You might also like
- Stage 5 Aboriginal Studies - Redfern Now Teachers GuideDocument65 pagesStage 5 Aboriginal Studies - Redfern Now Teachers Guideapi-327869042100% (1)
- Recovery From Narcissistic Abuse Through PDFDocument8 pagesRecovery From Narcissistic Abuse Through PDFBojan Nikolik100% (1)
- Nostalgia: The Bittersweet History of A Psychological ConceptDocument12 pagesNostalgia: The Bittersweet History of A Psychological ConceptRebecca Dance100% (2)
- History Taking in PsychiatryDocument3 pagesHistory Taking in PsychiatryJuan Cruz FenrirNo ratings yet
- Malingering in Psychiatric DisordersDocument4 pagesMalingering in Psychiatric DisordersStuti JoshiNo ratings yet
- Aggressivity, Narcissism, and Self-Destructiveness in The Psychotherapeutic Relationship - Otto KernbergDocument27 pagesAggressivity, Narcissism, and Self-Destructiveness in The Psychotherapeutic Relationship - Otto Kernbergvgimbe100% (1)
- Bernard Gallagher Cap. 5 Sociology of Mental IllnessDocument16 pagesBernard Gallagher Cap. 5 Sociology of Mental IllnessLaura CristinaNo ratings yet
- FOREVER MARKED A Dermatillomania DiaryDocument152 pagesFOREVER MARKED A Dermatillomania DiaryOsana Angelita ValandroNo ratings yet
- Intermittent Explosive DisorderDocument9 pagesIntermittent Explosive Disorders784tiwariNo ratings yet
- Intermittentexplosive Disorderasa Disorderof Impulsive Aggression Fordsm-5Document12 pagesIntermittentexplosive Disorderasa Disorderof Impulsive Aggression Fordsm-5nurulamaliahNo ratings yet
- West and Friedman, 2008Document6 pagesWest and Friedman, 2008tim radellNo ratings yet
- PSYCHIATRIC SERVICES©June 1999 Vol. 50 No. 6787psychopathy and Violent BehaviorAmong Patients With Schizophrenia or Schizoaffective DisorderDocument6 pagesPSYCHIATRIC SERVICES©June 1999 Vol. 50 No. 6787psychopathy and Violent BehaviorAmong Patients With Schizophrenia or Schizoaffective DisorderjudithbatallaNo ratings yet
- LevensonDocument8 pagesLevensonDidascalosNo ratings yet
- Stuart 2003 Enf Mental ViolenciaDocument4 pagesStuart 2003 Enf Mental ViolenciaJaime Fernández-AguirrebengoaNo ratings yet
- Hysterical PsychosisDocument8 pagesHysterical PsychosisalfonsougarteNo ratings yet
- Criminal PsychologyDocument40 pagesCriminal Psychologysknawab620No ratings yet
- Psychological Mechanisms Mediating Effects Between Trauma and PsychoticDocument10 pagesPsychological Mechanisms Mediating Effects Between Trauma and PsychoticifclarinNo ratings yet
- Forensic PsychologyDocument22 pagesForensic PsychologyCayabyab, Leif Azhley S.No ratings yet
- Beck (2005) The Current State of Cognitive TherapyDocument7 pagesBeck (2005) The Current State of Cognitive TherapyJavieraRamírezSánchezNo ratings yet
- Appraisal and Control of Sexual and Non-Sexual Intrusive Thoughts in University StudentsDocument17 pagesAppraisal and Control of Sexual and Non-Sexual Intrusive Thoughts in University StudentsYen-ßhäing ChiüNo ratings yet
- Zuckerman, M (1989) Personality in The Third Dimension A Psychobiological ApproachDocument28 pagesZuckerman, M (1989) Personality in The Third Dimension A Psychobiological ApproachMariana ArismendiNo ratings yet
- Cognitive Distortions and Suicide AttemptsDocument6 pagesCognitive Distortions and Suicide AttemptsMihaela AndreiNo ratings yet
- Pietrzak 2013Document1 pagePietrzak 2013MikerenNo ratings yet
- NIH Public AccessDocument12 pagesNIH Public AccessNabila alfaishaNo ratings yet
- HannibalDocument9 pagesHannibalAbigail Rojas RNo ratings yet
