You might also like
- Sample: Georgia Department of Public HealthDocument1 pageSample: Georgia Department of Public HealthWSB-TV Assignment DeskNo ratings yet
- Protective Effectiveness of Previous SARS-CoV-2 Infection and Hybrid ImmunityDocument12 pagesProtective Effectiveness of Previous SARS-CoV-2 Infection and Hybrid ImmunityCTV CalgaryNo ratings yet
- Souvenir Book Updated Compressed-1 PDFDocument184 pagesSouvenir Book Updated Compressed-1 PDFManju Kumari100% (1)
- 2B. Deventer CalculatorDocument10 pages2B. Deventer CalculatorJhon Edi DVMNo ratings yet
- PIIS0140673620312083Document10 pagesPIIS0140673620312083kayegi8666No ratings yet
- Articles: BackgroundDocument11 pagesArticles: BackgroundCRS1973No ratings yet
- Remdesivir in Adults With Severe COVID-19: A Randomised, Double-Blind, Placebo-Controlled, Multicentre TrialDocument10 pagesRemdesivir in Adults With Severe COVID-19: A Randomised, Double-Blind, Placebo-Controlled, Multicentre TrialKinshuk ShekharNo ratings yet
- Piis0140673620310229 PDFDocument10 pagesPiis0140673620310229 PDFkayegi8666No ratings yet
- COVID 19 Vacunación en NiñosDocument13 pagesCOVID 19 Vacunación en NiñosSMIBA MedicinaNo ratings yet
- Wu 2015Document7 pagesWu 2015Noel Saúl Argüello SánchezNo ratings yet
- Sinovac JournalDocument10 pagesSinovac JournalGeulissa AddiniNo ratings yet
- Jurnal EED 3Document10 pagesJurnal EED 3Garsa GarnolNo ratings yet
- Final Efficacy Analysis, Interim Safety AnalysisDocument12 pagesFinal Efficacy Analysis, Interim Safety AnalysisGêmili BalbinotNo ratings yet
- 1 s2.0 S0140673621027537 MainDocument12 pages1 s2.0 S0140673621027537 Mainwaciy70505No ratings yet
- Artigo Lancet Coronavac 17-11-2020Document14 pagesArtigo Lancet Coronavac 17-11-2020Carlos LinsNo ratings yet
- Lectura de InmunologiaDocument10 pagesLectura de InmunologiaLuzmarina LinoNo ratings yet
- Background: OnlineDocument12 pagesBackground: OnlineCRS1973No ratings yet
- Safety, Tolerability and Immunogenicity of An Inactivated Sars-Cov-S VaccineDocument12 pagesSafety, Tolerability and Immunogenicity of An Inactivated Sars-Cov-S Vaccinezakaria alfajriNo ratings yet
- Jama Al Kaabi 2021 Oi 210057 1621966324.79302Document11 pagesJama Al Kaabi 2021 Oi 210057 1621966324.79302Rafiq Khanani DUHSNo ratings yet
- 四价登革热疫苗能有效预防亚洲健康儿童的登革热感染Document8 pages四价登革热疫苗能有效预防亚洲健康儿童的登革热感染Albert SongNo ratings yet
- CE (Ra) F (SH) PF1 (SY OM) PFA (OM) PN (KM)Document6 pagesCE (Ra) F (SH) PF1 (SY OM) PFA (OM) PN (KM)SUBHADIPNo ratings yet
- Fase 1.2Document11 pagesFase 1.2Verliatesya TugasNo ratings yet
- Efek Samping RemdesifirDocument11 pagesEfek Samping Remdesifirelsie versieNo ratings yet
- International Immunopharmacology: Meta-Analysis of Randomized Controlled TrialsDocument9 pagesInternational Immunopharmacology: Meta-Analysis of Randomized Controlled TrialsPujiNo ratings yet
- Articles: BackgroundDocument9 pagesArticles: Backgroundgilang_8899No ratings yet
- Gilbert2005 Studi HivDocument12 pagesGilbert2005 Studi HivErnawati HidayatNo ratings yet
- P009 Assessing The Status Quo Ulcerative Colitis.10Document2 pagesP009 Assessing The Status Quo Ulcerative Colitis.10Santiago ZamudioNo ratings yet
- Effectiveness of 2 Doses of Varicella Vaccine in Children: MajorarticleDocument4 pagesEffectiveness of 2 Doses of Varicella Vaccine in Children: MajorarticleYuni Eun WijayaNo ratings yet
- Candidiasis in PICUDocument6 pagesCandidiasis in PICUMeirinda HidayantiNo ratings yet
- Safety and Immunogenicity of A Heterologous Boost With A Recombinant VaccineDocument35 pagesSafety and Immunogenicity of A Heterologous Boost With A Recombinant VaccineAristegui NoticiasNo ratings yet
