You might also like
- The Whartons' Strength Book: Lower Body: Total Stability for Upper Legs, Hips, Trunk, Lower Legs, Ankles, and FeetFrom EverandThe Whartons' Strength Book: Lower Body: Total Stability for Upper Legs, Hips, Trunk, Lower Legs, Ankles, and FeetRating: 3 out of 5 stars3/5 (3)
- Patellofemoral/Chondromalacia Protocol: Anatomy and BiomechanicsDocument8 pagesPatellofemoral/Chondromalacia Protocol: Anatomy and BiomechanicsGirijashankar KhuntiaNo ratings yet
- The Whartons' Strength Book: Upper Body: Total Stability for Shoulders, Neck, Arm, Wrist, and ElbowFrom EverandThe Whartons' Strength Book: Upper Body: Total Stability for Shoulders, Neck, Arm, Wrist, and ElbowRating: 5 out of 5 stars5/5 (1)
- Hip OA Rehab: A 4-Phase Guide to RecoveryDocument7 pagesHip OA Rehab: A 4-Phase Guide to RecoveryPaul Radulescu - FizioterapeutNo ratings yet
- Exercises for Those Who Suffer a Disk HerniaFrom EverandExercises for Those Who Suffer a Disk HerniaRating: 5 out of 5 stars5/5 (2)
- Lumbar Disc HerniationDocument8 pagesLumbar Disc Herniationandra_scooterNo ratings yet
- ACL Non-Operative ManagmentDocument10 pagesACL Non-Operative ManagmentHammad -ullahNo ratings yet
- The Athlete's Guide to Stretching: Increasing Flexibility For Inury Prevention And RehabilitationFrom EverandThe Athlete's Guide to Stretching: Increasing Flexibility For Inury Prevention And RehabilitationRating: 4 out of 5 stars4/5 (1)
- Rotator Cuff Impingement/Tendinopathy Rehab GuideDocument8 pagesRotator Cuff Impingement/Tendinopathy Rehab GuidemadaleenNo ratings yet
- HK11 Jumpers KneeDocument7 pagesHK11 Jumpers KneeDestinee LegendsNo ratings yet
- Dynamic Stretching: The Revolutionary New Warm-up Method to Improve Power, Performance and Range of MotionFrom EverandDynamic Stretching: The Revolutionary New Warm-up Method to Improve Power, Performance and Range of MotionRating: 5 out of 5 stars5/5 (1)
- Tennis Elbow RehabDocument8 pagesTennis Elbow RehabDarren Willis100% (2)
- Power Flex Stretching - Super Flexibility and Strength for peak performanceFrom EverandPower Flex Stretching - Super Flexibility and Strength for peak performanceRating: 3 out of 5 stars3/5 (3)
- Treatment: Home TreatmentsDocument3 pagesTreatment: Home TreatmentsDhimas Reyhan Putra SayudhaNo ratings yet
- Frozen Shoulder GuideDocument8 pagesFrozen Shoulder GuidefriskaNo ratings yet
- DYNAMIC LUMBAR STABILIZATION TRAINING Dean Farwood, P.T.Document5 pagesDYNAMIC LUMBAR STABILIZATION TRAINING Dean Farwood, P.T.Luis Eduardo Barbosa OrtegaNo ratings yet
- Physical Fitness Notes Second AssessmentDocument116 pagesPhysical Fitness Notes Second AssessmentElena JordanovaNo ratings yet
- How to Treat a Sprained AnkleDocument4 pagesHow to Treat a Sprained AnkleSakthi Annamalai.cNo ratings yet
- Quadriceps Muscle Strain GuideDocument16 pagesQuadriceps Muscle Strain GuideAZOZ 19No ratings yet
- A Weighty Subject: The Ergonomics of Resistance TrainingDocument4 pagesA Weighty Subject: The Ergonomics of Resistance TrainingmailbabuNo ratings yet
- Trunk Stabilization ProgramDocument20 pagesTrunk Stabilization ProgramLate ArtistNo ratings yet
- North American Spine Society Public Education SeriesDocument12 pagesNorth American Spine Society Public Education SeriesVanitha Ratha KrishnanNo ratings yet
- Patella TendonitisDocument43 pagesPatella Tendonitisvijkris1985100% (2)
