You might also like
- Peripheral Vascular DiseaseDocument47 pagesPeripheral Vascular Diseaseusmle prepNo ratings yet
- GYNE - Chronic Pelvic Pain, Endometriosis, and AdenomyosisDocument13 pagesGYNE - Chronic Pelvic Pain, Endometriosis, and AdenomyosisAlodia RazonNo ratings yet
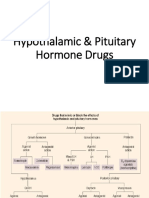
- Hypothalamic & Pituitary Hormone DrugsDocument29 pagesHypothalamic & Pituitary Hormone DrugsDylan MansillaNo ratings yet
- Appendicitis Management and Nursing Care PlanDocument37 pagesAppendicitis Management and Nursing Care PlanAlva AlfaNo ratings yet
- Deep Vein ThrombosisDocument13 pagesDeep Vein Thrombosisusmle prepNo ratings yet
- Gonadal Hormones and InhibitorsDocument14 pagesGonadal Hormones and InhibitorsbluesumNo ratings yet
- Hysterectomy, (Removal of Uterus) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHysterectomy, (Removal of Uterus) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsRating: 5 out of 5 stars5/5 (1)
- Pharm C Exam 10 Drug ListDocument2 pagesPharm C Exam 10 Drug ListVokdadaNo ratings yet
- Oral Contraceptives: Presented byDocument24 pagesOral Contraceptives: Presented byfarmasi_hm100% (1)
- Pelvic Assessment Maternity NursingDocument33 pagesPelvic Assessment Maternity Nursingusmle prepNo ratings yet
- Uterine Fibroids: An Update On Current and Emerging Medical Treatment OptionsDocument22 pagesUterine Fibroids: An Update On Current and Emerging Medical Treatment OptionsAlfian Rahman HadiNo ratings yet
- 46s - Contraception TBL (Pearson - Dillon)Document13 pages46s - Contraception TBL (Pearson - Dillon)adriaran101No ratings yet
- Endometriosis: Menstruation Seems To Play A Major Role in The Pathogenesis of EndometriosisDocument6 pagesEndometriosis: Menstruation Seems To Play A Major Role in The Pathogenesis of EndometriosisJason FooNo ratings yet
- Clinical Efficacy of Ginger Plus B 6 Vitamin in Hyperemesis Gravidarum: Report of Two Cases Case Report Case Report 1Document3 pagesClinical Efficacy of Ginger Plus B 6 Vitamin in Hyperemesis Gravidarum: Report of Two Cases Case Report Case Report 1Dewi KurniasariNo ratings yet
- MIDTERM EL. 109aDocument13 pagesMIDTERM EL. 109aYla MontealtoNo ratings yet
- Management A.1 EndometritisDocument5 pagesManagement A.1 Endometritisbhritany vidalNo ratings yet
- Peptic Ulcer Disease in Children: Dr. MaitaiDocument6 pagesPeptic Ulcer Disease in Children: Dr. MaitaiAlvin OmondiNo ratings yet
- 36 DysmenorrhoeDocument25 pages36 DysmenorrhoeNagamalar RajendraNo ratings yet
- Alteration in Reproductive SystemDocument35 pagesAlteration in Reproductive SystemSherds E ColasNo ratings yet
- Pharma (Done)Document19 pagesPharma (Done)YelNo ratings yet
- Mother & Child Health CareDocument5 pagesMother & Child Health CareGoogle BdNo ratings yet
- MSN Module 1Document15 pagesMSN Module 1Joey VenegasNo ratings yet
- Intro To OncologyDocument2 pagesIntro To Oncologyapi-534214500No ratings yet
- Leaflet Hiperplasia EndometriumDocument2 pagesLeaflet Hiperplasia EndometriumjefryNo ratings yet
- PID Sunilkumar Sreedevi ArchaDocument18 pagesPID Sunilkumar Sreedevi Archapk5bjbct8wNo ratings yet
- Drugs For Gastrointestinal DiseasesDocument4 pagesDrugs For Gastrointestinal DiseasesjeyNo ratings yet
- Medical Management of Closed Pyometra in A Bitch: A Case ReportDocument4 pagesMedical Management of Closed Pyometra in A Bitch: A Case ReportRonny Alberto GallegoNo ratings yet
- Abnormal Menses NotesDocument4 pagesAbnormal Menses NotesJunior VillNo ratings yet
- EsophagusDocument10 pagesEsophagusSherif shalabyNo ratings yet
- Upper Respiratory Disorders: ObjectivesDocument16 pagesUpper Respiratory Disorders: ObjectivesJennie QuachNo ratings yet
