You might also like
- Metabolic Syndrome Program: How to Lose Weight, Beat Heart Disease, Stop Insulin Resistance and MoreFrom EverandMetabolic Syndrome Program: How to Lose Weight, Beat Heart Disease, Stop Insulin Resistance and MoreRating: 4.5 out of 5 stars4.5/5 (2)
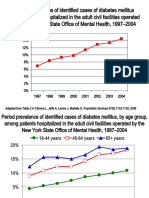
- Diabetes and Schizophrenia 2005: Are We Any Closer To Understanding The Link?Document10 pagesDiabetes and Schizophrenia 2005: Are We Any Closer To Understanding The Link?Leslie CitromeNo ratings yet
- Metabolic Syndrome and Psychiatric Illness: Interactions, Pathophysiology, Assessment and TreatmentFrom EverandMetabolic Syndrome and Psychiatric Illness: Interactions, Pathophysiology, Assessment and TreatmentNo ratings yet
- The Metabolic Syndrome - What Is It and How Should It Be Managed?Document14 pagesThe Metabolic Syndrome - What Is It and How Should It Be Managed?adi suputraNo ratings yet
- The Metabolic Syndrome: Time For A Critical AppraisalDocument16 pagesThe Metabolic Syndrome: Time For A Critical AppraisalprabhatguyNo ratings yet
- A Comprehensive Definition For Metabolic Syndrome - PMCDocument13 pagesA Comprehensive Definition For Metabolic Syndrome - PMCGAYATHIRINo ratings yet
- Mottillo2010 PDFDocument20 pagesMottillo2010 PDFSintia CahyaniNo ratings yet
- Sindrome Metabolico Med - Clin - North - Am 2011Document19 pagesSindrome Metabolico Med - Clin - North - Am 2011saraNo ratings yet
- Metabolic Syndrome as a Predictor of DiabetesDocument10 pagesMetabolic Syndrome as a Predictor of DiabetesChiranjeeviNo ratings yet
- The metabolic syndrome: understanding a global epidemicDocument14 pagesThe metabolic syndrome: understanding a global epidemicPaulo Victor Amorim MarquesNo ratings yet
- Metabolicsyndrome: Susan L. Samson,, Alan J. GarberDocument23 pagesMetabolicsyndrome: Susan L. Samson,, Alan J. GarberStephany ArenasNo ratings yet
- Metabolicsyndrome: Susan L. Samson,, Alan J. GarberDocument16 pagesMetabolicsyndrome: Susan L. Samson,, Alan J. GarberCarla ValladoNo ratings yet
- Metabolic Syndrome and StrokeDocument5 pagesMetabolic Syndrome and StrokeEmir SaricNo ratings yet
- Journal of Diabetes and Its ComplicationsDocument5 pagesJournal of Diabetes and Its ComplicationsQqNo ratings yet
- Metabolic Syndrome May Be A Sign of Rapid Aging 2155 6156 1000674Document5 pagesMetabolic Syndrome May Be A Sign of Rapid Aging 2155 6156 1000674Kiki KikukNo ratings yet
- ObesityDocument33 pagesObesitySusy QuirozNo ratings yet
- The Metabolic Syndrome Prevalence, CHD Risk, and Treatment: Cinzia Sarti T, John GallagherDocument12 pagesThe Metabolic Syndrome Prevalence, CHD Risk, and Treatment: Cinzia Sarti T, John GallagherMatthew ContrerasNo ratings yet
- 2005 - M BERTOLOTTI - Reviewarticlehyperlipidaemiaandcardiovascularrisk (Retrieved-2016!08!22)Document3 pages2005 - M BERTOLOTTI - Reviewarticlehyperlipidaemiaandcardiovascularrisk (Retrieved-2016!08!22)jeffaguilarNo ratings yet
- Cardiovascular Disease in Diabetes, Beyond GlucoseDocument27 pagesCardiovascular Disease in Diabetes, Beyond GlucosemagreaNo ratings yet
- Supersize Teens - The Metabolic Syndrome.Document23 pagesSupersize Teens - The Metabolic Syndrome.Milon MitraNo ratings yet