- Training System For Enhancing Athletic Performance Al VermeilDocument165 pagesTraining System For Enhancing Athletic Performance Al Vermeilxaviermay100% (7)
- Effective Martial Arts - Training With No Equipment or Partner Vol 2 - Ageless Flexibility and Joint MobilityDocument74 pagesEffective Martial Arts - Training With No Equipment or Partner Vol 2 - Ageless Flexibility and Joint MobilityTamil Vanan NNo ratings yet
- 2010 Rehabilitation of Ankle and FootDocument11 pages2010 Rehabilitation of Ankle and FootRodrigo GarcíaNo ratings yet
- Resistance Exercise For Impaired Muscle Performance: Chapter No 6 DR - Iqra Ashraf DPT, MS-MSKDocument29 pagesResistance Exercise For Impaired Muscle Performance: Chapter No 6 DR - Iqra Ashraf DPT, MS-MSKSania SaeedNo ratings yet
- Swimmer's Shoulder - StatPearlsDocument4 pagesSwimmer's Shoulder - StatPearlsFillipe AgraNo ratings yet
- نسخة light blue creative modern medical clinic presentationDocument33 pagesنسخة light blue creative modern medical clinic presentationFaresNo ratings yet
- Acromioclavicular Joint Injuries and Physical Therapy ManagementDocument12 pagesAcromioclavicular Joint Injuries and Physical Therapy ManagementSereinNo ratings yet
- Hamstring MuscleDocument8 pagesHamstring MuscleMuhamad SdeqNo ratings yet
- Manual Muscle TestingDocument29 pagesManual Muscle Testingcreat1No ratings yet
- Connecting the Core Muscles for Stability and PerformanceDocument5 pagesConnecting the Core Muscles for Stability and PerformanceManos GladxNo ratings yet
- Knee Arthroscopy Meniscectomy Recovery GuideDocument9 pagesKnee Arthroscopy Meniscectomy Recovery Guidebayan salahNo ratings yet
- Strong As An Ox Olympic Weightlifting Program Manual PDFDocument32 pagesStrong As An Ox Olympic Weightlifting Program Manual PDFJonathan Schroeder80% (5)
- Low Back Health through Stabilization ExercisesDocument8 pagesLow Back Health through Stabilization ExercisesDavid StadkindNo ratings yet
- Patellar Tendon Rupture and RehabilitationDocument4 pagesPatellar Tendon Rupture and RehabilitationdedsnetNo ratings yet
- Physiotherapy For Quadriceps Tendon TearDocument2 pagesPhysiotherapy For Quadriceps Tendon TearenadNo ratings yet
- Spine Stabilization PowerpointDocument87 pagesSpine Stabilization PowerpointALLAN COSTA MONTEIRONo ratings yet
- Lower Crossed SyndromeDocument8 pagesLower Crossed SyndromeThaseen75% (4)
- Sports Injuries in UE - Shoulder - Part 3.Document87 pagesSports Injuries in UE - Shoulder - Part 3.salmankhan09215No ratings yet
- Preventing Dance Injuries Through Proper Technique and Self-CareDocument12 pagesPreventing Dance Injuries Through Proper Technique and Self-CareKashima KotaroNo ratings yet
- Hamstring Exercise ProgressionDocument15 pagesHamstring Exercise ProgressionFrancisco De VelascoNo ratings yet
- Therapeutic Gymnasium PDFDocument45 pagesTherapeutic Gymnasium PDFPrabhat SharmaNo ratings yet
- Post-Op Hip Active-Assisted Exercise ProgramDocument3 pagesPost-Op Hip Active-Assisted Exercise ProgramAhmad AfiyyuddinNo ratings yet
- Patellectomy RehabDocument29 pagesPatellectomy RehabKhateeja Tul KubraNo ratings yet
- Frozen ShoulderDocument6 pagesFrozen ShoulderanumolNo ratings yet
- Patellar Tendonitis TreatmentDocument7 pagesPatellar Tendonitis TreatmentRatnaPrasadNalamNo ratings yet