- Akiskal 1983Document10 pagesAkiskal 1983Shandy PutraNo ratings yet
- Affect, Risk, and Decision Making: Paul Slovic and Ellen Peters Melissa L. FinucaneDocument6 pagesAffect, Risk, and Decision Making: Paul Slovic and Ellen Peters Melissa L. FinucaneBrick HartNo ratings yet
- The Current State of Cognitive Therapy: A 40-Year RetrospectiveDocument7 pagesThe Current State of Cognitive Therapy: A 40-Year RetrospectiveSandro Alcobaça100% (1)
- P3 Event-Related Potentials and Childhood Maltreatment in Successful and Unsuccessful PsychopathsDocument7 pagesP3 Event-Related Potentials and Childhood Maltreatment in Successful and Unsuccessful PsychopathsPedro SilvaNo ratings yet
- The Responsibility of The Psychopathy RevisitedDocument11 pagesThe Responsibility of The Psychopathy RevisitedJuan Carlos T'ang VenturónNo ratings yet
- Perception of Causality in Schizophrenia PDFDocument7 pagesPerception of Causality in Schizophrenia PDFBojan NikolikNo ratings yet
- Psycopath RecoversDocument48 pagesPsycopath RecoversBioestatística Mestrado UFRJNo ratings yet
- Dissociation Affect Dysregulation Somatization BVDKDocument22 pagesDissociation Affect Dysregulation Somatization BVDKkanuNo ratings yet
- Premeditated Paper, 2003Document10 pagesPremeditated Paper, 2003Sebastián ReyesNo ratings yet
- Malingering 4Document7 pagesMalingering 4Vedora Angelia GultomNo ratings yet
- Aadya Tiwari - The Influence of Psychopathic Traits On Homicidal BehaviorDocument7 pagesAadya Tiwari - The Influence of Psychopathic Traits On Homicidal Behavior27tiwariaNo ratings yet
- ERQ Plan - Etiologies of PTSDDocument3 pagesERQ Plan - Etiologies of PTSDRudy CookNo ratings yet
- NIH Public AccessDocument13 pagesNIH Public AccessJuan Alberto GonzálezNo ratings yet
- Lynn1984 Nonvolition Expectancies and Hypnotic RapportDocument9 pagesLynn1984 Nonvolition Expectancies and Hypnotic Rapportgambit71No ratings yet
- Bem2011 PDFDocument19 pagesBem2011 PDFCristina RîndașuNo ratings yet
- Malingering: Avoidance of Criminal Responsibility, Trial, and PunishmentDocument4 pagesMalingering: Avoidance of Criminal Responsibility, Trial, and PunishmentPridina Syadirah100% (1)
- 2019 Lukasz PDFDocument24 pages2019 Lukasz PDFnermal93No ratings yet
- Assignment Reference Material (2020-21) BPCE - 014 PsychopathologyDocument9 pagesAssignment Reference Material (2020-21) BPCE - 014 PsychopathologyAnjnaKandariNo ratings yet
- J.E. Kennedy - (Response To Letter On Capricious Psi)Document2 pagesJ.E. Kennedy - (Response To Letter On Capricious Psi)Mytee8888No ratings yet
- Halusi JurnalDocument16 pagesHalusi JurnalVitta ChusmeywatiNo ratings yet
- Images Videos Quizzes ListsDocument6 pagesImages Videos Quizzes ListsshavikNo ratings yet
- Paranoid Personality Disorder: Case ReportDocument3 pagesParanoid Personality Disorder: Case ReporttTTNo ratings yet
- Suicidal Behavior in Latency-Age Children: An StudyDocument14 pagesSuicidal Behavior in Latency-Age Children: An StudyAdriánMadrigalNo ratings yet
- Abnormal Psychology - ReviewerDocument16 pagesAbnormal Psychology - ReviewerVanessa GabonNo ratings yet
- Schizophrenia FinalDocument9 pagesSchizophrenia Finalapi-285384246No ratings yet
- Impulsivity: A Predisposition Toward Risky Behaviors: Nour-Mohammad BakhshaniDocument3 pagesImpulsivity: A Predisposition Toward Risky Behaviors: Nour-Mohammad BakhshaniCoordinacionPsicologiaVizcayaGuaymasNo ratings yet
- Anderson 2014Document16 pagesAnderson 2014Bárbara FernandesNo ratings yet
