You might also like
- Causes/Risk Factors: ModifiableDocument5 pagesCauses/Risk Factors: ModifiableDelvimalakianoNo ratings yet
- Retina Detachment, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionFrom EverandRetina Detachment, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionNo ratings yet
- Cataract ExtractionDocument4 pagesCataract Extractionselle726No ratings yet
- Surgical ProceduresDocument20 pagesSurgical ProceduresfheisanzNo ratings yet
- NCM 116: Care of Clients With Problems in Nutrition and Gastrointestinal, Metabolism and Endocrine,, Acute and ChronicDocument18 pagesNCM 116: Care of Clients With Problems in Nutrition and Gastrointestinal, Metabolism and Endocrine,, Acute and ChronicDiego DumauaNo ratings yet
- CD 6 OphthalmologyDocument7 pagesCD 6 OphthalmologyؤيؤييسيNo ratings yet
- JaniceDocument2 pagesJaniceCrystal Ivy AgpaoaNo ratings yet
- Determining Visual Acuity: Ocular EmergenciesDocument6 pagesDetermining Visual Acuity: Ocular Emergenciesendang kurniatiNo ratings yet
- PL802Document16 pagesPL802Nazir IsmailovNo ratings yet
- Ost Operative Care: General Instructions For Post Operative Patients After Eye SurgeryDocument29 pagesOst Operative Care: General Instructions For Post Operative Patients After Eye SurgerymalathiNo ratings yet
- Nursing Care of Clients Undergoing Eye SurgeryDocument1 pageNursing Care of Clients Undergoing Eye SurgerySewyel GarburiNo ratings yet
- Cataract SurgeryDocument14 pagesCataract SurgeryRenato AbellaNo ratings yet
- Assessment of The EYESDocument64 pagesAssessment of The EYESAlliah Marie CababarosNo ratings yet
- Activity5 (Retinal Detachment)Document3 pagesActivity5 (Retinal Detachment)Gabbii CincoNo ratings yet
- Eye, Ear, and Throat DisordersDocument95 pagesEye, Ear, and Throat DisordersGil Platon SorianoNo ratings yet
- Cataract CasestudyDocument3 pagesCataract CasestudyJamal AgontongNo ratings yet
- Pre and Post Op Care of Cataract in MCHDocument4 pagesPre and Post Op Care of Cataract in MCHAthira PSNo ratings yet
- MS Eye and Vision DisordersDocument78 pagesMS Eye and Vision DisordersAntoinette Sallan NopiaNo ratings yet
- Common Eye Problems in ChildrenDocument6 pagesCommon Eye Problems in ChildrentheglobalnursingNo ratings yet
- Nursing care plan for cataract patientsDocument2 pagesNursing care plan for cataract patientsMicky Zelia100% (3)
- Disturbance in Sensory PerceptionDocument48 pagesDisturbance in Sensory PerceptionKristine Louise JavierNo ratings yet
- Eye DisordersDocument14 pagesEye DisordersAireen Grace GilosNo ratings yet
- Cataract Types, Causes, Symptoms & TreatmentDocument3 pagesCataract Types, Causes, Symptoms & TreatmentShereen ManabilangNo ratings yet
- Rationale of Ms Exam October 18, 2022Document15 pagesRationale of Ms Exam October 18, 2022Felimon BugtongNo ratings yet
- CataractDocument7 pagesCataractaltfanz_044454No ratings yet
- Sensory Practice TestDocument19 pagesSensory Practice TestJennelyn GinturoNo ratings yet
- EENTDocument52 pagesEENTdr2tin100% (1)
- Laser-Assisted in Situ KeratomileusisDocument3 pagesLaser-Assisted in Situ KeratomileusisJoe RealNo ratings yet
- Visual Nursing Bullets Eye Care GuideDocument3 pagesVisual Nursing Bullets Eye Care GuideDonaJeanNo ratings yet
- Glaucoma and CataractDocument30 pagesGlaucoma and CataractJayselle ArvieNo ratings yet
- Special Senses Post TestDocument10 pagesSpecial Senses Post TestAngie RelosNo ratings yet
- Cataract PTDocument9 pagesCataract PTPreeti SharmaNo ratings yet
- Cataract PTDocument9 pagesCataract PTpreeti sharmaNo ratings yet
- CA Eye and Ear DisorderDocument20 pagesCA Eye and Ear DisorderEsmareldah Henry Sirue100% (1)
- Care of Patients with Neurosensory DisordersDocument18 pagesCare of Patients with Neurosensory DisordersSIJINo ratings yet
- CATARACTSDocument2 pagesCATARACTSHanee Kaye TagubaNo ratings yet
- Irrigation of The EyeDocument10 pagesIrrigation of The EyeissaiahnicolleNo ratings yet
- Cataract Information For Patients: and Click On Wait Times TabDocument13 pagesCataract Information For Patients: and Click On Wait Times TabVidini Kusuma AjiNo ratings yet
- Drugs Used To Treat Glaucoma and Other EyeDocument38 pagesDrugs Used To Treat Glaucoma and Other Eyerenz bartolomeNo ratings yet
- Eye Instillation Procedure Guide NursingDocument3 pagesEye Instillation Procedure Guide NursingTrisha ApillanesNo ratings yet
