-Throughput Strategies For Penicillin G Acylase Production in Re. Coli Fed-Batch CultivationsDocument13 pagesHigh-Throughput Strategies For Penicillin G Acylase Production in Re. Coli Fed-Batch CultivationsMaruf MuhammadNo ratings yet
- Degradation of o Xylene and M Xylene by A Novel Sulfate Reducer Belonging To The Genus DesulfotomaculumDocument11 pagesDegradation of o Xylene and M Xylene by A Novel Sulfate Reducer Belonging To The Genus DesulfotomaculumMaruf MuhammadNo ratings yet
- Microbial Transformation of Ginsenoside rb1 Re and rg1 and Its Contribution To The Improved Anti Inflammatory Activity of GinsengDocument10 pagesMicrobial Transformation of Ginsenoside rb1 Re and rg1 and Its Contribution To The Improved Anti Inflammatory Activity of GinsengjdfhakfdNo ratings yet
- Brief Report: Corynebacterium GlutamicumDocument5 pagesBrief Report: Corynebacterium GlutamicumMaruf MuhammadNo ratings yet
- Physiological Characterization of Thermotolerant Yeast For Cellulosic Ethanol ProductionDocument12 pagesPhysiological Characterization of Thermotolerant Yeast For Cellulosic Ethanol ProductionMaruf MuhammadNo ratings yet
- The Impact of Diclofenac and Ibuprofen On Biofilm Formation On The Surface of Polypropylene MeshDocument7 pagesThe Impact of Diclofenac and Ibuprofen On Biofilm Formation On The Surface of Polypropylene MeshMaruf MuhammadNo ratings yet
- Vasoconstriction Potency Induced by Aminoamide Local Anesthetics Correlates With Lipid Solubility PDFDocument8 pagesVasoconstriction Potency Induced by Aminoamide Local Anesthetics Correlates With Lipid Solubility PDFMaruf MuhammadNo ratings yet
- Imac Capture of Recombinant Protein From Unclarified Mammalian Cell Feed StreamsDocument11 pagesImac Capture of Recombinant Protein From Unclarified Mammalian Cell Feed StreamsMaruf MuhammadNo ratings yet
- Metabolic Engineering For The Microbial Production of Isoprenoids Carotenoids and Isoprenoid Based BiofuelsDocument9 pagesMetabolic Engineering For The Microbial Production of Isoprenoids Carotenoids and Isoprenoid Based BiofuelsjdfhakfdNo ratings yet
- Use of Cationic Polymers To Reduce Pathogen Levels During Dairy Manure SeparationDocument7 pagesUse of Cationic Polymers To Reduce Pathogen Levels During Dairy Manure SeparationjdfhakfdNo ratings yet
- Towards Synthesis of Monoterpenes and Derivatives Using Synthetic BiologyDocument7 pagesTowards Synthesis of Monoterpenes and Derivatives Using Synthetic BiologyjdfhakfdNo ratings yet
- a-design-build-test-cycle-using-modeling-and-experiments-reveals-interdependencies-between-upper-glycolysis-and-xylose-uptake-in-recombinant-s-cerevisiae-and-improves-predictive-capabilities-of-large-scale-kineDocument19 pagesa-design-build-test-cycle-using-modeling-and-experiments-reveals-interdependencies-between-upper-glycolysis-and-xylose-uptake-in-recombinant-s-cerevisiae-and-improves-predictive-capabilities-of-large-scale-kineMaruf MuhammadNo ratings yet
- Amino Acid Catabolism Directed Biofuel Production in Clostridium Sticklandii An Insight Into Model Driven Systems EngineeringDocument29 pagesAmino Acid Catabolism Directed Biofuel Production in Clostridium Sticklandii An Insight Into Model Driven Systems EngineeringMaruf MuhammadNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Vasoconstriction in Septic Shock: What'S New in Intensive CareDocument4 pagesVasoconstriction in Septic Shock: What'S New in Intensive CareGabriela PachecoNo ratings yet