- The Metabolic Syndrome-From Insulin Resistance To Obesity and DiabetesDocument19 pagesThe Metabolic Syndrome-From Insulin Resistance To Obesity and DiabetesLucho FerroNo ratings yet
- Metabolic Syndrome: Misleading Diagnosis or Valid Condition?Document3 pagesMetabolic Syndrome: Misleading Diagnosis or Valid Condition?melaniratihNo ratings yet
- Metabolic Syndrome (Insulin Resistance Syndrome or Syndrome X) - UpToDateDocument17 pagesMetabolic Syndrome (Insulin Resistance Syndrome or Syndrome X) - UpToDateAlejandro Flores VelascoNo ratings yet
- Jbcahs 4 39Document7 pagesJbcahs 4 39miranddaelvira02No ratings yet
- AnnotationsDocument3 pagesAnnotationsAegina FestinNo ratings yet
- Metabolic SyndromeDocument9 pagesMetabolic SyndromeThomasManuelWasuwayNo ratings yet
- Cardiometabolic Syndrome PipinDocument15 pagesCardiometabolic Syndrome Pipinspider_mechNo ratings yet
- Dyson LineDocument10 pagesDyson LineSharly DwijayantiNo ratings yet
- Am J Clin Nutr 2006 Reaven 1237-47-1Document12 pagesAm J Clin Nutr 2006 Reaven 1237-47-1mrclpppNo ratings yet
- Metabolic Syndrome: Learning ObjectivesDocument20 pagesMetabolic Syndrome: Learning Objectivesddeeb420% (1)
- ++balkau 1999Document3 pages++balkau 1999Nodira AlakbarovaNo ratings yet
- Harmonizing The Metabolic SyndromeDocument7 pagesHarmonizing The Metabolic SyndromeCarlos_RuedasNo ratings yet
- 2018 Dislipidemia-RevisaDocument16 pages2018 Dislipidemia-RevisaLuminita HutanuNo ratings yet
- Srikant H 2016Document10 pagesSrikant H 2016aditya sekarNo ratings yet
- Dislipidemia ACP 2017Document16 pagesDislipidemia ACP 2017José Luis PradoNo ratings yet
- The Metabolic Syndrome: T. Fulop, D. Tessier, A. CarpentierDocument12 pagesThe Metabolic Syndrome: T. Fulop, D. Tessier, A. CarpentierLaviniaMenicucciNo ratings yet
- Approach To DyslipedimiaDocument26 pagesApproach To Dyslipedimiaazharuddin imamuddinNo ratings yet
- 2007 Metabolic Sindrom CVDDocument8 pages2007 Metabolic Sindrom CVDLuminita HutanuNo ratings yet
- Alencar 2010Document6 pagesAlencar 2010Tín NguyễnNo ratings yet
- Lien 2008Document14 pagesLien 2008gyyygNo ratings yet
- Cardiovascular Safety Profile of Currently Available Diabetic DrugsDocument17 pagesCardiovascular Safety Profile of Currently Available Diabetic Drugsvina_nursyaidahNo ratings yet
- Assessing cardiovascular risk in diabetics using different indicesDocument5 pagesAssessing cardiovascular risk in diabetics using different indicesSeptian PutraNo ratings yet
- Artículo Dislipemia ESCDocument12 pagesArtículo Dislipemia ESCSMIBA MedicinaNo ratings yet
- 2004 Metabolic Risk During Antipsychotic TreatmentDocument11 pages2004 Metabolic Risk During Antipsychotic TreatmentDiego HormacheaNo ratings yet
- Diabetes Treatment Literature ReviewDocument7 pagesDiabetes Treatment Literature Reviewafmzatvuipwdal100% (1)
- Atherogenic Dyslipidemia in Patients With Established Coronary Artery DiseaseDocument6 pagesAtherogenic Dyslipidemia in Patients With Established Coronary Artery DiseasebilahalvirayuNo ratings yet
- 2 Metabolic - Syndrom - Sherling DHDocument3 pages2 Metabolic - Syndrom - Sherling DHM JNo ratings yet
- Polygenic Hypercholesterolemia: Causes, Risks & TreatmentDocument6 pagesPolygenic Hypercholesterolemia: Causes, Risks & TreatmentSamhitha Ayurvedic ChennaiNo ratings yet
