You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5819)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Job DescriptionDocument10 pagesJob Descriptionpioneer92No ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Discharge Audit For AMAU: Instructions For Audit ToolDocument37 pagesDischarge Audit For AMAU: Instructions For Audit Toolpioneer92No ratings yet
- Safe Site Surgery Audit ToolDocument9 pagesSafe Site Surgery Audit Toolpioneer92No ratings yet
- Pain Management Audit Pain Management AuditDocument12 pagesPain Management Audit Pain Management Auditpioneer92No ratings yet
- WAST 2020 Person Specification (For August 2020 Intake Onwards)Document3 pagesWAST 2020 Person Specification (For August 2020 Intake Onwards)pioneer92No ratings yet
- CCrISP-13-Nutrition and The Surgical PatientDocument27 pagesCCrISP-13-Nutrition and The Surgical Patientpioneer92No ratings yet
- CCrISP-11-Fluid and Electrolyte Management PDFDocument19 pagesCCrISP-11-Fluid and Electrolyte Management PDFpioneer92100% (1)
- CCrISP 1 IntroductionDocument19 pagesCCrISP 1 Introductionpioneer92No ratings yet
- Introduction To Neuro Marketing: Slide Prepared By-Anshu and HarshyashweeDocument10 pagesIntroduction To Neuro Marketing: Slide Prepared By-Anshu and HarshyashweeAmisha SinghNo ratings yet
- Chapter 2 Plant Asset and Intangible AssetDocument18 pagesChapter 2 Plant Asset and Intangible AssetasnfkasNo ratings yet
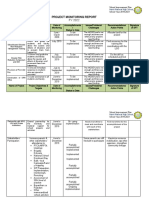
- Project Monitoring Report. GovernanceDocument6 pagesProject Monitoring Report. GovernanceJASMIN FAMANo ratings yet
- Unauthorised: Certificate of Inspection For Import of Products From Organic Production Into The European UnionDocument2 pagesUnauthorised: Certificate of Inspection For Import of Products From Organic Production Into The European UnionIndriani widya utariNo ratings yet
- PR1 - Module 1Document48 pagesPR1 - Module 1Angelie Rose CañezoNo ratings yet
- CSR by Mahindra GroupDocument27 pagesCSR by Mahindra GroupPriyankar PaulNo ratings yet
- Abstract Book - ICFME-2022Document105 pagesAbstract Book - ICFME-2022S R E E N I V A S ANo ratings yet
- FM 8500Document99 pagesFM 8500SergeyNo ratings yet
- CPI Hands - On - 20Document20 pagesCPI Hands - On - 20Yannick AssoumanNo ratings yet
- Information On The MIP Program Session 2018-2020: (Last Update: August 2017)Document3 pagesInformation On The MIP Program Session 2018-2020: (Last Update: August 2017)Imran JuttNo ratings yet
- InstallationManualDocument6 pagesInstallationManualErnest IpNo ratings yet
- Blank BOL - 1Document1 pageBlank BOL - 1Ion CojocaruNo ratings yet
- WEEDS and PestsDocument35 pagesWEEDS and PestsolawedabbeyNo ratings yet
- GU-612 - v3.1 - Guidelines - Incident Investigation and Reporting v1Document185 pagesGU-612 - v3.1 - Guidelines - Incident Investigation and Reporting v1rwerwerw100% (3)
- HP Openview Operations 7.5 For Windows Software: Data SheetDocument8 pagesHP Openview Operations 7.5 For Windows Software: Data Sheetlakbabi1035No ratings yet
- 3.1 Käfigläufer-Motoren 3.1 Käfigläufer-Motoren: 3.1 Squirrel Cage Motors 3.1 Squirrel Cage MotorsDocument1 page3.1 Käfigläufer-Motoren 3.1 Käfigläufer-Motoren: 3.1 Squirrel Cage Motors 3.1 Squirrel Cage MotorsAndro MedaNo ratings yet
- Different Forms of BUSINESS ORGANIZATIONS JSDocument7 pagesDifferent Forms of BUSINESS ORGANIZATIONS JSKristina PabloNo ratings yet
- Veenus Medi Lab Panadura - BC 10Document7 pagesVeenus Medi Lab Panadura - BC 10Nirmani HansiniNo ratings yet
- Tentative Counselling Schedule, Admissions 2022-23 UG Programs (Except B. Tech & B. Lib.)Document1 pageTentative Counselling Schedule, Admissions 2022-23 UG Programs (Except B. Tech & B. Lib.)Devika KapoorNo ratings yet
- Documents - Pub Frankfinn Travel Assignment 55b0f8cdb266bDocument78 pagesDocuments - Pub Frankfinn Travel Assignment 55b0f8cdb266bSidhu RajputNo ratings yet
- Centre For Research: Dr.V.Murugesan DirectorDocument2 pagesCentre For Research: Dr.V.Murugesan Directornellai kumarNo ratings yet
- Professional Engrg in Nigeria-1Document4 pagesProfessional Engrg in Nigeria-1mykekeysNo ratings yet
- ATG - Automatic Tank Gauge System: Installation Requirements of MTG vs. Hybrid RadarDocument1 pageATG - Automatic Tank Gauge System: Installation Requirements of MTG vs. Hybrid RadarRicardo souzaNo ratings yet
- Analytical Study of Cloud ERP and ERPDocument9 pagesAnalytical Study of Cloud ERP and ERPLilamala LilavelikaNo ratings yet
- SCP Technical GuideDocument108 pagesSCP Technical GuideJosé Luis Morán HernándezNo ratings yet
- Resume: Mahesh - Nagappa.GalagaliDocument2 pagesResume: Mahesh - Nagappa.GalagaliMahesh ChiniwalarNo ratings yet
- Report of The Department of The Army Review of The Preliminary Investigations Into The My Lai Incident-V3-Exhibits-Book2Document432 pagesReport of The Department of The Army Review of The Preliminary Investigations Into The My Lai Incident-V3-Exhibits-Book2zepolkNo ratings yet
- Civil Vi Environmental Engineering I (10cv61) NotesDocument142 pagesCivil Vi Environmental Engineering I (10cv61) NotesPoojit Popli100% (1)
- Manitowoc 3900W CatalogueDocument10 pagesManitowoc 3900W Cataloguesolly79No ratings yet
- Test Bank For Community Health Nursing A Canadian Perspective 5th Edition Lynnette Leeseberg Stamler Lynnette Leeseberg Stamler Lucia Yiu Aliyah Dosani Josephine Etowa Cheryl Van Daalen SmithDocument86 pagesTest Bank For Community Health Nursing A Canadian Perspective 5th Edition Lynnette Leeseberg Stamler Lynnette Leeseberg Stamler Lucia Yiu Aliyah Dosani Josephine Etowa Cheryl Van Daalen SmithLinda Burnham100% (33)