- MainDocument5 pagesMainFerdous HakimNo ratings yet
- Viral GeneticDocument10 pagesViral Geneticfirdaus.kabiruNo ratings yet
- PAPER FINALnejmoa2202261Document15 pagesPAPER FINALnejmoa2202261anitamanriquefcbNo ratings yet
- Safety and Immunogenicity of A Single Dose, Live-Attenuated Tetravalent Dengue Vaccine Feb 2022Document8 pagesSafety and Immunogenicity of A Single Dose, Live-Attenuated Tetravalent Dengue Vaccine Feb 2022Reinaldi octaNo ratings yet
- Articles: BackgroundDocument12 pagesArticles: BackgroundBudi Haryadi PNo ratings yet
- Different Longitudinal Patterns of Nucleic Acid and Serology Testing Results Based On Disease Severity of COVID-19 PatientsDocument5 pagesDifferent Longitudinal Patterns of Nucleic Acid and Serology Testing Results Based On Disease Severity of COVID-19 PatientsagboxNo ratings yet
- Remdesivir Covid 19Document10 pagesRemdesivir Covid 19nanaNo ratings yet
- Espondilodiscitis Infecciosa Por Patógenos Poco ComunesDocument5 pagesEspondilodiscitis Infecciosa Por Patógenos Poco ComunesOthoniel RamirezNo ratings yet
- Fase II: Oxford y AstraZeneca Publicaron en The Lancet Que Lograron 99% de Eficacia en Su Vacuna Contra El COVID-19Document15 pagesFase II: Oxford y AstraZeneca Publicaron en The Lancet Que Lograron 99% de Eficacia en Su Vacuna Contra El COVID-19Urgente24No ratings yet
- Estudio Publicado en Guangdong, China, Sobre La Contagiosidad de La Variante Delta de CoronavirusDocument18 pagesEstudio Publicado en Guangdong, China, Sobre La Contagiosidad de La Variante Delta de Coronavirussofia crottiNo ratings yet
- LC PDFDocument10 pagesLC PDFJorge Andres Balza GranadosNo ratings yet
- Nejmoa 1310422Document11 pagesNejmoa 1310422mz zumrodinNo ratings yet
- Community Acquired Pneumonia In+childrenDocument4 pagesCommunity Acquired Pneumonia In+childrendai shujuanNo ratings yet
- Pmid 36550736 IpiDocument6 pagesPmid 36550736 Ipiajaya basnetNo ratings yet
- Antibiotics 10 01088Document16 pagesAntibiotics 10 01088ahridulfoNo ratings yet
- Toxicology Reports: SciencedirectDocument6 pagesToxicology Reports: SciencedirectNoNWONo ratings yet
- Correlates of Protection Against Symptomatic and Asymptomatic Sars-Cov-2 InfectionDocument31 pagesCorrelates of Protection Against Symptomatic and Asymptomatic Sars-Cov-2 InfectionAbasyakira RaihanNo ratings yet
- High Prevalence of Azithromycin Resistance To Treponema Pallidum in Geographically Different Areas in ChinaDocument5 pagesHigh Prevalence of Azithromycin Resistance To Treponema Pallidum in Geographically Different Areas in Chinaselvia emilyaNo ratings yet
- Safety and Immunogenicity of Two RNA-Based Covid-19 Vaccine CandidatesDocument12 pagesSafety and Immunogenicity of Two RNA-Based Covid-19 Vaccine CandidatesOKE channelNo ratings yet
- Medi 96 E5864Document6 pagesMedi 96 E5864mono1144No ratings yet
- Article 1Document6 pagesArticle 1AMILA SYAZLINANo ratings yet
- Safety, Tolerability, and Immunogenicity of COVID-19 Vaccines A Systematic Review and PRE PRINTDocument31 pagesSafety, Tolerability, and Immunogenicity of COVID-19 Vaccines A Systematic Review and PRE PRINTVitória GabrieleNo ratings yet
- IDR 368857 Diagnosis and Treatment To A Post Craniotomy Intracranial inDocument7 pagesIDR 368857 Diagnosis and Treatment To A Post Craniotomy Intracranial inKadriye OvalıNo ratings yet
- Carbapenem-Pseudomonas AeruginosaDocument11 pagesCarbapenem-Pseudomonas AeruginosaMAYANo ratings yet