- Sdarticle1 La HoreDocument20 pagesSdarticle1 La HoreLuis Eduardo SantosNo ratings yet
- Polypharmacy in The Aging Patient A Review of Glycemic Control in Older Adults With Type 2 DiabetesDocument12 pagesPolypharmacy in The Aging Patient A Review of Glycemic Control in Older Adults With Type 2 Diabetesapi-311409998No ratings yet
- Wa0003.Document14 pagesWa0003.MariaVirginiaNo ratings yet
- Association of Hypertriglyceridemia With Ischemic Stroke, Study in A Tertiary Care Hospital in BangladeshDocument6 pagesAssociation of Hypertriglyceridemia With Ischemic Stroke, Study in A Tertiary Care Hospital in BangladeshRay HannaNo ratings yet
- Hyperglycemic CrisisDocument9 pagesHyperglycemic CrisisRoberto López MataNo ratings yet
- Diabetes 5Document16 pagesDiabetes 5patricia osei-owusuNo ratings yet
- Crawford Nutri Sas 21Document7 pagesCrawford Nutri Sas 21Divo Skye CrawfordNo ratings yet
- The Effects of Menopause On The Serum Lipid Profile of Normal Females of South East Nigeria J. C. Igweh, I. U. Nwagha, J. M. OkaroDocument6 pagesThe Effects of Menopause On The Serum Lipid Profile of Normal Females of South East Nigeria J. C. Igweh, I. U. Nwagha, J. M. OkaroutarinuNo ratings yet
- j.1365 2796.2006.01752.x20160829 29101 n3bfks With Cover Page v2Document12 pagesj.1365 2796.2006.01752.x20160829 29101 n3bfks With Cover Page v2herondaleNo ratings yet
- A Comprehensive Definition For Metabolic Syndrome: Paul L. HuangDocument7 pagesA Comprehensive Definition For Metabolic Syndrome: Paul L. HuangFedrik Monte Kristo LimbongNo ratings yet
- PCSK9 INHIBITORS FOR DYSLIPIDEMIA CONTROLDocument10 pagesPCSK9 INHIBITORS FOR DYSLIPIDEMIA CONTROLAlexander JosethangNo ratings yet
- Jhs v3 Id1044 PDFDocument4 pagesJhs v3 Id1044 PDFUrsheila HaekmatiarNo ratings yet
- See Full Prescribing Information For Complete Boxed WarningDocument14 pagesSee Full Prescribing Information For Complete Boxed WarningLeslie CitromeNo ratings yet
- RamelteonProductLabel 1218 PDFDocument18 pagesRamelteonProductLabel 1218 PDFLeslie CitromeNo ratings yet
- TriazolamProductLabel 1019 PDFDocument13 pagesTriazolamProductLabel 1019 PDFLeslie CitromeNo ratings yet
- Restoril™ (Temazepam) Capsules USP RX Only Warning: Risks From Concomitant Use With OpioidsDocument14 pagesRestoril™ (Temazepam) Capsules USP RX Only Warning: Risks From Concomitant Use With OpioidsLeslie CitromeNo ratings yet
- ZolpidemProductLabel 0819 PDFDocument7 pagesZolpidemProductLabel 0819 PDFLeslie CitromeNo ratings yet
- See Full Prescribing Information For Complete Boxed WarningDocument14 pagesSee Full Prescribing Information For Complete Boxed WarningLeslie CitromeNo ratings yet
- ZolpidemProductLabel 0819 PDFDocument7 pagesZolpidemProductLabel 0819 PDFLeslie CitromeNo ratings yet
- DoxepinSleepProductLabel 0310 PDFDocument4 pagesDoxepinSleepProductLabel 0310 PDFLeslie CitromeNo ratings yet
- WhatIsTranscranialMagneticStimulation CITROME KlineLine1999Document1 pageWhatIsTranscranialMagneticStimulation CITROME KlineLine1999Leslie CitromeNo ratings yet
- RamelteonProductLabel 1218 PDFDocument18 pagesRamelteonProductLabel 1218 PDFLeslie CitromeNo ratings yet
- TriazolamProductLabel 1019 PDFDocument13 pagesTriazolamProductLabel 1019 PDFLeslie CitromeNo ratings yet