- Prevención de Pubalgia Atlética y Dolor Crónico en La Ingle en Jugadores de FútbolDocument4 pagesPrevención de Pubalgia Atlética y Dolor Crónico en La Ingle en Jugadores de FútbolFloren Martil GuijarroNo ratings yet
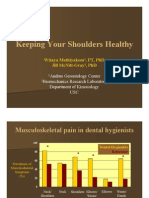
- Keeping Your Shoulders HealthyDocument38 pagesKeeping Your Shoulders Healthyxyz84No ratings yet
- Long Thoracic Nerve PalsyDocument2 pagesLong Thoracic Nerve PalsyJose Luis Tabueña OrtegaNo ratings yet
- 14 Exercises That Can Worsen HealthDocument4 pages14 Exercises That Can Worsen HealthNmorah QandilNo ratings yet
- Coastal Iliotibial Band 2014Document2 pagesCoastal Iliotibial Band 2014lesterbsbNo ratings yet
- Fasa Akut Selepas PembedahanDocument4 pagesFasa Akut Selepas Pembedahanchris waddleNo ratings yet
- Post Op Cervical Fusion PDFDocument3 pagesPost Op Cervical Fusion PDFNICOLÁS ANDRÉS AYELEF PARRAGUEZNo ratings yet
- How To Maintain Good Knee Joint Health 20160708Document6 pagesHow To Maintain Good Knee Joint Health 20160708rarNo ratings yet
- StretchingDocument32 pagesStretchingTofan Ana88% (8)
- Off-Campus Placement ProjectDocument4 pagesOff-Campus Placement Projectapi-488042467No ratings yet
- Short-Term Effects of Mobilization-With-Movement (MWM) and Auto-Mwm Application in Recreational Runners With Iliotibial Band SyndromeDocument8 pagesShort-Term Effects of Mobilization-With-Movement (MWM) and Auto-Mwm Application in Recreational Runners With Iliotibial Band SyndromeRia PuputNo ratings yet
- ITband Exercises PDFDocument2 pagesITband Exercises PDFShashNo ratings yet
- RPW Shockwave Therapy: Scientific Studies OverviewDocument38 pagesRPW Shockwave Therapy: Scientific Studies OverviewRia Puput100% (1)
- ITBSReview Article RLBRSMFPMR2011Document13 pagesITBSReview Article RLBRSMFPMR2011Ria PuputNo ratings yet
- Low Back Pain: Information For PatientsDocument8 pagesLow Back Pain: Information For PatientsShibli RahmanNo ratings yet
- 0207 ProlotherapyDocument36 pages0207 ProlotherapyRia PuputNo ratings yet
- Effect of Hip Abductor Strengthening Among Non-Professional Cyclists With Iliotibial Band Friction SyndromeDocument11 pagesEffect of Hip Abductor Strengthening Among Non-Professional Cyclists With Iliotibial Band Friction SyndromeRia PuputNo ratings yet
- Closed kinetic exercises improve knee proprioceptionDocument3 pagesClosed kinetic exercises improve knee proprioceptionRia PuputNo ratings yet
- ACR OA Guideline Development Process Knee and HipDocument8 pagesACR OA Guideline Development Process Knee and HipAulia Satria BimantaraNo ratings yet
- Constraining Kinematics During Single-Leg Squats and Step-Ups CanDocument56 pagesConstraining Kinematics During Single-Leg Squats and Step-Ups CanRia PuputNo ratings yet
- Osteoarthritis of The Knee Information Booklet PDFDocument36 pagesOsteoarthritis of The Knee Information Booklet PDFRia PuputNo ratings yet
- Effectiveness of Combined Chain Exercises On PainDocument11 pagesEffectiveness of Combined Chain Exercises On PainJulenda CintarinovaNo ratings yet
- Corrective Exercises in The Treatment of Scoliosis PDFDocument21 pagesCorrective Exercises in The Treatment of Scoliosis PDFRia PuputNo ratings yet
- Home Exercise Program for ScoliosisDocument6 pagesHome Exercise Program for ScoliosisChris SakeNo ratings yet
- Foot and Ankle Ability Measure PDFDocument3 pagesFoot and Ankle Ability Measure PDFFirda Dwi AzizahNo ratings yet
