You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Computer ProgrammingDocument32 pagesComputer ProgrammingSazibur HossainNo ratings yet
- Scehdule of Charges - Card - 2019Document2 pagesScehdule of Charges - Card - 2019Salam DhaliNo ratings yet
- Application Form For Chinese Government Scholarship: Personal DataDocument4 pagesApplication Form For Chinese Government Scholarship: Personal DataSalam DhaliNo ratings yet
- University of Alberta HandbookDocument35 pagesUniversity of Alberta HandbookHumayun GaziNo ratings yet
- Pdfanddoc 734447 PDFDocument70 pagesPdfanddoc 734447 PDFShibin TaNo ratings yet
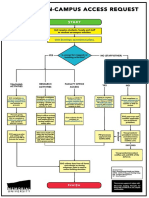
- Campus Access FlowchartDocument1 pageCampus Access FlowchartSalam DhaliNo ratings yet
- Musician A 2020 BatchDocument1 pageMusician A 2020 BatchSalam DhaliNo ratings yet
- Chemical Engineering: Masc / Meng / PHDDocument3 pagesChemical Engineering: Masc / Meng / PHDSalam DhaliNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Software Requirement SpecificationDocument10 pagesSoftware Requirement SpecificationSushil SarrafNo ratings yet
- Instruction Manual Series 880 CIU Plus: July 2009 Part No.: 4416.526 Rev. 6Document44 pagesInstruction Manual Series 880 CIU Plus: July 2009 Part No.: 4416.526 Rev. 6nknico100% (1)
- Steps To Control Water Depletion Jun2019Document2 pagesSteps To Control Water Depletion Jun2019chamanNo ratings yet
- SignalsVOL 1 SupplementBDocument67 pagesSignalsVOL 1 SupplementBcdettlingerNo ratings yet
- VTP Renault 6.14.1 Web Version - Pdf.pagespeed - Ce.c T5zGltXA PDFDocument176 pagesVTP Renault 6.14.1 Web Version - Pdf.pagespeed - Ce.c T5zGltXA PDFIbrahim AwadNo ratings yet
- Nyush Ds Cs Capstone Outline TemplateDocument2 pagesNyush Ds Cs Capstone Outline TemplateFresh Prince Of NigeriaNo ratings yet
- Group Terms&ConditionsDocument5 pagesGroup Terms&Conditionsbelen rodriguezNo ratings yet
- Marketing For Hospitality & TourismDocument5 pagesMarketing For Hospitality & Tourismislahu56No ratings yet
- Virtual Vacancy Round 2 Mbbs - Bds Ug Counselling 20Document90 pagesVirtual Vacancy Round 2 Mbbs - Bds Ug Counselling 20Jaydev DegloorkarNo ratings yet
- Sfa 5.22 PDFDocument36 pagesSfa 5.22 PDFLuis Evangelista Moura PachecoNo ratings yet
- International Maritime Solid Bulk Cargoes (IMSBC) CodeDocument18 pagesInternational Maritime Solid Bulk Cargoes (IMSBC) CodeJasper Abrantes100% (1)
- Marine Products: SL-3 Engine ControlsDocument16 pagesMarine Products: SL-3 Engine ControlsPedro GuerraNo ratings yet
- 20 X 70Document102 pages20 X 70MatAlengNo ratings yet
- Mechanical FPD P.sanchezDocument9 pagesMechanical FPD P.sanchezHailley DensonNo ratings yet
- Lucrare de DiplomaDocument99 pagesLucrare de DiplomarashcapurNo ratings yet
- HTTP ProtocolDocument16 pagesHTTP ProtocolHao NguyenNo ratings yet
- imageRUNNER+ADVANCE+C5051-5045-5035-5030 Parts CatalogDocument268 pagesimageRUNNER+ADVANCE+C5051-5045-5035-5030 Parts CatalogDragos Burlacu100% (1)
- PosdmDocument29 pagesPosdmChandraBhushan67% (3)
- Application For New Ration Card - Telangana & AP StatesDocument1 pageApplication For New Ration Card - Telangana & AP Statesping2gopiNo ratings yet
- Diagrame Des MomentsDocument1 pageDiagrame Des Momentsabdoul ndiayeNo ratings yet
- Part - A (Short Answer Questions) : S. No. Questions Bloom's Taxonomy Level Course OutcomeDocument11 pagesPart - A (Short Answer Questions) : S. No. Questions Bloom's Taxonomy Level Course OutcomeDevendra BhavsarNo ratings yet
- 13 DocumentsDocument38 pages13 DocumentsPoorClaresBostonNo ratings yet
- (E-Brochure) Ginza HillDocument6 pages(E-Brochure) Ginza HillRenald 'Renald' RenaldNo ratings yet
- MN502 Lecture 3 Basic CryptographyDocument45 pagesMN502 Lecture 3 Basic CryptographySajan JoshiNo ratings yet
- A033Document24 pagesA033PRANAV GOYALNo ratings yet
- NV 2Document2 pagesNV 2Joshua ApongolNo ratings yet
- Bidding Process in Infrastructure ProjectsDocument44 pagesBidding Process in Infrastructure ProjectsRajesh Chowdary Chintamaneni100% (2)
- 2 - McCullough HospitalDocument2 pages2 - McCullough HospitalGuru Charan ChitikenaNo ratings yet
- Drafting Foundation PlanDocument24 pagesDrafting Foundation Planerol bancoroNo ratings yet
- Challenges Students Face in Conducting A Literature ReviewDocument6 pagesChallenges Students Face in Conducting A Literature ReviewafdtunqhoNo ratings yet