You might also like
- Aripiprazol in DeliriumDocument6 pagesAripiprazol in DeliriumRobert MovileanuNo ratings yet
- Safety, Efficacy, and Patient Acceptability of Aripiprazole in The Maintenance Treatment of Bipolar DisorderDocument14 pagesSafety, Efficacy, and Patient Acceptability of Aripiprazole in The Maintenance Treatment of Bipolar DisorderMakkai Popa Mihai VladimirNo ratings yet
- Antipsychotic Treatments For The Elderly Efficacy and Safety of AripiprazoleDocument19 pagesAntipsychotic Treatments For The Elderly Efficacy and Safety of Aripiprazoleneutron mobile gamingNo ratings yet
- Effects of Escitalopram On Plasma Concentrations of Aripiprazole and Its Active Metabolite, Dehydroaripiprazole, in Japanese PatientsDocument5 pagesEffects of Escitalopram On Plasma Concentrations of Aripiprazole and Its Active Metabolite, Dehydroaripiprazole, in Japanese PatientsIulia CiocotisanNo ratings yet
- Leslie Citrome, MD, MPH, Richard Josiassen, PHD, Nigel Bark, MD, Karen S Brown, MS, Suresh Mallikaarjun, PHD, Daniel E Salazar, PHDDocument1 pageLeslie Citrome, MD, MPH, Richard Josiassen, PHD, Nigel Bark, MD, Karen S Brown, MS, Suresh Mallikaarjun, PHD, Daniel E Salazar, PHDLeslie CitromeNo ratings yet
- Nemoto2012 Apz+ Paroxetina RCTDocument5 pagesNemoto2012 Apz+ Paroxetina RCTIulia CiocotisanNo ratings yet
- adverse-events-related-olanzapineDocument4 pagesadverse-events-related-olanzapineDanielNo ratings yet
- Aripiprazole: Formulary ReviewDocument10 pagesAripiprazole: Formulary ReviewmissayayayaNo ratings yet
- Aripiprazole: A Novel Atypical Antipsychotic Drug With A Uniquely Robust PharmacologyDocument20 pagesAripiprazole: A Novel Atypical Antipsychotic Drug With A Uniquely Robust PharmacologyJared Michael BergerNo ratings yet
- Antipsychotic Medication Prescribing Trends in A Tertiary Care HospitalDocument4 pagesAntipsychotic Medication Prescribing Trends in A Tertiary Care HospitalSilfa NataliaNo ratings yet
- Aripiprazol in Delirium La Pacientii VarstniciDocument10 pagesAripiprazol in Delirium La Pacientii VarstniciRobert MovileanuNo ratings yet
- Lithium, Carbamazepine and Valproate in Acute ManiaDocument6 pagesLithium, Carbamazepine and Valproate in Acute ManiaGading AuroraNo ratings yet
- AripripazoleDocument13 pagesAripripazoleOneng IfayaniNo ratings yet
- Darwish2012 Qtp+Armodafinil RCTDocument11 pagesDarwish2012 Qtp+Armodafinil RCTIulia CiocotisanNo ratings yet
- Warnings: Clinical Worsening and Suicide Risk, Precautions: Information For Patients, and Precautions: Pediatric Use)Document19 pagesWarnings: Clinical Worsening and Suicide Risk, Precautions: Information For Patients, and Precautions: Pediatric Use)Zamin AhmedNo ratings yet
- Clotiapine - Another Forgotten Treassure in PsychiatryDocument1 pageClotiapine - Another Forgotten Treassure in PsychiatryJuan IgnacioNo ratings yet
- Rifampin, A Cytochrome P450 3A Inducer, Decreases Plasma Concentrations of Antipsychotic Risperidone in Healthy VolunteersDocument7 pagesRifampin, A Cytochrome P450 3A Inducer, Decreases Plasma Concentrations of Antipsychotic Risperidone in Healthy VolunteersIulia CiocotisanNo ratings yet
- Differences and similarities among the three dopamine receptor partial agonistsDocument10 pagesDifferences and similarities among the three dopamine receptor partial agonistsolivukovic100% (1)
- Atypical Antipsychotics and Newer AntidepressantsDocument21 pagesAtypical Antipsychotics and Newer Antidepressantseagame gamersNo ratings yet