- Cognitive Emotional and Social Processes in PsychosisDocument8 pagesCognitive Emotional and Social Processes in Psychosishelen.ashton5No ratings yet
- Moelleretal 2001psychiatricaspectsofimpulsivityDocument12 pagesMoelleretal 2001psychiatricaspectsofimpulsivityZavršni radNo ratings yet
- Decety Et Al. (2013)Document8 pagesDecety Et Al. (2013)Micaela TaverniniNo ratings yet
- Ika MaulizaDocument7 pagesIka MaulizaIka MaulizaNo ratings yet
- Ika MaulizaDocument7 pagesIka MaulizaIka MaulizaNo ratings yet
- 2011 - The Criminal Psychopath - History, Neuroscience, Treatment, and EconomicsDocument49 pages2011 - The Criminal Psychopath - History, Neuroscience, Treatment, and EconomicsKarina FigueiredoNo ratings yet
- Psychopathological Mechanisms Linking Childhood Traumatic ExperiencesDocument8 pagesPsychopathological Mechanisms Linking Childhood Traumatic Experiencessaurav.das2030No ratings yet
- Daniel Freeman, Understanding+and+TreatmentDocument24 pagesDaniel Freeman, Understanding+and+TreatmentDNNo ratings yet
- Schizo 3Document11 pagesSchizo 3Aldy GeriNo ratings yet
- Unmasking Feigned Sanity A Neurobiological Model of Emotion Processing in Primary PsychopathyDocument23 pagesUnmasking Feigned Sanity A Neurobiological Model of Emotion Processing in Primary PsychopathyAnna BezhanishviliNo ratings yet
- Bear Fedio PDFDocument14 pagesBear Fedio PDFPaula HarrisNo ratings yet
- Using The Psychopathy Checklist-Revised With Female Samples: Reliability, Validity, and Implications For Clinical UtilityDocument16 pagesUsing The Psychopathy Checklist-Revised With Female Samples: Reliability, Validity, and Implications For Clinical UtilityIsa Abu YahyaNo ratings yet
- Adolescent Suicide and Self-Injury: Mentalizing Theory and TreatmentFrom EverandAdolescent Suicide and Self-Injury: Mentalizing Theory and TreatmentLaurel L. WilliamsNo ratings yet
- RamelteonProductLabel 1218 PDFDocument18 pagesRamelteonProductLabel 1218 PDFLeslie CitromeNo ratings yet
- RamelteonProductLabel 1218 PDFDocument18 pagesRamelteonProductLabel 1218 PDFLeslie CitromeNo ratings yet
- DoxepinSleepProductLabel 0310 PDFDocument4 pagesDoxepinSleepProductLabel 0310 PDFLeslie CitromeNo ratings yet
- See Full Prescribing Information For Complete Boxed WarningDocument14 pagesSee Full Prescribing Information For Complete Boxed WarningLeslie CitromeNo ratings yet
- ZolpidemProductLabel 0819 PDFDocument7 pagesZolpidemProductLabel 0819 PDFLeslie CitromeNo ratings yet
- TriazolamProductLabel 1019 PDFDocument13 pagesTriazolamProductLabel 1019 PDFLeslie CitromeNo ratings yet
- DiabetesEpidemiologySlidesForDistribution CITROME AdaptedPsychServ2006Document8 pagesDiabetesEpidemiologySlidesForDistribution CITROME AdaptedPsychServ2006Leslie CitromeNo ratings yet
- Restoril™ (Temazepam) Capsules USP RX Only Warning: Risks From Concomitant Use With OpioidsDocument14 pagesRestoril™ (Temazepam) Capsules USP RX Only Warning: Risks From Concomitant Use With OpioidsLeslie CitromeNo ratings yet
- DoxepinSleepProductLabel 0310 PDFDocument4 pagesDoxepinSleepProductLabel 0310 PDFLeslie CitromeNo ratings yet
- See Full Prescribing Information For Complete Boxed WarningDocument14 pagesSee Full Prescribing Information For Complete Boxed WarningLeslie CitromeNo ratings yet
- TriazolamProductLabel 1019 PDFDocument13 pagesTriazolamProductLabel 1019 PDFLeslie CitromeNo ratings yet
