You might also like
- Anatomy: 1800 Multiple Choice QuestionsFrom EverandAnatomy: 1800 Multiple Choice QuestionsRating: 3.5 out of 5 stars3.5/5 (15)
- Randall Cooper Acl Rehabilitation GuideDocument28 pagesRandall Cooper Acl Rehabilitation GuideLacra Apetrei100% (1)
- Crowe ClassificationDocument18 pagesCrowe ClassificationPetru CarajaNo ratings yet
- Manual Muscle Testing Scoring SheetDocument1 pageManual Muscle Testing Scoring SheetjotiroyNo ratings yet
- GOOD ONE - Posterior Tibialis ExercisesDocument2 pagesGOOD ONE - Posterior Tibialis ExercisesSylvia GraceNo ratings yet
- Proximal Femoral Focal DeficiencyDocument35 pagesProximal Femoral Focal DeficiencyAlfred JacksonNo ratings yet
- Proximal Femoral Focal Deficiency (PFFD)Document23 pagesProximal Femoral Focal Deficiency (PFFD)Alfred JacksonNo ratings yet
- Perthes Disease: by Dr. Abdul Karim Postgraduate Resident Orthopedic Surgery Pgmi/Lgh. Lahore PakistanDocument68 pagesPerthes Disease: by Dr. Abdul Karim Postgraduate Resident Orthopedic Surgery Pgmi/Lgh. Lahore Pakistandrakkashmiri50% (2)
- Presentation LLD FarzandDocument44 pagesPresentation LLD Farzanddrakkashmiri100% (1)
- Legg Calve PerthesDocument93 pagesLegg Calve PerthesAkshay LakraNo ratings yet
- Congenital Femoral Phocomelia: Al-Amin Mohamed Osman Abdiaziz Ibrahim MohamedDocument24 pagesCongenital Femoral Phocomelia: Al-Amin Mohamed Osman Abdiaziz Ibrahim MohamedAlfred JacksonNo ratings yet
- Perthes DiseaseDocument45 pagesPerthes DiseaseAh ZhangNo ratings yet
- Fractures of Proximal FemurDocument38 pagesFractures of Proximal FemurMisoNo ratings yet
- Trauma Medulla SpinalisDocument79 pagesTrauma Medulla SpinalisiqiqiqiqiqNo ratings yet
- Developmental Dysplasia of The HipDocument33 pagesDevelopmental Dysplasia of The HipJoy KirumbaNo ratings yet
- 2009.10.09 Legg Calve Perthes Disease 2Document43 pages2009.10.09 Legg Calve Perthes Disease 2AnItaNo ratings yet
- DR - O. K. A. SamuelsDocument76 pagesDR - O. K. A. Samuelsgdudex118811No ratings yet
- Overview Congenital Musculoskeletal DisorderDocument84 pagesOverview Congenital Musculoskeletal DisorderRyan Trian100% (3)
- Legg CALVE PERVE DISEASEDocument7 pagesLegg CALVE PERVE DISEASEYussika FernandaNo ratings yet
- Congenital Abnormalities MusculoSkeletal SystemDocument116 pagesCongenital Abnormalities MusculoSkeletal SystemVii syilsaNo ratings yet
- PR LEviDocument14 pagesPR LEviEMIRZA NUR WICAKSONONo ratings yet
- Pediatric Orthopaedics: Dr. Andreas Siagian SpotDocument66 pagesPediatric Orthopaedics: Dr. Andreas Siagian SpotFirdausi RiskiviawinandaNo ratings yet
- Surgical Treatment of DDH in Adults, ThaDocument11 pagesSurgical Treatment of DDH in Adults, ThaMyhay CretzuNo ratings yet
- Hip Dislocations and Femoral Head Fractures: John T. Gorczyca, MDDocument97 pagesHip Dislocations and Femoral Head Fractures: John T. Gorczyca, MDLassie LazyNo ratings yet
- Legg Calves Pertes Mas CortoDocument4 pagesLegg Calves Pertes Mas CortoGabriel MolinaNo ratings yet
- Hip Fractures: by Tariq KhanDocument42 pagesHip Fractures: by Tariq KhanKamran Khan KhalilNo ratings yet
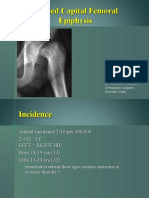
- Slipped Capital Femoral Epiphysis: Vivek PandeyDocument30 pagesSlipped Capital Femoral Epiphysis: Vivek PandeyvivpanNo ratings yet
- Hip DislocDocument67 pagesHip DislocAli TawbeNo ratings yet
- Hip DislocationDocument39 pagesHip DislocationSHAMENI VINODNo ratings yet
- Hip ProblemsDocument46 pagesHip ProblemsDhiya' VinaNo ratings yet
- 4 Perthes Ve SCFEDocument34 pages4 Perthes Ve SCFECharl UnalNo ratings yet