- Population Pharmacokinetics of Valproic Acid in Patients With Mania: Implication For Individualized Dosing RegimensDocument11 pagesPopulation Pharmacokinetics of Valproic Acid in Patients With Mania: Implication For Individualized Dosing RegimensKelletCadilloBarruetoNo ratings yet
- AripiprazoleDocument4 pagesAripiprazolecibad52358No ratings yet
- Kumar 2009Document7 pagesKumar 2009C ONo ratings yet
- Influence of Drugs Interacting With CYP3A4 On The Pharmacokinetics, Pharmacodynamics, and SafetyDocument13 pagesInfluence of Drugs Interacting With CYP3A4 On The Pharmacokinetics, Pharmacodynamics, and SafetyLuciana OliveiraNo ratings yet
- Aripiprazole - Mechanism of Action, Clinical Efficacy and Side EffectsDocument10 pagesAripiprazole - Mechanism of Action, Clinical Efficacy and Side EffectsRuben Del CidNo ratings yet
- Atypical Antipsychotic Augmentation in Major Depressive DisorderDocument13 pagesAtypical Antipsychotic Augmentation in Major Depressive DisorderrantiNo ratings yet
- Brexpiprazole: A Review of A New Treatment Option For Schizophrenia and Major Depressive DisorderDocument6 pagesBrexpiprazole: A Review of A New Treatment Option For Schizophrenia and Major Depressive DisorderLuis Pablo HsNo ratings yet
- Optimal dosing strategies for atypical antipsychoticsDocument6 pagesOptimal dosing strategies for atypical antipsychoticsLeslie CitromeNo ratings yet
- Aripiprazole in Schizophrenia and Schizo PDFDocument18 pagesAripiprazole in Schizophrenia and Schizo PDFAlexandra PopaNo ratings yet
- BurkeDocument10 pagesBurkeMary FallNo ratings yet
- Acute Antipsychotic-Induced Akathisia Revisited - Michael PoyurovskyDocument3 pagesAcute Antipsychotic-Induced Akathisia Revisited - Michael PoyurovskyFábio Yutani KosekiNo ratings yet
- Psychotropic Drugs May Cause High Prolactin LevelsDocument8 pagesPsychotropic Drugs May Cause High Prolactin LevelsAndra SpatarNo ratings yet
- Download Behavioural Neurology Of Anti Epileptic Drugs A Practical Guide Andrea E Cavanna full chapterDocument67 pagesDownload Behavioural Neurology Of Anti Epileptic Drugs A Practical Guide Andrea E Cavanna full chapterronald.allison470100% (5)
- 10.1515 - Jom 1982 821114Document4 pages10.1515 - Jom 1982 821114realxsaloNo ratings yet
- Articles: Spironolactone Management of Resistant HypertensionDocument8 pagesArticles: Spironolactone Management of Resistant HypertensionKatherine America Camac DelgadoNo ratings yet
- Mirelesh Et Al, 1985 - Valproate and Clonazepam Comedication in Epilepsy-EpilepsiaDocument5 pagesMirelesh Et Al, 1985 - Valproate and Clonazepam Comedication in Epilepsy-EpilepsiaFazal DalalNo ratings yet
- Markovitz2002 Risp+Probenecid RCTDocument9 pagesMarkovitz2002 Risp+Probenecid RCTIulia CiocotisanNo ratings yet
- BarbuiDocument8 pagesBarbuirinaldiapt08No ratings yet
- Adjunctive Valproic Acid in Management-Refractory Hyperactive Delirium A Case Series and RationaleDocument6 pagesAdjunctive Valproic Acid in Management-Refractory Hyperactive Delirium A Case Series and RationalefelipeNo ratings yet
- Anti Psychotics Odt'sDocument26 pagesAnti Psychotics Odt'ssaimanideepakNo ratings yet
- Withdrawal Seizure Associated With High Dosage of Aripiprazole and Fluoxetine: A Case ReportDocument3 pagesWithdrawal Seizure Associated With High Dosage of Aripiprazole and Fluoxetine: A Case ReportwsandoNo ratings yet
- Smoking 15Document6 pagesSmoking 15Clara CurcaNo ratings yet
- Refractory Hypotension from Prazosin OverdoseDocument5 pagesRefractory Hypotension from Prazosin OverdoseSyed Shahrul Naz SyedNo ratings yet
- Zyprexa: Olanzapine TabletsDocument32 pagesZyprexa: Olanzapine TabletsnalgatoreNo ratings yet