- Static Balance Normsin ChildrenDocument8 pagesStatic Balance Normsin ChildrenRia PuputNo ratings yet
- Ijpr 2018 145Document7 pagesIjpr 2018 145Ria PuputNo ratings yet
- SimpleSet Exercise Program Grid Template SampleDocument2 pagesSimpleSet Exercise Program Grid Template SampleRia PuputNo ratings yet
- Hydrotherapy For LBP FixxDocument22 pagesHydrotherapy For LBP FixxRia PuputNo ratings yet
- 1062 6050 555 16Document10 pages1062 6050 555 16Ria PuputNo ratings yet
- A 4 Shoulder Impinge Appendix 5Document8 pagesA 4 Shoulder Impinge Appendix 5NatuNo ratings yet
- Chest Physiotherapy in Intensive Care Unit (ICU) PDFDocument399 pagesChest Physiotherapy in Intensive Care Unit (ICU) PDFGuillermo Sasso Pacheco83% (6)
- BiomekanikDocument16 pagesBiomekanikRia PuputNo ratings yet
- Hortatory ExpositionDocument7 pagesHortatory ExpositionRia PuputNo ratings yet
- Cat Muscles Study GuideDocument28 pagesCat Muscles Study Guidearvinric100% (1)
- Peranan Fisioterapi Pada Kasus Hallux Valgus (Bunion) Dengan Intervensi NMT Dan Strengthening Untuk Mengurangi NyeriDocument7 pagesPeranan Fisioterapi Pada Kasus Hallux Valgus (Bunion) Dengan Intervensi NMT Dan Strengthening Untuk Mengurangi NyeriShalmaa LarasatiNo ratings yet
- Medial Patellofemoral Ligament MPFLDocument8 pagesMedial Patellofemoral Ligament MPFLImran AshrafNo ratings yet
- Screen Knee Issues for Potential Serious ConditionsDocument120 pagesScreen Knee Issues for Potential Serious Conditionssayles4174100% (1)
- Medical Tests, Signs & Maneuvers Guide: Achilles Squeeze TestDocument12 pagesMedical Tests, Signs & Maneuvers Guide: Achilles Squeeze TestWaqar AhmedNo ratings yet
- The Great and Mysterious ButtDocument6 pagesThe Great and Mysterious ButtaggybongNo ratings yet
- The Asics Natural Running GuideDocument15 pagesThe Asics Natural Running GuideJavalinoshopNo ratings yet
- Ligamento Cruzado Doble FasciculoDocument16 pagesLigamento Cruzado Doble FasciculoAuusto CórdobaNo ratings yet
- Snell Lower Limb Questions AnswersDocument6 pagesSnell Lower Limb Questions AnswersBen95% (37)
- ACIIDA - SP - 1 Direct Anterior ApproachDocument30 pagesACIIDA - SP - 1 Direct Anterior ApproachJayjeet BhoiteNo ratings yet
- Foot DropDocument30 pagesFoot Dropdr_s_ganesh100% (1)
- Genu ValgumDocument3 pagesGenu ValgumBiniam AssefaNo ratings yet
- Foot Orthoses and Other Forms of Conservative Foot CareDocument262 pagesFoot Orthoses and Other Forms of Conservative Foot CareJorge Aguirre Gonzalez100% (1)
- Muscle Flash CardsDocument127 pagesMuscle Flash Cardsjoelh9100% (3)
- Foot Anatomy and PhysiologyDocument9 pagesFoot Anatomy and PhysiologyMarta BłaszczykNo ratings yet
- Treatment and Rehabilitation of Fractures (Stanley Hoppenfeld)Document1 pageTreatment and Rehabilitation of Fractures (Stanley Hoppenfeld)小蓮花No ratings yet
- Squat TestDocument5 pagesSquat TestLuis Espinoza Aramburú100% (1)
- Most Common Surfing Injuries and Accidents - SurflineDocument2 pagesMost Common Surfing Injuries and Accidents - Surflineapi-549909228No ratings yet
- Physical Examination of Knee Ligament Injuries: Review ArticleDocument8 pagesPhysical Examination of Knee Ligament Injuries: Review ArticlenuriajunitNo ratings yet
- Arteries of Lower LimbDocument6 pagesArteries of Lower LimbAlli NdahuraNo ratings yet
- Department of Anatomy Hasanuddin University: Dr. Hasan NyambeDocument57 pagesDepartment of Anatomy Hasanuddin University: Dr. Hasan NyambeMaksi YantoNo ratings yet