- Pediatric Lower Extremity Orthopedic ConcernsDocument28 pagesPediatric Lower Extremity Orthopedic ConcernsDitaAnggaraKusumaNo ratings yet
- Pediatric OrthopaedicDocument66 pagesPediatric OrthopaedicDhito RodriguezNo ratings yet
- Exploring Advances in THADocument73 pagesExploring Advances in THABridgit FinleyNo ratings yet
- Isthmic Spondylolisthesis: Anterior Vs Posterior FusionDocument48 pagesIsthmic Spondylolisthesis: Anterior Vs Posterior FusionneareastspineNo ratings yet
- Congenital Posteromedial BowingDocument28 pagesCongenital Posteromedial BowingLokesh SharmaNo ratings yet
- Slipped Capital Femoral EpiphysisDocument40 pagesSlipped Capital Femoral EpiphysisDrAshesh Desai100% (2)
- Ortho McqsDocument27 pagesOrtho McqsRandom HNo ratings yet
- Scfe2 140618022225 Phpapp01Document48 pagesScfe2 140618022225 Phpapp01Alexandro WiyandaNo ratings yet
- Fracture-Dislocation of The Hip-KaizarDocument69 pagesFracture-Dislocation of The Hip-KaizarKaizar Ennis100% (1)
- Congenital Dislocation of The Knee - RP's Ortho NotesDocument3 pagesCongenital Dislocation of The Knee - RP's Ortho NotesSabari NathNo ratings yet
- Adolescent Idiopathic ScoliosisDocument42 pagesAdolescent Idiopathic ScoliosisPerjalanan SukarNo ratings yet
- Dr. Robert Tirtowijoyo (Paediatric Condition) Inggris UMJ Maret 2008Document73 pagesDr. Robert Tirtowijoyo (Paediatric Condition) Inggris UMJ Maret 2008Muhamad Agung SupriyantoNo ratings yet
- Dr. Robert Tirtowijoyo (Paediatric Condition) Inggris UMJ Maret 2008 EditedDocument73 pagesDr. Robert Tirtowijoyo (Paediatric Condition) Inggris UMJ Maret 2008 EditedMuhamad Agung SupriyantoNo ratings yet
- Referat Reconstruction IDocument7 pagesReferat Reconstruction IReza Devianto HambaliNo ratings yet
- S1.2 Spinal Trauma, Orthopaedic Management - DR Ahmad RamdanDocument47 pagesS1.2 Spinal Trauma, Orthopaedic Management - DR Ahmad RamdanParadita MulyaNo ratings yet
- Lower Extremity DisordersDocument25 pagesLower Extremity DisordersJameson87No ratings yet
- CtevDocument30 pagesCtevHernanda Haudzan HakimNo ratings yet
- Pathological FractureDocument92 pagesPathological FractureSeptyAuliaNo ratings yet
- Shih 2018Document7 pagesShih 2018Genesis Cedeño GonzalezNo ratings yet
- Slipped Capital Femoral Epiphysis: MSC Otho, MRCS Assistant Lecturer of Orthopaedic at Ain Shams UniversityDocument30 pagesSlipped Capital Femoral Epiphysis: MSC Otho, MRCS Assistant Lecturer of Orthopaedic at Ain Shams UniversityBell Swan100% (1)
- Femoral Neck FracturesDocument8 pagesFemoral Neck FracturesMorshed Mahbub AbirNo ratings yet
- PESCAVUSDocument67 pagesPESCAVUSozan_amir14614No ratings yet
- Develop Med Child Neuro - 2009 - ROOT - Surgical Treatment For Hip Pain in The Adult Cerebral Palsy PatientDocument8 pagesDevelop Med Child Neuro - 2009 - ROOT - Surgical Treatment For Hip Pain in The Adult Cerebral Palsy PatientSitthikorn StrikerrNo ratings yet
- 2023 Cavus Foot SurgeryDocument83 pages2023 Cavus Foot SurgerysaragNo ratings yet
- Developmental Dysplasia of The Hip: Dr. Bassel El-Osta SPR Trauma & OrthopaedicsDocument71 pagesDevelopmental Dysplasia of The Hip: Dr. Bassel El-Osta SPR Trauma & OrthopaedicsvadimmadanNo ratings yet
- 8.8.2017 - Fracture of FemurDocument57 pages8.8.2017 - Fracture of FemurUlfa Sari Al-BahmiNo ratings yet
- Hip Fracture of Proximal Femur SOAP COMPLETEDocument10 pagesHip Fracture of Proximal Femur SOAP COMPLETEEj TuliaoNo ratings yet
- Evan, MD Orthopaedic and Traumatology University of Kristen Krida WacanaDocument39 pagesEvan, MD Orthopaedic and Traumatology University of Kristen Krida WacanaIyannyanNo ratings yet