- Serum Monitoring of Antipsychotic Drug Levels During Concomitant Administration of Sertraline and Antipsychotic MedicationDocument4 pagesSerum Monitoring of Antipsychotic Drug Levels During Concomitant Administration of Sertraline and Antipsychotic MedicationIulia CiocotisanNo ratings yet
- Daftar PustakaDocument16 pagesDaftar PustakaDestrie CindyNo ratings yet
- Revisão AtípicosDocument29 pagesRevisão AtípicosFernanda GuimarãesNo ratings yet
- Mechanism of Action of Antipsychotics: Antipsychotics: Pharmacology and Clinical Decision MakingDocument4 pagesMechanism of Action of Antipsychotics: Antipsychotics: Pharmacology and Clinical Decision MakingLuhur Anggoro SulistioNo ratings yet
- O Carter Snead_2007Document4 pagesO Carter Snead_2007Kossay ZaouiNo ratings yet
- Risperdal Tablets and Solution PiDocument27 pagesRisperdal Tablets and Solution PiIzam M. FalahNo ratings yet
- Aripiprazol in TABDocument10 pagesAripiprazol in TABRobert MovileanuNo ratings yet
- Antipsicoticos 2da Gen 3Document21 pagesAntipsicoticos 2da Gen 3drarodriramosNo ratings yet
- Clozapin RisperidonDocument7 pagesClozapin RisperidonAnonymous 2LcGdsRNo ratings yet
- Coping Therapy Dependence: Naltrexone and Skills For AlcoholDocument7 pagesCoping Therapy Dependence: Naltrexone and Skills For AlcoholOana BumbucNo ratings yet
- Potkin2002 QTP+ Hal Risp Thiridazine RCTDocument10 pagesPotkin2002 QTP+ Hal Risp Thiridazine RCTIulia CiocotisanNo ratings yet
- Jurnal NorvascDocument8 pagesJurnal NorvascYoung AjjaNo ratings yet
- Therapeutic Drug Monitoring of Valproic AcidDocument4 pagesTherapeutic Drug Monitoring of Valproic AcidTanveerNo ratings yet
- Abilify, An Antipsychotic DrugDocument4 pagesAbilify, An Antipsychotic DrugAdam RodriguezNo ratings yet
- The Relationship Between Clinical Pharmacokinetics of Aripiprazole and CYP2D6 Genetic Polymorphism: Effects of CYP Enzyme Inhibition by Coadministration of Paroxetine or FluvoxamineDocument9 pagesThe Relationship Between Clinical Pharmacokinetics of Aripiprazole and CYP2D6 Genetic Polymorphism: Effects of CYP Enzyme Inhibition by Coadministration of Paroxetine or FluvoxamineIulia CiocotisanNo ratings yet
- Ajp 156 5 702Document8 pagesAjp 156 5 7029 PsychologyNo ratings yet
- TriazolamProductLabel 1019 PDFDocument13 pagesTriazolamProductLabel 1019 PDFLeslie CitromeNo ratings yet
- DoxepinSleepProductLabel 0310 PDFDocument4 pagesDoxepinSleepProductLabel 0310 PDFLeslie CitromeNo ratings yet
- ZolpidemProductLabel 0819 PDFDocument7 pagesZolpidemProductLabel 0819 PDFLeslie CitromeNo ratings yet
- See Full Prescribing Information For Complete Boxed WarningDocument14 pagesSee Full Prescribing Information For Complete Boxed WarningLeslie CitromeNo ratings yet
- RamelteonProductLabel 1218 PDFDocument18 pagesRamelteonProductLabel 1218 PDFLeslie CitromeNo ratings yet
- RamelteonProductLabel 1218 PDFDocument18 pagesRamelteonProductLabel 1218 PDFLeslie CitromeNo ratings yet
- ZolpidemProductLabel 0819 PDFDocument7 pagesZolpidemProductLabel 0819 PDFLeslie CitromeNo ratings yet
- TriazolamProductLabel 1019 PDFDocument13 pagesTriazolamProductLabel 1019 PDFLeslie CitromeNo ratings yet
- IncidencePrevalenceSurveillanceDiabetesMellitusInpatientsPoster For Distribution CITROME CINP2006Document1 pageIncidencePrevalenceSurveillanceDiabetesMellitusInpatientsPoster For Distribution CITROME CINP2006Leslie CitromeNo ratings yet
- WhatIsTranscranialMagneticStimulation CITROME KlineLine1999Document1 pageWhatIsTranscranialMagneticStimulation CITROME KlineLine1999Leslie CitromeNo ratings yet