- SKENARIO 2 - Pelvic Inflammatory Disease REVISIDocument7 pagesSKENARIO 2 - Pelvic Inflammatory Disease REVISILidya IryaniNo ratings yet
- Krizelle CAPP 2Document2 pagesKrizelle CAPP 2Krizelle VaronaNo ratings yet
- En Dome Trios IsDocument13 pagesEn Dome Trios IsJerome Diplomatic NugentNo ratings yet
- Diagnostic Tests For EndometriosisDocument2 pagesDiagnostic Tests For EndometriosisApril Kirstin ChuaNo ratings yet
- Case StudyDocument3 pagesCase StudyGwyneth CartallaNo ratings yet
- MS Case PresDocument54 pagesMS Case PresShaine_Thompso_6877No ratings yet
- B.inggris Kel.6 3CDocument18 pagesB.inggris Kel.6 3CEmi LestariNo ratings yet
- NON-ALCOHOLIC FATTY LIVEr DISEASE (NAFLD) - NASHDocument4 pagesNON-ALCOHOLIC FATTY LIVEr DISEASE (NAFLD) - NASHJason FooNo ratings yet
- TRANS MSN Patient-in-SurgeryDocument6 pagesTRANS MSN Patient-in-SurgeryLezel LaracasNo ratings yet
- Preventing Opioid-Induced ConstipationDocument2 pagesPreventing Opioid-Induced Constipationaib reisNo ratings yet
- DR Ram Kumar Final Paper UploadDocument8 pagesDR Ram Kumar Final Paper Uploadrahumics256No ratings yet
- 39 Hormonal ContraceptionDocument36 pages39 Hormonal ContraceptionaweleNo ratings yet
- Background of The Condition:: Those That Put A Person at Risk of Developing A Problem)Document3 pagesBackground of The Condition:: Those That Put A Person at Risk of Developing A Problem)Genelly Anne Argañoza RamosNo ratings yet
- Patogesis EndometriosisDocument39 pagesPatogesis EndometriosisponekNo ratings yet
- MED THERA 3.02 - Pediatric TherapeuticsDocument6 pagesMED THERA 3.02 - Pediatric TherapeuticsRenz Francis SasaNo ratings yet
- T. Gastrointestinal DisordersDocument6 pagesT. Gastrointestinal DisordersJyl Yan SelasorNo ratings yet
- Contraceptive Implant: Prepared by Mohamed Liban YusufDocument2 pagesContraceptive Implant: Prepared by Mohamed Liban YusufMohamed LibanNo ratings yet
- Salin2 PPT ProposalDocument22 pagesSalin2 PPT ProposalSultan HSBNo ratings yet
- SGD Digestive SystemDocument3 pagesSGD Digestive SystemZH TVNo ratings yet
- OB - NCP (Episiotomy)Document3 pagesOB - NCP (Episiotomy)eosNo ratings yet
- En Dome Trios IsDocument42 pagesEn Dome Trios Isifer_018No ratings yet
- Arero Primary Hospital Pain MGT ProtocolDocument9 pagesArero Primary Hospital Pain MGT Protocolsami ketemaNo ratings yet
- Question - Bank - Pharmacology - SGS - 242.pdf - Filename - UTF-8''Question Bank Pharmacology SGS 242Document20 pagesQuestion - Bank - Pharmacology - SGS - 242.pdf - Filename - UTF-8''Question Bank Pharmacology SGS 242Mustafa SaßerNo ratings yet
- Medical Treatment of Endometriosis-Related PainDocument24 pagesMedical Treatment of Endometriosis-Related PainAgung SentosaNo ratings yet
- Relly Yanuari Primariawan, DR., SpOG (K) - Kenapa Penting Terapi Post Op Endometriosis-1Document38 pagesRelly Yanuari Primariawan, DR., SpOG (K) - Kenapa Penting Terapi Post Op Endometriosis-1oktavianusNo ratings yet
- Endometriosis: An Update On Management: ReviewDocument18 pagesEndometriosis: An Update On Management: Reviewxiaojun yangNo ratings yet
- Endometriosis & AdenomyosisDocument47 pagesEndometriosis & AdenomyosisAzim Syahmi Abd RazakNo ratings yet
- Ijerph 19 16148Document11 pagesIjerph 19 16148itziar.13.riveraNo ratings yet
- Management and InterventionDocument2 pagesManagement and InterventionPrincess C. SultanNo ratings yet
- Endometriosis: Li Qi LingDocument67 pagesEndometriosis: Li Qi LingwaheedaNo ratings yet
- Epp Bab 1-2Document17 pagesEpp Bab 1-2Ahmad BuchoriNo ratings yet
- The Development and Current Methods of Hormonal Birth ControlDocument9 pagesThe Development and Current Methods of Hormonal Birth ControllisacostaNo ratings yet