- Benefits of A Second Dose of Intramuscular (IM) Aripiprazole To Control Agitation in Patients With Schizophrenia or Bipolar I DisorderDocument1 pageBenefits of A Second Dose of Intramuscular (IM) Aripiprazole To Control Agitation in Patients With Schizophrenia or Bipolar I DisorderLeslie CitromeNo ratings yet
- ZolpidemProductLabel 0819 PDFDocument7 pagesZolpidemProductLabel 0819 PDFLeslie CitromeNo ratings yet
- WhatIsTranscranialMagneticStimulation CITROME KlineLine1999Document1 pageWhatIsTranscranialMagneticStimulation CITROME KlineLine1999Leslie CitromeNo ratings yet
- INTRODUCTION (Continued)Document1 pageINTRODUCTION (Continued)Leslie CitromeNo ratings yet
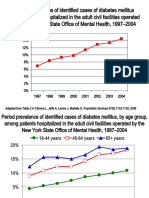
- IncidencePrevalenceSurveillanceDiabetesMellitusInpatientsPoster For Distribution CITROME CINP2006Document1 pageIncidencePrevalenceSurveillanceDiabetesMellitusInpatientsPoster For Distribution CITROME CINP2006Leslie CitromeNo ratings yet
- IncidencePrevalenceSurveillanceDiabetesMellitusInpatientsPoster For Distribution CITROME CINP2006Document1 pageIncidencePrevalenceSurveillanceDiabetesMellitusInpatientsPoster For Distribution CITROME CINP2006Leslie CitromeNo ratings yet
- ZiprasidoneHaloperidolHostilitySchizophreniaPoster CITROME CINP2006Document1 pageZiprasidoneHaloperidolHostilitySchizophreniaPoster CITROME CINP2006Leslie CitromeNo ratings yet
- OlanzapineHighDoseRCTHGLFPoster KINON CINP2006Document19 pagesOlanzapineHighDoseRCTHGLFPoster KINON CINP2006Leslie CitromeNo ratings yet
- DiabetesEpidemiologyFiguresSupplement CITROME PsychServ2006onlineDocument5 pagesDiabetesEpidemiologyFiguresSupplement CITROME PsychServ2006onlineLeslie CitromeNo ratings yet
- Sscchhiizzoopphhrreenniiaa: Ccuurrrreenntt Ttrreeaattm Meenntt CcoonnssiiddeerraattiioonnssDocument4 pagesSscchhiizzoopphhrreenniiaa: Ccuurrrreenntt Ttrreeaattm Meenntt CcoonnssiiddeerraattiioonnssLeslie CitromeNo ratings yet
- ReducingInpatientAggressionPayingAttentionPaysOffPoster NOLAN APA2006Document1 pageReducingInpatientAggressionPayingAttentionPaysOffPoster NOLAN APA2006Leslie CitromeNo ratings yet
- Catechol-O-methyltransferase and Monoamine Oxidase-A Polymorphisms and Treatment Response To Typical and Atypical NeurolepticsDocument3 pagesCatechol-O-methyltransferase and Monoamine Oxidase-A Polymorphisms and Treatment Response To Typical and Atypical NeurolepticsLeslie CitromeNo ratings yet
- CATIENNTEditorialRegardingCITROME KERWIN IntJClinPract2006Document2 pagesCATIENNTEditorialRegardingCITROME KERWIN IntJClinPract2006Leslie CitromeNo ratings yet
- IncidencePrevalenceSurveillanceDiabetesMellitusInpatientsPoster CITROME NCDEU2006Document1 pageIncidencePrevalenceSurveillanceDiabetesMellitusInpatientsPoster CITROME NCDEU2006Leslie CitromeNo ratings yet
- OlanzapineEarlyPredictorsWeightGainBipolarDisorder LIPKOVICH JClinPsychopharm2006Document5 pagesOlanzapineEarlyPredictorsWeightGainBipolarDisorder LIPKOVICH JClinPsychopharm2006Leslie CitromeNo ratings yet
- ZiprasidoneHaloperidolHostilitySchizophreniaPoster CITROME APA2006Document1 pageZiprasidoneHaloperidolHostilitySchizophreniaPoster CITROME APA2006Leslie CitromeNo ratings yet
- MedicalTrainingUnitedStatesAddendum CITROME CMAJ1992Document2 pagesMedicalTrainingUnitedStatesAddendum CITROME CMAJ1992Leslie CitromeNo ratings yet
- QuetiapineAntiaggressiveAgentCaseReport CITROME JCP2001Document1 pageQuetiapineAntiaggressiveAgentCaseReport CITROME JCP2001Leslie CitromeNo ratings yet
- DiabetesSchizophreniaInterview CITROME BehavHealthCare2006Document8 pagesDiabetesSchizophreniaInterview CITROME BehavHealthCare2006Leslie CitromeNo ratings yet