- IncidencePrevalenceSurveillanceDiabetesMellitusInpatientsPoster For Distribution CITROME CINP2006Document1 pageIncidencePrevalenceSurveillanceDiabetesMellitusInpatientsPoster For Distribution CITROME CINP2006Leslie CitromeNo ratings yet
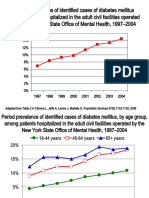
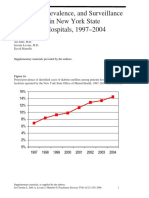
- Diabetes prevalence trends in NY mental hospitalsDocument8 pagesDiabetes prevalence trends in NY mental hospitalsLeslie CitromeNo ratings yet
- DoxepinSleepProductLabel 0310 PDFDocument4 pagesDoxepinSleepProductLabel 0310 PDFLeslie CitromeNo ratings yet
- Restoril™ (Temazepam) Capsules USP RX Only Warning: Risks From Concomitant Use With OpioidsDocument14 pagesRestoril™ (Temazepam) Capsules USP RX Only Warning: Risks From Concomitant Use With OpioidsLeslie CitromeNo ratings yet
- Ziprasidone efficacy against hostility in schizophreniaDocument1 pageZiprasidone efficacy against hostility in schizophreniaLeslie CitromeNo ratings yet
- CATIENNTEditorialRegardingCITROME KERWIN IntJClinPract2006Document2 pagesCATIENNTEditorialRegardingCITROME KERWIN IntJClinPract2006Leslie CitromeNo ratings yet
- See Full Prescribing Information For Complete Boxed WarningDocument14 pagesSee Full Prescribing Information For Complete Boxed WarningLeslie CitromeNo ratings yet
- OlanzapineHighDoseRCTHGLFPoster KINON CINP2006Document19 pagesOlanzapineHighDoseRCTHGLFPoster KINON CINP2006Leslie CitromeNo ratings yet
- INTRODUCTION (Continued)Document1 pageINTRODUCTION (Continued)Leslie CitromeNo ratings yet
- Incidence and Prevalence of Diabetes in NY Psychiatric Hospitals 1997-2004Document5 pagesIncidence and Prevalence of Diabetes in NY Psychiatric Hospitals 1997-2004Leslie CitromeNo ratings yet
- IncidencePrevalenceSurveillanceDiabetesMellitusInpatientsPoster CITROME NCDEU2006Document1 pageIncidencePrevalenceSurveillanceDiabetesMellitusInpatientsPoster CITROME NCDEU2006Leslie CitromeNo ratings yet
- Sscchhiizzoopphhrreenniiaa: Ccuurrrreenntt Ttrreeaattm Meenntt CcoonnssiiddeerraattiioonnssDocument4 pagesSscchhiizzoopphhrreenniiaa: Ccuurrrreenntt Ttrreeaattm Meenntt CcoonnssiiddeerraattiioonnssLeslie CitromeNo ratings yet
- Benefits of A Second Dose of Intramuscular (IM) Aripiprazole To Control Agitation in Patients With Schizophrenia or Bipolar I DisorderDocument1 pageBenefits of A Second Dose of Intramuscular (IM) Aripiprazole To Control Agitation in Patients With Schizophrenia or Bipolar I DisorderLeslie CitromeNo ratings yet
- NR330 Efficacy of Ziprasidone Against Hostility in SchizophreniaDocument1 pageNR330 Efficacy of Ziprasidone Against Hostility in SchizophreniaLeslie CitromeNo ratings yet
- OlanzapineEarlyPredictorsWeightGainBipolarDisorder LIPKOVICH JClinPsychopharm2006Document5 pagesOlanzapineEarlyPredictorsWeightGainBipolarDisorder LIPKOVICH JClinPsychopharm2006Leslie CitromeNo ratings yet
- Catechol-O-methyltransferase and Monoamine Oxidase-A Polymorphisms and Treatment Response To Typical and Atypical NeurolepticsDocument3 pagesCatechol-O-methyltransferase and Monoamine Oxidase-A Polymorphisms and Treatment Response To Typical and Atypical NeurolepticsLeslie CitromeNo ratings yet
- ReducingInpatientAggressionPayingAttentionPaysOffPoster NOLAN APA2006Document1 pageReducingInpatientAggressionPayingAttentionPaysOffPoster NOLAN APA2006Leslie CitromeNo ratings yet
- QuetiapineAntiaggressiveAgentCaseReport CITROME JCP2001Document1 pageQuetiapineAntiaggressiveAgentCaseReport CITROME JCP2001Leslie CitromeNo ratings yet
- ZiprasidoneHaloperidolHostilitySchizophrenia CITROME JCP2006 PDFDocument5 pagesZiprasidoneHaloperidolHostilitySchizophrenia CITROME JCP2006 PDFLeslie CitromeNo ratings yet