- Innovations in Conservative Endometriosis Treatment: An Updated ReviewDocument14 pagesInnovations in Conservative Endometriosis Treatment: An Updated ReviewparamitastellaNo ratings yet
- Oncology Skills Checklist: Name - DateDocument5 pagesOncology Skills Checklist: Name - DateMary ElizabethNo ratings yet
- Why Treat Only Ill PeopleDocument6 pagesWhy Treat Only Ill PeopleIona DarkNo ratings yet
- GynaeDocument8 pagesGynaeGokul DevNo ratings yet
- ContraceptiveDocument32 pagesContraceptiveediting visualsNo ratings yet
- Disorders of Eustachian TubeDocument21 pagesDisorders of Eustachian Tubeusmle prep100% (1)
- GAS No Resistance: PenicillinDocument4 pagesGAS No Resistance: Penicillinusmle prepNo ratings yet
- Suppression of Ovarian Activity With A Drospirenone-ContainingDocument10 pagesSuppression of Ovarian Activity With A Drospirenone-ContainingNegreanu AncaNo ratings yet
- 1 s2.0 S0010782417305383 MainDocument7 pages1 s2.0 S0010782417305383 MainCicilia Valentine SimamoraNo ratings yet
- Hormone Replacement Therapy (HRT)Document15 pagesHormone Replacement Therapy (HRT)LanaNo ratings yet
- Invoice Februari OtwDocument43 pagesInvoice Februari OtwAnnissa Puspa JNo ratings yet
- Stock OpnameDocument4 pagesStock OpnameDeka MaulyaniNo ratings yet
- DynaMed Plus - Endocrine Therapy For Early and Locally Advanced Breast CancerDocument50 pagesDynaMed Plus - Endocrine Therapy For Early and Locally Advanced Breast CancerGamer MadaNo ratings yet
- Infertility Management in Women With PolycysticDocument7 pagesInfertility Management in Women With PolycysticCarolina SidabutarNo ratings yet
- Drugs in Ovulation InductionDocument8 pagesDrugs in Ovulation InductionJeevs Music100% (1)
- DX Test de GNRH 2011Document6 pagesDX Test de GNRH 2011Sheyla Alegre ParionaNo ratings yet
- Modelo UnidadesDocument64 pagesModelo UnidadesRafael MagalhãesNo ratings yet
- Janeiro - 24 US Coach - XLSBDocument8 pagesJaneiro - 24 US Coach - XLSBfiscalNo ratings yet
- Nappi - Vaginal Ring in Contraception, New AdvantagesDocument53 pagesNappi - Vaginal Ring in Contraception, New AdvantagesBeatriz Eugenia NavarroNo ratings yet
- 55 60Document5 pages55 60Jihad MalikNo ratings yet
- Reproductive System Related DrugsDocument5 pagesReproductive System Related DrugsNoor AlsheikhNo ratings yet
- Bp503t Pcol Unit-VDocument46 pagesBp503t Pcol Unit-VAakkkNo ratings yet
- FSRH Guidance Switching or Starting Methods of Contraception August 2019Document10 pagesFSRH Guidance Switching or Starting Methods of Contraception August 2019Ting Yiu WongNo ratings yet
- HORMON REPRODUKSI DAN SIKLUS HAID Prof. Dr. Dr. Nusratuddin Abdullah, SP - OG (K) MARSDocument21 pagesHORMON REPRODUKSI DAN SIKLUS HAID Prof. Dr. Dr. Nusratuddin Abdullah, SP - OG (K) MARStenri olaNo ratings yet
- Superior PDFDocument5 pagesSuperior PDFmhgc108210No ratings yet
- Evidace Based ECDocument15 pagesEvidace Based ECRana Yuda StiraNo ratings yet
- Generic Name:: Norgestimate and Ethinyl EstradiolDocument5 pagesGeneric Name:: Norgestimate and Ethinyl EstradiolJay VillasotoNo ratings yet
- PHARCHEM2 LIST Hormones To Cardiovascular DrugsDocument7 pagesPHARCHEM2 LIST Hormones To Cardiovascular DrugsLA BriguelaNo ratings yet
- Lecture 9 Endocrine HormonesDocument18 pagesLecture 9 Endocrine HormonesKC PalattaoNo ratings yet
- Female Sex HormonesDocument20 pagesFemale Sex HormonesAlina ShahNo ratings yet
- Anticancer Hormones & AntagonistsDocument27 pagesAnticancer Hormones & AntagonistsBob MuneneNo ratings yet
- The Ultimate PCT Supplement (Hpta Restoration) - Looksmax - Org - Men's Self-Improvement & AestheticsDocument25 pagesThe Ultimate PCT Supplement (Hpta Restoration) - Looksmax - Org - Men's Self-Improvement & Aestheticskrakesh7848No ratings yet