- Chapter 2Document9 pagesChapter 2andro De PioNo ratings yet
- SatvavajayaDocument10 pagesSatvavajayaMatt AldridgeNo ratings yet
- Child PsychiatryDocument320 pagesChild PsychiatryAmalia Ciubotariu100% (1)
- The Care of Aggressive and Antisocial Children and YouthDocument25 pagesThe Care of Aggressive and Antisocial Children and YouthRoch LongueépéeNo ratings yet
- Family Interventions Basic Principles And.8Document9 pagesFamily Interventions Basic Principles And.8Jose Luis AriasNo ratings yet
- 1-S2.0-S1008127520301814-Main 4Document5 pages1-S2.0-S1008127520301814-Main 4afri pakalessyNo ratings yet
- Envy Manifestations and Personality DisordersDocument7 pagesEnvy Manifestations and Personality DisordersDan Rosca100% (1)
- 09: The Nature/Nurture Debate: Student ObjectivesDocument8 pages09: The Nature/Nurture Debate: Student ObjectivesŞterbeţ RuxandraNo ratings yet
- LYRA Value Impact Workforce HealthDocument13 pagesLYRA Value Impact Workforce HealthThomas WhittyNo ratings yet
- Inclusive Final Question BankDocument33 pagesInclusive Final Question BankAsma BadeNo ratings yet
- Psychiatry Is The Branch of Medicine Focused On The DiagnosisDocument3 pagesPsychiatry Is The Branch of Medicine Focused On The DiagnosisTalal MahfouzNo ratings yet
- Parenting Stress in Mothers and Fathers of Toddlers With Autism Spectrum Disorders: Associations With Child CharacteristicsDocument15 pagesParenting Stress in Mothers and Fathers of Toddlers With Autism Spectrum Disorders: Associations With Child CharacteristicsHelena Gandia AbellanNo ratings yet
- Mental IllnessDocument3 pagesMental IllnessKate EvangelistaNo ratings yet
- Health g7 Third QuarterDocument5 pagesHealth g7 Third QuarterSunny Grace Padernal Libo-on100% (2)
- Definitions of Abnormality IntroDocument25 pagesDefinitions of Abnormality IntroamnaNo ratings yet
- Sadness or Depression International Perspectives On The Depression Epidemic and Its Meaning PDFDocument428 pagesSadness or Depression International Perspectives On The Depression Epidemic and Its Meaning PDFAnna MariaNo ratings yet
- DISORDERDocument3 pagesDISORDERMia Grace GarciaNo ratings yet
- Essentials of Abnormal Psychology 8th Edition Durand Test Bank Full Chapter PDFDocument45 pagesEssentials of Abnormal Psychology 8th Edition Durand Test Bank Full Chapter PDFJessicaTorresxokc100% (13)
- 2018-Bell-Abusos en La Infancia y Experiencias Psicóticas en La Edad Adulta-Hallazgos de Un Estudio Longitudinal de 35 AñosDocument6 pages2018-Bell-Abusos en La Infancia y Experiencias Psicóticas en La Edad Adulta-Hallazgos de Un Estudio Longitudinal de 35 Añosmvillar15_247536468No ratings yet
- Paranoid Personality DisorderDocument5 pagesParanoid Personality DisorderKrishia Kamille TanNo ratings yet
- AndenoteDocument8 pagesAndenoteTonetteNo ratings yet
- UPDATED EXAMINATION G7 With ANSWER KEYDocument4 pagesUPDATED EXAMINATION G7 With ANSWER KEYLemuel Español CamusNo ratings yet
- Stage 1: Independence Stage: Family Life Cycle: Issues Influencing Each StageDocument9 pagesStage 1: Independence Stage: Family Life Cycle: Issues Influencing Each StagePaozLyz AND FriendsNo ratings yet
- Individual and Group ChildDocument12 pagesIndividual and Group ChildTabita Raisya RizantiNo ratings yet
- Book of Best Practices Trauma and The Role of Mental Health in Post-Conflict RecoveryDocument383 pagesBook of Best Practices Trauma and The Role of Mental Health in Post-Conflict RecoveryDiego Salcedo AvilaNo ratings yet