- Sscchhiizzoopphhrreenniiaa: Ccuurrrreenntt Ttrreeaattm Meenntt CcoonnssiiddeerraattiioonnssDocument4 pagesSscchhiizzoopphhrreenniiaa: Ccuurrrreenntt Ttrreeaattm Meenntt CcoonnssiiddeerraattiioonnssLeslie CitromeNo ratings yet
- Diabetes prevalence trends in NY mental hospitalsDocument8 pagesDiabetes prevalence trends in NY mental hospitalsLeslie CitromeNo ratings yet
- DoxepinSleepProductLabel 0310 PDFDocument4 pagesDoxepinSleepProductLabel 0310 PDFLeslie CitromeNo ratings yet
- IncidencePrevalenceSurveillanceDiabetesMellitusInpatientsPoster For Distribution CITROME CINP2006Document1 pageIncidencePrevalenceSurveillanceDiabetesMellitusInpatientsPoster For Distribution CITROME CINP2006Leslie CitromeNo ratings yet
- CATIENNTEditorialRegardingCITROME KERWIN IntJClinPract2006Document2 pagesCATIENNTEditorialRegardingCITROME KERWIN IntJClinPract2006Leslie CitromeNo ratings yet
- IncidencePrevalenceSurveillanceDiabetesMellitusInpatientsPoster For Distribution CITROME CINP2006Document1 pageIncidencePrevalenceSurveillanceDiabetesMellitusInpatientsPoster For Distribution CITROME CINP2006Leslie CitromeNo ratings yet
- INTRODUCTION (Continued)Document1 pageINTRODUCTION (Continued)Leslie CitromeNo ratings yet
- Ziprasidone efficacy against hostility in schizophreniaDocument1 pageZiprasidone efficacy against hostility in schizophreniaLeslie CitromeNo ratings yet
- OlanzapineHighDoseRCTHGLFPoster KINON CINP2006Document19 pagesOlanzapineHighDoseRCTHGLFPoster KINON CINP2006Leslie CitromeNo ratings yet
- OlanzapineEarlyPredictorsWeightGainBipolarDisorder LIPKOVICH JClinPsychopharm2006Document5 pagesOlanzapineEarlyPredictorsWeightGainBipolarDisorder LIPKOVICH JClinPsychopharm2006Leslie CitromeNo ratings yet
- Catechol-O-methyltransferase and Monoamine Oxidase-A Polymorphisms and Treatment Response To Typical and Atypical NeurolepticsDocument3 pagesCatechol-O-methyltransferase and Monoamine Oxidase-A Polymorphisms and Treatment Response To Typical and Atypical NeurolepticsLeslie CitromeNo ratings yet
- IncidencePrevalenceSurveillanceDiabetesMellitusInpatientsPoster CITROME NCDEU2006Document1 pageIncidencePrevalenceSurveillanceDiabetesMellitusInpatientsPoster CITROME NCDEU2006Leslie CitromeNo ratings yet
- Incidence and Prevalence of Diabetes in NY Psychiatric Hospitals 1997-2004Document5 pagesIncidence and Prevalence of Diabetes in NY Psychiatric Hospitals 1997-2004Leslie CitromeNo ratings yet
- ReducingInpatientAggressionPayingAttentionPaysOffPoster NOLAN APA2006Document1 pageReducingInpatientAggressionPayingAttentionPaysOffPoster NOLAN APA2006Leslie CitromeNo ratings yet
- NR330 Efficacy of Ziprasidone Against Hostility in SchizophreniaDocument1 pageNR330 Efficacy of Ziprasidone Against Hostility in SchizophreniaLeslie CitromeNo ratings yet
- DiabetesSchizophreniaInterview CITROME BehavHealthCare2006Document8 pagesDiabetesSchizophreniaInterview CITROME BehavHealthCare2006Leslie CitromeNo ratings yet
- MedicalTrainingUnitedStatesAddendum CITROME CMAJ1992Document2 pagesMedicalTrainingUnitedStatesAddendum CITROME CMAJ1992Leslie CitromeNo ratings yet