- Impact of Corticosteroid Therapy On Outcomes of Persons With Sars-Cov-2, Sars-Cov, or Mers-Cov Infection: A Systematic Review and Meta-AnalysisDocument9 pagesImpact of Corticosteroid Therapy On Outcomes of Persons With Sars-Cov-2, Sars-Cov, or Mers-Cov Infection: A Systematic Review and Meta-AnalysisMax CamargoNo ratings yet
- Efficacy and Safety of Rezafungin and Caspofungin in Candidaemia and Invasive CandidiasisDocument10 pagesEfficacy and Safety of Rezafungin and Caspofungin in Candidaemia and Invasive Candidiasisluis sanchezNo ratings yet
- Colistin Monotherapy Versus Combination Therapy For Carbapenem-Resistant Organisms NEJM EvidenceDocument27 pagesColistin Monotherapy Versus Combination Therapy For Carbapenem-Resistant Organisms NEJM Evidencerac.oncologyNo ratings yet
- PIIS1473309924000306Document11 pagesPIIS1473309924000306sazzad suvroNo ratings yet
- CDC Study On Effectiveness of COVID-19 VaccinesDocument8 pagesCDC Study On Effectiveness of COVID-19 VaccinesWSYX/WTTENo ratings yet
- Efficacy of Clinacanthus Nutans Extracts in PatientsDocument7 pagesEfficacy of Clinacanthus Nutans Extracts in Patientsconrad9richterNo ratings yet
- IDR 445826 Nirmatrelvir Ndash Ritonavir Reduced Mortality in HospitalizDocument11 pagesIDR 445826 Nirmatrelvir Ndash Ritonavir Reduced Mortality in HospitalizRowell NavarroNo ratings yet
- Diagnostic Imaging of Novel Coronavirus PneumoniaFrom EverandDiagnostic Imaging of Novel Coronavirus PneumoniaMinming ZhangNo ratings yet
- Rapid On-site Evaluation (ROSE): A Practical GuideFrom EverandRapid On-site Evaluation (ROSE): A Practical GuideGuoping CaiNo ratings yet
- Rates of Dark CO2 Fixation Are Driven by Microbial Biomass in A Temperate Forest SoilDocument58 pagesRates of Dark CO2 Fixation Are Driven by Microbial Biomass in A Temperate Forest SoilIsais NNo ratings yet
- Etoposide As Salvage Therapy For Cytokine Storm Due To COVID-19Document16 pagesEtoposide As Salvage Therapy For Cytokine Storm Due To COVID-19Adi permadiNo ratings yet
- Customization and External Validation of The Simplified Mortality Score For The Intensive Care Unit (SMS-ICU) in Brazilian Critically Ill PatientsDocument7 pagesCustomization and External Validation of The Simplified Mortality Score For The Intensive Care Unit (SMS-ICU) in Brazilian Critically Ill PatientsIsais NNo ratings yet
- Venous Blood Lactate Concentrations in Patients With Shock: Interesting But Not Really HelpfulDocument2 pagesVenous Blood Lactate Concentrations in Patients With Shock: Interesting But Not Really HelpfulIsais NNo ratings yet
- Risk of Incident Bleeding After Acute Kidney Injury: A Retrospective Cohort StudyDocument32 pagesRisk of Incident Bleeding After Acute Kidney Injury: A Retrospective Cohort StudyIsais NNo ratings yet
- Rates of Dark CO2 Fixation Are Driven by Microbial Biomass in A Temperate Forest SoilDocument58 pagesRates of Dark CO2 Fixation Are Driven by Microbial Biomass in A Temperate Forest SoilIsais NNo ratings yet
- The Opportunity Costs of Caring For People With Dementia in Southern SpainDocument7 pagesThe Opportunity Costs of Caring For People With Dementia in Southern SpainIsais NNo ratings yet
- Covid 19 y Tratamiento Embolia PulmonarDocument27 pagesCovid 19 y Tratamiento Embolia PulmonarSMIBA Medicina100% (1)
- Electrolyte Measurement - Myths and Misunderstandings - Part IIDocument11 pagesElectrolyte Measurement - Myths and Misunderstandings - Part IIIsais NNo ratings yet
- Should We Ban Live Surgery?Document2 pagesShould We Ban Live Surgery?Isais NNo ratings yet