- Plasticity FascialDocument13 pagesPlasticity FascialMichael DuranNo ratings yet
- One Lung VentilationDocument38 pagesOne Lung VentilationVarun Reddy V100% (1)
- Heat and Cold ApplicationDocument5 pagesHeat and Cold ApplicationBern NerquitNo ratings yet
- The Pharmacology of Adrenergic Receptors PDFDocument15 pagesThe Pharmacology of Adrenergic Receptors PDFKathryn MitchellNo ratings yet
- AUTACOIDSDocument45 pagesAUTACOIDSArshiya FatimaNo ratings yet
- PharmacologyDocument236 pagesPharmacologynbde2100% (5)
- Thermoregulation and The Heart ReviewDocument3 pagesThermoregulation and The Heart ReviewDavidNo ratings yet
- Untitled19 PDFDocument19 pagesUntitled19 PDFElizabeth LeonNo ratings yet
- Chapter 12 Biology 11Document52 pagesChapter 12 Biology 11ax1leNo ratings yet
- Raynaud's Phenomenon: Review ArticleDocument10 pagesRaynaud's Phenomenon: Review ArticleDhakves JustikaNo ratings yet
- Epinephrine Vs Norepinephrine: Advanced Pharmacology Dr. Sana' Al Aqqad by Students: Ali Ghanem Ismael Bani MatarDocument15 pagesEpinephrine Vs Norepinephrine: Advanced Pharmacology Dr. Sana' Al Aqqad by Students: Ali Ghanem Ismael Bani MatarSabrina ShalhoutNo ratings yet
- Тема 4Document19 pagesТема 4张晨No ratings yet
- B1 SyncopeDocument84 pagesB1 SyncopeAnonymous HH3c17osNo ratings yet
- Krok 1 - 2015 (Physiology)Document28 pagesKrok 1 - 2015 (Physiology)Harsh NimavatNo ratings yet
- Hypercapnia: Neus Fabregas, Juan Fernández-CandilDocument12 pagesHypercapnia: Neus Fabregas, Juan Fernández-CandilGone WaysNo ratings yet
- Infiltration & EkstravasationDocument9 pagesInfiltration & EkstravasationSasha Hidayat FullNo ratings yet
- Free Chapter - Recovery - From - Training PDFDocument24 pagesFree Chapter - Recovery - From - Training PDFSzigmund100% (1)
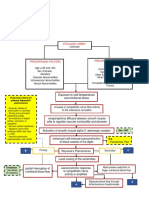
- Pathophysiology Raynauds Phenomenon Schematic DiagramDocument6 pagesPathophysiology Raynauds Phenomenon Schematic DiagramEerie Era0% (1)
- Lect 75control of Tissue Blood FlowDocument23 pagesLect 75control of Tissue Blood FlowEl FaroukNo ratings yet
- Whole-Body Human Thermal Models: E. H. WisslerDocument50 pagesWhole-Body Human Thermal Models: E. H. WisslerArinjayKumarNo ratings yet
- @anesthesia - Books 2015 MCQs For Handbook of Local Anesthesia PDFDocument205 pages@anesthesia - Books 2015 MCQs For Handbook of Local Anesthesia PDFVivek Sinha100% (2)
- Guyton Hall PHYSIOLOGY Chapter 18 PDFDocument2 pagesGuyton Hall PHYSIOLOGY Chapter 18 PDFOsman NazirNo ratings yet
- PR1301 Tutorial 1Document2 pagesPR1301 Tutorial 1BeatriceKayNo ratings yet
- BP602T Unit 1-3Document207 pagesBP602T Unit 1-3Gyampoh SolomonNo ratings yet
- 10.4 Homeostasis-1Document10 pages10.4 Homeostasis-1صالح ابراهيمNo ratings yet
- Prevention of Cold Injuries During ExerciseDocument18 pagesPrevention of Cold Injuries During ExerciseAdmirNo ratings yet
- Public Assessment Report Decentralised ProcedureDocument26 pagesPublic Assessment Report Decentralised Procedurefad12345No ratings yet
- MethergineDocument2 pagesMethergineKyla VillafrancaNo ratings yet
- Arterial HyperemyDocument10 pagesArterial HyperemyRohit NaiduNo ratings yet