- DiabetesSchizophreniaInterview CITROME BehavHealthCare2006Document8 pagesDiabetesSchizophreniaInterview CITROME BehavHealthCare2006Leslie CitromeNo ratings yet
- Antidotes and Their UsesDocument3 pagesAntidotes and Their UsesAbdul SalamNo ratings yet
- Nephrotoxic Drugs - Ready ReckonersDocument14 pagesNephrotoxic Drugs - Ready ReckonerskrgduraiNo ratings yet
- TB DB FinalDocument92 pagesTB DB FinalAbdullah Khairul AfnanNo ratings yet
- Side Effects of Expare.Document6 pagesSide Effects of Expare.Emelda LaraNo ratings yet
- Nexpro Uae FinalDocument13 pagesNexpro Uae Finalamr ahmedNo ratings yet
- Drug Study: La Salle UniversityDocument3 pagesDrug Study: La Salle UniversityJb RosillosaNo ratings yet
- Daftar Formularium ObatDocument6 pagesDaftar Formularium ObatRina HerlinaNo ratings yet
- Antibiotic Skin TestingDocument8 pagesAntibiotic Skin TestingFitz JaminitNo ratings yet
- Anticancer ChemotherapyDocument40 pagesAnticancer Chemotherapyanon_3901479100% (1)
- Certificate For COVID-19 Vaccination: Beneficiary DetailsDocument1 pageCertificate For COVID-19 Vaccination: Beneficiary DetailsS M SarojNo ratings yet
- Saldo Per Barang: Nama Barang Kode Barangbatch No. Exp. Datesaldo Batch Otal BarangDocument34 pagesSaldo Per Barang: Nama Barang Kode Barangbatch No. Exp. Datesaldo Batch Otal BarangimansariNo ratings yet
- Contoh Gol. Obat KIEDocument5 pagesContoh Gol. Obat KIEYanuar prasetyoNo ratings yet
- CetirizineDocument2 pagesCetirizineAnonymous QqyLDoW1No ratings yet
- How To Administer Intramuscular (IM) Vaccines: Client Age Injection Site Needle SizeDocument2 pagesHow To Administer Intramuscular (IM) Vaccines: Client Age Injection Site Needle Sizeemilia_sweetyNo ratings yet
- Certificate For COVID-19 Vaccination: Beneficiary DetailsDocument1 pageCertificate For COVID-19 Vaccination: Beneficiary DetailsaravindNo ratings yet
- SDFO Drug Education Module, T1 AY 2018-2019Document65 pagesSDFO Drug Education Module, T1 AY 2018-2019Cheryle gayodanNo ratings yet
- Stok Opname Ok Feb 2021Document14 pagesStok Opname Ok Feb 2021fiannysjahjadiNo ratings yet
- Effectiveness of Clomiphene Citrate For Improving Sperm ConcentrationDocument6 pagesEffectiveness of Clomiphene Citrate For Improving Sperm ConcentrationRoy LiemNo ratings yet
- PainDocument90 pagesPainmikErlh100% (4)
- Name of The Medicinal ProductDocument7 pagesName of The Medicinal Productddandan_2No ratings yet
- Tech Sheet - Desvac Dovac - ENDocument2 pagesTech Sheet - Desvac Dovac - ENNaeem AhmadNo ratings yet
- Case Presentation: Presented By: Gokul. A. J 2 Pharm. D (17Q3009)Document22 pagesCase Presentation: Presented By: Gokul. A. J 2 Pharm. D (17Q3009)GimpNo ratings yet
- CBR A Drug DevelopDocument2 pagesCBR A Drug DevelopAlfieNo ratings yet
- DRUG-EDUCATION-FOR-THE-YOUTH-NSTP-LECTURE (1) .OdpDocument70 pagesDRUG-EDUCATION-FOR-THE-YOUTH-NSTP-LECTURE (1) .OdpJulia Shane BarriosNo ratings yet
- Recording Forms (Masterlist) School Forms - Kinder To Grade 7Document16 pagesRecording Forms (Masterlist) School Forms - Kinder To Grade 7lourdes estopaciaNo ratings yet
- Cefazolin and Dextrose USP for bacterial infectionsDocument3 pagesCefazolin and Dextrose USP for bacterial infectionsYaleswari Hayu PertiwiNo ratings yet
- Drug InteractionsDocument43 pagesDrug Interactionstry_dinaa100% (1)
- Pharmacokinetic and Pharmacodynamic Properties of Histamine H Receptor AntagonistsDocument19 pagesPharmacokinetic and Pharmacodynamic Properties of Histamine H Receptor AntagonistsSasoo EmadNo ratings yet
- PentoxifyllineDocument7 pagesPentoxifyllinePapaindoNo ratings yet
- فارما تلخيصDocument8 pagesفارما تلخيصmahmoud fuqahaNo ratings yet