- Benefits of A Second Dose of Intramuscular (IM) Aripiprazole To Control Agitation in Patients With Schizophrenia or Bipolar I DisorderDocument1 pageBenefits of A Second Dose of Intramuscular (IM) Aripiprazole To Control Agitation in Patients With Schizophrenia or Bipolar I DisorderLeslie CitromeNo ratings yet
- QuetiapineAntiaggressiveAgentCaseReport CITROME JCP2001Document1 pageQuetiapineAntiaggressiveAgentCaseReport CITROME JCP2001Leslie CitromeNo ratings yet
- St. Paul University Philippines: School of Health SciencesDocument8 pagesSt. Paul University Philippines: School of Health SciencesJay Andrea Vea IsraelNo ratings yet
- Post Analytical Best PracticesDocument61 pagesPost Analytical Best PracticesSaravnan Rajendran100% (1)
- What is cholesterol and its functions in the bodyDocument5 pagesWhat is cholesterol and its functions in the bodySara SirajNo ratings yet
- Lipids Case StudiesDocument6 pagesLipids Case Studiesgogo29% (7)
- Quicknotes MedsurgDocument638 pagesQuicknotes MedsurgGVHH100% (17)
- NiaCur (With Monolaurin + Cofactors) Protocol - Jan 6, 2022Document27 pagesNiaCur (With Monolaurin + Cofactors) Protocol - Jan 6, 2022Humberto Alfaro IbarraNo ratings yet
- HtyhDocument324 pagesHtyhmike jognNo ratings yet
- ACE Personal Trainer Manual Chapter 13Document59 pagesACE Personal Trainer Manual Chapter 13Đạt NguyễnNo ratings yet
- Standard Qualification FormDocument2 pagesStandard Qualification Formjonam7102No ratings yet
- Blood Sugar Lowering Effect of Zinc and Multi Vitamin/ Mineral Supplementation Is Dependent On Initial Fasting Blood GlucoseDocument14 pagesBlood Sugar Lowering Effect of Zinc and Multi Vitamin/ Mineral Supplementation Is Dependent On Initial Fasting Blood GlucoseNorries Jonell CaballarNo ratings yet
- 10 1056@NEJMoa1803917 PDFDocument11 pages10 1056@NEJMoa1803917 PDFRiler ChtoNo ratings yet
- Functional Foods FOR KIDNEY DISEASESDocument29 pagesFunctional Foods FOR KIDNEY DISEASESBliss CloudNo ratings yet
- Diagnostic Biochemistry. (Ms 1st &2nd Sem.3rd Year) Part-3newDocument94 pagesDiagnostic Biochemistry. (Ms 1st &2nd Sem.3rd Year) Part-3newmatrix_oriNo ratings yet
- Diabetes Mellitus Complte LONG 2Document56 pagesDiabetes Mellitus Complte LONG 2John Vincent Dy OcampoNo ratings yet
- GLUCOSE, UREA, URIC ACID, CREATININE, CHOLESTEROL, TRIGLYCERIDE, HDL-C, LDL-C, TOTAL PROTEIN, ALBUMIN, BILIRUBIN TEST METHODSDocument4 pagesGLUCOSE, UREA, URIC ACID, CREATININE, CHOLESTEROL, TRIGLYCERIDE, HDL-C, LDL-C, TOTAL PROTEIN, ALBUMIN, BILIRUBIN TEST METHODSZoe Tagoc100% (3)
- 4-HLS SLIDE, SplinaDocument153 pages4-HLS SLIDE, Splinaapi-3804539No ratings yet
- Acute Ischemic Stroke Management: Dr. Aldrin C Leman, SpsDocument25 pagesAcute Ischemic Stroke Management: Dr. Aldrin C Leman, SpsRizky MaulydaNo ratings yet
- Study of Lipid Profile in Coronary Heart Disease Patients in LibyaDocument9 pagesStudy of Lipid Profile in Coronary Heart Disease Patients in LibyaInternational Medical PublisherNo ratings yet
- High-Intensity Statin Therapy Yields Better OutcomDocument14 pagesHigh-Intensity Statin Therapy Yields Better Outcomkehie HananielNo ratings yet
- Green Tea Health BenefitsDocument13 pagesGreen Tea Health BenefitsStreetreach CameroonNo ratings yet
- HypertriglyceridemiaDocument8 pagesHypertriglyceridemiaNaila KhanNo ratings yet