- Knee Pain Internal ArtsDocument7 pagesKnee Pain Internal ArtsGabriel PedrozaNo ratings yet
- Ortho TestsDocument23 pagesOrtho TestsAMIRSAM SHAHHOSSEININo ratings yet
- Anatomy of the Lower LimbsDocument84 pagesAnatomy of the Lower LimbsAlviraNo ratings yet
- TFC Seminar Manual (Online)Document5 pagesTFC Seminar Manual (Online)Emanuel SortinoNo ratings yet
- The Ankle in Football - 2014 PDFDocument326 pagesThe Ankle in Football - 2014 PDFRobert TănăsescuNo ratings yet
- Anatomy, Bony Pelvis and Lower Limb, Leg Bones: February 2019Document8 pagesAnatomy, Bony Pelvis and Lower Limb, Leg Bones: February 2019Chess NutsNo ratings yet
- The Human Foot Anatomy, Deformities and Treatment A Volume Containing A Complete and Comprehensive Description of The Anatomy of The FootDocument402 pagesThe Human Foot Anatomy, Deformities and Treatment A Volume Containing A Complete and Comprehensive Description of The Anatomy of The FootEjup MajollariNo ratings yet
- Case PresentationDocument19 pagesCase PresentationIbad Ur RehmanNo ratings yet
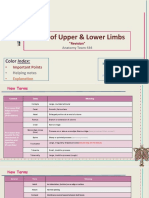
- Bones of Upper and Lower Limbs - RevisionDocument15 pagesBones of Upper and Lower Limbs - RevisionChess Nuts100% (1)
- Chakras and Yoga: Finding Inner Harmony Through Practice, Awaken the Energy Centers for Optimal Physical and Spiritual Health.From EverandChakras and Yoga: Finding Inner Harmony Through Practice, Awaken the Energy Centers for Optimal Physical and Spiritual Health.Rating: 4 out of 5 stars4/5 (2)
- Functional Training and Beyond: Building the Ultimate Superfunctional Body and MindFrom EverandFunctional Training and Beyond: Building the Ultimate Superfunctional Body and MindRating: 4.5 out of 5 stars4.5/5 (1)
- Body by Science: A Research Based Program for Strength Training, Body building, and Complete Fitness in 12 Minutes a WeekFrom EverandBody by Science: A Research Based Program for Strength Training, Body building, and Complete Fitness in 12 Minutes a WeekRating: 4.5 out of 5 stars4.5/5 (84)
- Boundless: Upgrade Your Brain, Optimize Your Body & Defy AgingFrom EverandBoundless: Upgrade Your Brain, Optimize Your Body & Defy AgingRating: 4.5 out of 5 stars4.5/5 (66)
- Chair Yoga: Sit, Stretch, and Strengthen Your Way to a Happier, Healthier YouFrom EverandChair Yoga: Sit, Stretch, and Strengthen Your Way to a Happier, Healthier YouRating: 3.5 out of 5 stars3.5/5 (5)
- Strong Is the New Beautiful: Embrace Your Natural Beauty, Eat Clean, and Harness Your PowerFrom EverandStrong Is the New Beautiful: Embrace Your Natural Beauty, Eat Clean, and Harness Your PowerRating: 4 out of 5 stars4/5 (5)
- The Yogi Code: Seven Universal Laws of Infinite SuccessFrom EverandThe Yogi Code: Seven Universal Laws of Infinite SuccessRating: 4.5 out of 5 stars4.5/5 (104)
- Endure: Mind, Body, and the Curiously Elastic Limits of Human PerformanceFrom EverandEndure: Mind, Body, and the Curiously Elastic Limits of Human PerformanceRating: 4.5 out of 5 stars4.5/5 (237)
- Wall Pilates: Quick-and-Simple to Lose Weight and Stay Healthy. A 30-Day Journey with + 100 ExercisesFrom EverandWall Pilates: Quick-and-Simple to Lose Weight and Stay Healthy. A 30-Day Journey with + 100 ExercisesNo ratings yet