- Risk of Incident Bleeding After Acute Kidney Injury: A Retrospective Cohort StudyDocument32 pagesRisk of Incident Bleeding After Acute Kidney Injury: A Retrospective Cohort StudyIsais NNo ratings yet
- Initial Assessment, Risk Stratification, and Early Management of Acute Nonvariceal Upper Gastrointestinal HemorrhageDocument15 pagesInitial Assessment, Risk Stratification, and Early Management of Acute Nonvariceal Upper Gastrointestinal HemorrhageIsais NNo ratings yet
- Inadequate Prophylactic Effect of Low-Molecular Weight Heparin in Critically Ill COVID-19 PatientsDocument4 pagesInadequate Prophylactic Effect of Low-Molecular Weight Heparin in Critically Ill COVID-19 PatientsIsais NNo ratings yet
- Emerging Endoscopic Treatments For Nonvariceal Upper Gastrointestinal HemorrhageDocument14 pagesEmerging Endoscopic Treatments For Nonvariceal Upper Gastrointestinal HemorrhageIsais NNo ratings yet
- Foreword Upper and Lower Gastrointestinal Bleeding: Everything You Need To KnowDocument2 pagesForeword Upper and Lower Gastrointestinal Bleeding: Everything You Need To KnowIsais NNo ratings yet
- Initial Assessment, Risk Stratification, and Early Management of Acute Nonvariceal Upper Gastrointestinal HemorrhageDocument15 pagesInitial Assessment, Risk Stratification, and Early Management of Acute Nonvariceal Upper Gastrointestinal HemorrhageIsais NNo ratings yet
- Development and Licensure of Vaccines To Prevent COVID-19 Guidance For IndustryDocument24 pagesDevelopment and Licensure of Vaccines To Prevent COVID-19 Guidance For IndustryIsais NNo ratings yet
- J. Hauer Et Al Leukemia 2020 PrePrintDocument8 pagesJ. Hauer Et Al Leukemia 2020 PrePrintIsais NNo ratings yet
- The Key Role of Education in The Europe 2020 Strategy: SSRN Electronic Journal October 2010Document20 pagesThe Key Role of Education in The Europe 2020 Strategy: SSRN Electronic Journal October 2010Isais NNo ratings yet
- Europe 2020: A Europe Strategy For Smart, Sustainable and Inclusive Growth.Document37 pagesEurope 2020: A Europe Strategy For Smart, Sustainable and Inclusive Growth.EKAI CenterNo ratings yet
- Endotherapy of Peptic Ulcer BleedingDocument13 pagesEndotherapy of Peptic Ulcer BleedingIsais NNo ratings yet
- The Europe 2020Document18 pagesThe Europe 2020Isais NNo ratings yet
- Vaccination Schedule: Infants Toddlers Children Adolescents AdultsDocument1 pageVaccination Schedule: Infants Toddlers Children Adolescents AdultsIsais NNo ratings yet
- Undocumented Migrants and The Europe 2020 Strategy:: Making Social Inclusion A Reality For All Migrants inDocument20 pagesUndocumented Migrants and The Europe 2020 Strategy:: Making Social Inclusion A Reality For All Migrants inIsais NNo ratings yet
- Canada-COVID-19 Vaccine Letter May 21st 2020 - UpdatedDocument4 pagesCanada-COVID-19 Vaccine Letter May 21st 2020 - UpdatedIsais NNo ratings yet
- 2020-European Semester Country-Report-Germany enDocument93 pages2020-European Semester Country-Report-Germany enIsais NNo ratings yet
- Suspending Classes Without Stopping Learning: China's Education Emergency Management Policy in The COVID-19 OutbreakDocument6 pagesSuspending Classes Without Stopping Learning: China's Education Emergency Management Policy in The COVID-19 OutbreakMeicy CimeNo ratings yet
- Covid-19: Russia Approves Vaccine Without Large Scale Testing or Published ResultsDocument2 pagesCovid-19: Russia Approves Vaccine Without Large Scale Testing or Published ResultsIsais NNo ratings yet
- Germany: Economic Growth Is Driven Increasingly by Domestic DemandDocument3 pagesGermany: Economic Growth Is Driven Increasingly by Domestic DemandIsais NNo ratings yet