- Extracting Carotenoid Pigments from Citrus Peel and Studying Their Functional PropertiesDocument18 pagesExtracting Carotenoid Pigments from Citrus Peel and Studying Their Functional Propertiesmerah hadjerNo ratings yet
- Spesial Untuk Member Baru: Body Fat CalculatorDocument1 pageSpesial Untuk Member Baru: Body Fat CalculatorSiska Syadiatul ZanahNo ratings yet
- Is Darkfield Microscopic Examination of Fresh Capillary Blood A VDocument137 pagesIs Darkfield Microscopic Examination of Fresh Capillary Blood A Vwtemple100% (3)
- Hyperlipidemia Guide: Causes, Symptoms and TreatmentDocument17 pagesHyperlipidemia Guide: Causes, Symptoms and Treatmentbent alfay7a2No ratings yet
- The Stubborn Fat SolutionDocument50 pagesThe Stubborn Fat SolutionMohamed Elkhder100% (2)
- 7509 17831 1 PB PDFDocument8 pages7509 17831 1 PB PDFMudhiatul 'AilahNo ratings yet
- Fermented Milk Products May Improve HealthDocument7 pagesFermented Milk Products May Improve Healthmilu1312No ratings yet
- 2001 AnnualDocument78 pages2001 Annualrizaldi rahmatullahNo ratings yet
- How Hyperlipidemia in Children Impacts Thrombosis and AtherosclerosisDocument10 pagesHow Hyperlipidemia in Children Impacts Thrombosis and AtherosclerosisFitriyana WinarnoNo ratings yet
- Boundless: Upgrade Your Brain, Optimize Your Body & Defy AgingFrom EverandBoundless: Upgrade Your Brain, Optimize Your Body & Defy AgingRating: 4.5 out of 5 stars4.5/5 (66)
- Chair Yoga: Sit, Stretch, and Strengthen Your Way to a Happier, Healthier YouFrom EverandChair Yoga: Sit, Stretch, and Strengthen Your Way to a Happier, Healthier YouRating: 3.5 out of 5 stars3.5/5 (5)
- Whole Body Barefoot: Transitioning Well to Minimal FootwearFrom EverandWhole Body Barefoot: Transitioning Well to Minimal FootwearRating: 4 out of 5 stars4/5 (16)
- Power of 10: The Once-A-Week Slow Motion Fitness RevolutionFrom EverandPower of 10: The Once-A-Week Slow Motion Fitness RevolutionRating: 3.5 out of 5 stars3.5/5 (11)
- Body by Science: A Research Based Program for Strength Training, Body building, and Complete Fitness in 12 Minutes a WeekFrom EverandBody by Science: A Research Based Program for Strength Training, Body building, and Complete Fitness in 12 Minutes a WeekRating: 4.5 out of 5 stars4.5/5 (84)
- Functional Training and Beyond: Building the Ultimate Superfunctional Body and MindFrom EverandFunctional Training and Beyond: Building the Ultimate Superfunctional Body and MindRating: 4.5 out of 5 stars4.5/5 (1)
- Aging Backwards: Reverse the Aging Process and Look 10 Years Younger in 30 Minutes a DayFrom EverandAging Backwards: Reverse the Aging Process and Look 10 Years Younger in 30 Minutes a DayNo ratings yet
- Peak: The New Science of Athletic Performance That is Revolutionizing SportsFrom EverandPeak: The New Science of Athletic Performance That is Revolutionizing SportsRating: 5 out of 5 stars5/5 (95)
- The Yamas & Niyamas: Exploring Yoga's Ethical PracticeFrom EverandThe Yamas & Niyamas: Exploring Yoga's Ethical PracticeRating: 4.5 out of 5 stars4.5/5 (19)
- Muscle for Life: Get Lean, Strong, and Healthy at Any Age!From EverandMuscle for Life: Get Lean, Strong, and Healthy at Any Age!Rating: 4.5 out of 5 stars4.5/5 (22)
- Relentless: From Good to Great to UnstoppableFrom EverandRelentless: From Good to Great to UnstoppableRating: 5 out of 5 stars5/5 (782)