- Hero Maker: 12 Weeks to Superhero Fit: A Hollywood Trainer's REAL Guide to Getting the Body You've Always WantedFrom EverandHero Maker: 12 Weeks to Superhero Fit: A Hollywood Trainer's REAL Guide to Getting the Body You've Always WantedRating: 4 out of 5 stars4/5 (1)
- Muscle for Life: Get Lean, Strong, and Healthy at Any Age!From EverandMuscle for Life: Get Lean, Strong, and Healthy at Any Age!Rating: 4.5 out of 5 stars4.5/5 (22)
- Power of 10: The Once-A-Week Slow Motion Fitness RevolutionFrom EverandPower of 10: The Once-A-Week Slow Motion Fitness RevolutionRating: 3.5 out of 5 stars3.5/5 (11)
- 7 Weeks to 10 Pounds of Muscle: The Complete Day-by-Day Program to Pack on Lean, Healthy Muscle MassFrom Everand7 Weeks to 10 Pounds of Muscle: The Complete Day-by-Day Program to Pack on Lean, Healthy Muscle MassRating: 4 out of 5 stars4/5 (2)
- Peak: The New Science of Athletic Performance That is Revolutionizing SportsFrom EverandPeak: The New Science of Athletic Performance That is Revolutionizing SportsRating: 5 out of 5 stars5/5 (95)
- Relentless: From Good to Great to UnstoppableFrom EverandRelentless: From Good to Great to UnstoppableRating: 5 out of 5 stars5/5 (781)
- If You Like Exercise … Chances Are You’Re Doing It Wrong: Proper Strength Training for Maximum ResultsFrom EverandIf You Like Exercise … Chances Are You’Re Doing It Wrong: Proper Strength Training for Maximum ResultsRating: 4.5 out of 5 stars4.5/5 (7)
- Yamas & Niyamas: Exploring Yoga's Ethical PracticeFrom EverandYamas & Niyamas: Exploring Yoga's Ethical PracticeRating: 4.5 out of 5 stars4.5/5 (110)
- SAS Training Manual: How to get fit enough to pass a special forces selection courseFrom EverandSAS Training Manual: How to get fit enough to pass a special forces selection courseRating: 4 out of 5 stars4/5 (3)
- Meat Is for Pussies: A How-To Guide for Dudes Who Want to Get Fit, Kick Ass, and Take NamesFrom EverandMeat Is for Pussies: A How-To Guide for Dudes Who Want to Get Fit, Kick Ass, and Take NamesRating: 3.5 out of 5 stars3.5/5 (8)
- Calisthenics: 12 Effective Exercises to Build Calisthenics Body in 14 DaysFrom EverandCalisthenics: 12 Effective Exercises to Build Calisthenics Body in 14 DaysRating: 3 out of 5 stars3/5 (5)
- The Calisthenics Codex: Fifty Exercises for Functional FitnessFrom EverandThe Calisthenics Codex: Fifty Exercises for Functional FitnessRating: 4 out of 5 stars4/5 (9)
- Calisthenics: Guide for Bodyweight Exercise, Build your Dream Body in 30 MinutesFrom EverandCalisthenics: Guide for Bodyweight Exercise, Build your Dream Body in 30 MinutesRating: 3 out of 5 stars3/5 (5)
- 7 Weeks to 50 Pull-Ups: Strengthen and Sculpt Your Arms, Shoulders, Back, and Abs by Training to Do 50 Consecutive Pull-UpsFrom Everand7 Weeks to 50 Pull-Ups: Strengthen and Sculpt Your Arms, Shoulders, Back, and Abs by Training to Do 50 Consecutive Pull-UpsRating: 3.5 out of 5 stars3.5/5 (2)
- Applied Polyvagal Theory in Yoga: Therapeutic Practices for Emotional HealthFrom EverandApplied Polyvagal Theory in Yoga: Therapeutic Practices for Emotional HealthNo ratings yet
- Deezify's Epic Workout Handbook: An Illustrated Guide to Getting SwoleFrom EverandDeezify's Epic Workout Handbook: An Illustrated Guide to Getting SwoleRating: 5 out of 5 stars5/5 (1)
- Beastmode Calisthenics: A Simple and Effective Guide to Get Ripped with Bodyweight TrainingFrom EverandBeastmode Calisthenics: A Simple and Effective Guide to Get Ripped with Bodyweight TrainingNo ratings yet