- 3.pediatric Hip DisordersDocument92 pages3.pediatric Hip DisordersMahmoud Abu Al AmrainNo ratings yet
- Andi Rahmat Hidayat C 111 07 104 Advisor: Dr. Andi Sirfa Dr. Helmiyadi Kuswardhana Supervisor: Dr. Henry Yurianto, M.Phill, PHD, SP - OtDocument30 pagesAndi Rahmat Hidayat C 111 07 104 Advisor: Dr. Andi Sirfa Dr. Helmiyadi Kuswardhana Supervisor: Dr. Henry Yurianto, M.Phill, PHD, SP - OtAndi Rahmat HidayatNo ratings yet
- Hip Neck Fracture, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHip Neck Fracture, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- A Simple Guide to the Neck and Its Disorders, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to the Neck and Its Disorders, Diagnosis, Treatment and Related ConditionsNo ratings yet
- Sample of English EssayDocument5 pagesSample of English Essayb6yf8tcd100% (2)
- Handout Appendicular Skeletal SystemDocument13 pagesHandout Appendicular Skeletal SystemRhodjane Dela CruzNo ratings yet
- Glutes Manual enDocument18 pagesGlutes Manual enPrincess BrownNo ratings yet
- ACL Reconstruction PhysiotherapyDocument20 pagesACL Reconstruction Physiotherapyking4lifeNo ratings yet
- Ankle LectureDocument19 pagesAnkle Lecturegunawan crisNo ratings yet
- PFC RP Surgical Technique (DePuy)Document43 pagesPFC RP Surgical Technique (DePuy)Sagaram Shashidar100% (1)
- Ankle Foot OrthosisDocument4 pagesAnkle Foot Orthosis楊畯凱No ratings yet
- Case Study For CastDocument10 pagesCase Study For CastMaria JuvilisaNo ratings yet
- Patient LoadDocument6 pagesPatient LoadJoanna EdenNo ratings yet
- Frog Muscles With OIA PDFDocument4 pagesFrog Muscles With OIA PDFAaron ArasaNo ratings yet
- 97-5994-302-00 Rev3 NexGen LCCK 4-In-1 Instrument STDocument52 pages97-5994-302-00 Rev3 NexGen LCCK 4-In-1 Instrument STJehannah Dayanara HayudiniNo ratings yet
- The Effect of The Gastrocnemius On The Plantar Fascia: Javier Pascual HuertaDocument18 pagesThe Effect of The Gastrocnemius On The Plantar Fascia: Javier Pascual HuertamarcelonorisNo ratings yet
- 筆記Document6 pages筆記姚立喬No ratings yet
- Affections of The Ankle and FootDocument77 pagesAffections of The Ankle and FootJudy Ann Bahom SantiagoNo ratings yet
- 1st Case Musculoskeletal - AuliaDocument25 pages1st Case Musculoskeletal - AuliaAULIA ANGRAININo ratings yet
- Muscles of The Thigh and LegDocument20 pagesMuscles of The Thigh and LegRawda IbrahimNo ratings yet
- Frcem Lower LimbsDocument69 pagesFrcem Lower LimbsskNo ratings yet
- 2 Hip Examination - How To Examine Hip DR Prof Anil AroraDocument112 pages2 Hip Examination - How To Examine Hip DR Prof Anil AroraSaikatNo ratings yet
- The Patellofemoral Joint PDFDocument281 pagesThe Patellofemoral Joint PDFjesussalvadorsuaza100% (2)
- Shin SplintsDocument11 pagesShin SplintsEllaNo ratings yet
- Isolated Medial Collateral Ligament Injuries in The KneeDocument6 pagesIsolated Medial Collateral Ligament Injuries in The KneekenthepaNo ratings yet
- Valgus Knee and Levels of ConstraintDocument22 pagesValgus Knee and Levels of ConstraintShu Yang HuNo ratings yet
- Achilles Tendinopathy What Runners Should Know FinitoDocument4 pagesAchilles Tendinopathy What Runners Should Know FinitoAdmirNo ratings yet
- A Systematic Review of Running-Related Musculoskeletal Injuries in RunnersDocument10 pagesA Systematic Review of Running-Related Musculoskeletal Injuries in RunnersInfo-qe QualityenergyNo ratings yet
- Paper - Fraktur TalusDocument30 pagesPaper - Fraktur TalusAriadi SyahputraNo ratings yet
- Janu Basti Treatment in AyurvedaDocument17 pagesJanu Basti Treatment in AyurvedaAP AyurvedaNo ratings yet
- ArtosDocument22 pagesArtosRia Rahmadiyani IINo ratings yet