- Strong Is the New Beautiful: Embrace Your Natural Beauty, Eat Clean, and Harness Your PowerFrom EverandStrong Is the New Beautiful: Embrace Your Natural Beauty, Eat Clean, and Harness Your PowerRating: 4 out of 5 stars4/5 (5)
- Weight Lifting Is a Waste of Time: So Is Cardio, and There’s a Better Way to Have the Body You WantFrom EverandWeight Lifting Is a Waste of Time: So Is Cardio, and There’s a Better Way to Have the Body You WantRating: 4.5 out of 5 stars4.5/5 (38)
- Endure: Mind, Body, and the Curiously Elastic Limits of Human PerformanceFrom EverandEndure: Mind, Body, and the Curiously Elastic Limits of Human PerformanceRating: 4.5 out of 5 stars4.5/5 (237)
- 7 Weeks to 10 Pounds of Muscle: The Complete Day-by-Day Program to Pack on Lean, Healthy Muscle MassFrom Everand7 Weeks to 10 Pounds of Muscle: The Complete Day-by-Day Program to Pack on Lean, Healthy Muscle MassRating: 4 out of 5 stars4/5 (2)
- Yamas & Niyamas: Exploring Yoga's Ethical PracticeFrom EverandYamas & Niyamas: Exploring Yoga's Ethical PracticeRating: 4.5 out of 5 stars4.5/5 (110)
- The Yogi Code: Seven Universal Laws of Infinite SuccessFrom EverandThe Yogi Code: Seven Universal Laws of Infinite SuccessRating: 4.5 out of 5 stars4.5/5 (104)
- Roxane Gay & Everand Originals: Built for This: The Quiet Strength of PowerliftingFrom EverandRoxane Gay & Everand Originals: Built for This: The Quiet Strength of PowerliftingRating: 4.5 out of 5 stars4.5/5 (132)
- Applied Polyvagal Theory in Yoga: Therapeutic Practices for Emotional HealthFrom EverandApplied Polyvagal Theory in Yoga: Therapeutic Practices for Emotional HealthNo ratings yet
- Music For Healing: With Nature Sounds For Natural Healing Powers: Sounds Of Nature, Deep Sleep Music, Meditation, Relaxation, Healing MusicFrom EverandMusic For Healing: With Nature Sounds For Natural Healing Powers: Sounds Of Nature, Deep Sleep Music, Meditation, Relaxation, Healing MusicRating: 5 out of 5 stars5/5 (1)
- Body by Science: A Research Based Program to Get the Results You Want in 12 Minutes a WeekFrom EverandBody by Science: A Research Based Program to Get the Results You Want in 12 Minutes a WeekRating: 4 out of 5 stars4/5 (38)
- The Calisthenics Codex: Fifty Exercises for Functional FitnessFrom EverandThe Calisthenics Codex: Fifty Exercises for Functional FitnessRating: 4 out of 5 stars4/5 (9)
- Calisthenics: Guide for Bodyweight Exercise, Build your Dream Body in 30 MinutesFrom EverandCalisthenics: Guide for Bodyweight Exercise, Build your Dream Body in 30 MinutesRating: 3 out of 5 stars3/5 (5)
- Roxane Gay & Everand Originals: Built for This: The Quiet Strength of PowerliftingFrom EverandRoxane Gay & Everand Originals: Built for This: The Quiet Strength of PowerliftingRating: 4.5 out of 5 stars4.5/5 (19)
- Deezify's Epic Workout Handbook: An Illustrated Guide to Getting SwoleFrom EverandDeezify's Epic Workout Handbook: An Illustrated Guide to Getting SwoleRating: 5 out of 5 stars5/5 (1)
- The Seven Spiritual Laws of Yoga: A Practical Guide to Healing Body, Mind, and SpiritFrom EverandThe Seven Spiritual Laws of Yoga: A Practical Guide to Healing Body, Mind, and SpiritRating: 4.5 out of 5 stars4.5/5 (73)