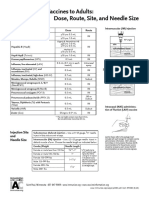
- Administering Vaccines To Adults: Dose, Route, Site, and Needle SizeDocument1 pageAdministering Vaccines To Adults: Dose, Route, Site, and Needle SizeAkashNo ratings yet
- Pediatric TB and HIV: The Potential of New TB VaccinesDocument27 pagesPediatric TB and HIV: The Potential of New TB VaccinesBarnabasNatambaNo ratings yet
- Portfolio IN Community Health Nursing: Submitted byDocument7 pagesPortfolio IN Community Health Nursing: Submitted byJay VillasotoNo ratings yet
- 67166-Apvma Veterinary Medicines Technical Report TemplateDocument42 pages67166-Apvma Veterinary Medicines Technical Report Templateali aimanNo ratings yet
- Office: Directors FOR Health OF Health Region Directors Medical Treatment RehabilitationDocument4 pagesOffice: Directors FOR Health OF Health Region Directors Medical Treatment RehabilitationDiwata OndeNo ratings yet
- Immunization P & SDocument122 pagesImmunization P & SnebilNo ratings yet
- Coronavirus (COVID-19) RecordsDocument2 pagesCoronavirus (COVID-19) RecordsVivek ElangovanNo ratings yet
- Irr Final DraftDocument7 pagesIrr Final Draftapi-571861077No ratings yet
- Annotated Bibliography Aasha TurnerDocument8 pagesAnnotated Bibliography Aasha Turnerapi-644326339No ratings yet
- Postest Imunitation-Alif Sachrul M-I1J020006-1Document3 pagesPostest Imunitation-Alif Sachrul M-I1J020006-1ARUM APRIANI 1No ratings yet
- CertificateDocument1 pageCertificateSubhajit MandalNo ratings yet
- Amicus BriefDocument27 pagesAmicus BriefThe FederalistNo ratings yet
- Perbedaan IPV Dan OPVDocument9 pagesPerbedaan IPV Dan OPVIntan SaraswatiNo ratings yet
- Materi - Webinar - Dr. Apt. Tiana Milanda, M.si.Document39 pagesMateri - Webinar - Dr. Apt. Tiana Milanda, M.si.DWI RAHMA HALIDANo ratings yet
- Aefi Reporting, Investigation & ManagementDocument23 pagesAefi Reporting, Investigation & ManagementPrabir Kumar ChatterjeeNo ratings yet
- Adjuvants Used in VaccinesDocument15 pagesAdjuvants Used in VaccinesVon Valentine MhuteNo ratings yet
- Narrative Report: Polio Outbreak Response Immunization Bopv Round 2Document4 pagesNarrative Report: Polio Outbreak Response Immunization Bopv Round 2Cristina MelloriaNo ratings yet
- Small Pox: General VirologyDocument24 pagesSmall Pox: General VirologyFahad HassanNo ratings yet
- Research Proposal: Statement in BOLD)Document4 pagesResearch Proposal: Statement in BOLD)sana mehtabNo ratings yet
- BSMT Ay 2021-2022Document45 pagesBSMT Ay 2021-2022Crystal AnnNo ratings yet
- India's COVID-19 Vaccina On Program: CFM Individual Wri/en Assignment 1Document3 pagesIndia's COVID-19 Vaccina On Program: CFM Individual Wri/en Assignment 1Ayushi ThakkarNo ratings yet
- G2 Travel COVID-19 Update - May 2021Document38 pagesG2 Travel COVID-19 Update - May 2021Megawati SyahfitriNo ratings yet
- Marketing ManagenentDocument2 pagesMarketing Managenentsiyam sharifNo ratings yet
- Harvard Epidemiologist Says The Case For COVID Vaccine Passports Was Just DemolishedDocument6 pagesHarvard Epidemiologist Says The Case For COVID Vaccine Passports Was Just DemolishedMassimo RiserboNo ratings yet
- Vaccination Certificate SyedPeerzadaAbdulYounus YZ6Ry6FmMhbMysvAaSDADocument1 pageVaccination Certificate SyedPeerzadaAbdulYounus YZ6Ry6FmMhbMysvAaSDAAbdul YounusNo ratings yet
- Community Health Nursing: Unit Title/SDocument4 pagesCommunity Health Nursing: Unit Title/SNicole LantinNo ratings yet
- Citizenship and Social Development (Sample Paper)Document7 pagesCitizenship and Social Development (Sample Paper)JamieNo ratings yet