- Glaucoma 191024141130Document25 pagesGlaucoma 191024141130Broz100% (1)
- Introduction, Health History, GordonsDocument10 pagesIntroduction, Health History, GordonsKayelyn-Rose CombateNo ratings yet
- GlaucomaDocument3 pagesGlaucomaPuviyarasiNo ratings yet
- Retinal Detachment GuideDocument21 pagesRetinal Detachment GuideRose O'SullivanNo ratings yet
- Cataract: Case Presentation - M.E.T.H.O.DDocument7 pagesCataract: Case Presentation - M.E.T.H.O.DKismet SummonsNo ratings yet
- Disorders of The EyeDocument16 pagesDisorders of The Eyelisette_sakuraNo ratings yet
- Guide to Cataract Surgery RecoveryDocument16 pagesGuide to Cataract Surgery Recoverydokumen kuNo ratings yet
- Eye Irrig RDDocument3 pagesEye Irrig RDJames Kristopher RebayaNo ratings yet
- NCP CataractDocument2 pagesNCP CataractMaureen Gay Acierto Tegui67% (3)
- Nursing Diagnosis For CataractDocument3 pagesNursing Diagnosis For CataractZainul HazwanNo ratings yet
- Invasive ProceduresDocument12 pagesInvasive ProceduresMay-AnnJoyRedoñaNo ratings yet
- EchothiophateDocument5 pagesEchothiophaterarasNo ratings yet
- Special EmergenciesDocument152 pagesSpecial EmergenciesJannell LawesNo ratings yet
- 05 DamageEye2017Document6 pages05 DamageEye2017sudhirksingh27No ratings yet
- Best Practices Procedure For Instillation of Eye DropsDocument1 pageBest Practices Procedure For Instillation of Eye DropsRahul ModiNo ratings yet
- Northern Medical Colleges Cataract CaseDocument4 pagesNorthern Medical Colleges Cataract CaseSIJINo ratings yet
- ExenterationDocument3 pagesExenterationMohammad Abdullah BawtagNo ratings yet
- Ocular Maneuvers EnglezaDocument6 pagesOcular Maneuvers EnglezaAlexa DyanaNo ratings yet
- 1 - MyopiaDocument9 pages1 - MyopiaSpislgal PhilipNo ratings yet
- Wanna One - Burn It UpDocument7 pagesWanna One - Burn It UpDelvimalakianoNo ratings yet
- Emergency management of oromaxillofacial trauma with anterior cranial base fracturesDocument1 pageEmergency management of oromaxillofacial trauma with anterior cranial base fracturesDelvimalakianoNo ratings yet
- Un Woman - Australia - ST Nurhazana SDocument2 pagesUn Woman - Australia - ST Nurhazana SDelvimalakianoNo ratings yet
- AssesmentDocument4 pagesAssesmentDelvimalakianoNo ratings yet
- Wanna One - Burn It UpDocument7 pagesWanna One - Burn It UpDelvimalakianoNo ratings yet
- Grammar TestDocument1 pageGrammar TestDelvimalakianoNo ratings yet
- Repository - Usu.ac - Id/bitstream/123456789/25638/4/chapter II PDFDocument1 pageRepository - Usu.ac - Id/bitstream/123456789/25638/4/chapter II PDFDelvimalakianoNo ratings yet
- Grammar TestDocument1 pageGrammar TestDelvimalakianoNo ratings yet
- 2017-02-02 - Moneysaver - Lewis-Clark EditionDocument20 pages2017-02-02 - Moneysaver - Lewis-Clark EditionDavid ArndtNo ratings yet
- Dual-band patch antenna for 5G applicationsDocument3 pagesDual-band patch antenna for 5G applicationsHarini VemulaNo ratings yet
- 524 799 Coach - K - Coach - Knight - CaseDocument15 pages524 799 Coach - K - Coach - Knight - Casekaushalmighty100% (1)
- Systematic Review of The Market Wide Herding Behavior in Asian RegionDocument9 pagesSystematic Review of The Market Wide Herding Behavior in Asian RegionIJAR JOURNALNo ratings yet
- InvoiceDocument2 pagesInvoiceamalNo ratings yet
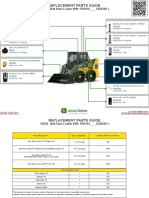
- 312GR Skid Steer Loader PIN 1T0312G G366358 Replacement Parts GuideDocument3 pages312GR Skid Steer Loader PIN 1T0312G G366358 Replacement Parts GuideNelson Andrade VelasquezNo ratings yet
- Hotel Reservation System: Hotel OAK-RAY, KandyDocument22 pagesHotel Reservation System: Hotel OAK-RAY, KandysaminaNo ratings yet
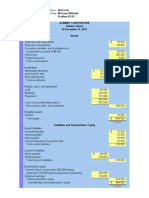
- Working Capital Management OF: Submitted by Priya BanerjeeDocument102 pagesWorking Capital Management OF: Submitted by Priya BanerjeeSushmita BarlaNo ratings yet
- Branding Strategy Mcvities PDFDocument13 pagesBranding Strategy Mcvities PDFrishab sablokNo ratings yet
- Group 3 - Brand Architecture Assignment IDocument9 pagesGroup 3 - Brand Architecture Assignment IShijin SreekumarNo ratings yet
- Licence Acoknowledgement SlipDocument1 pageLicence Acoknowledgement SlipBicky ChoudhuryNo ratings yet
- Volume 7 Issue 4Document12 pagesVolume 7 Issue 4thestuyvesantstandardNo ratings yet
- EIA For Maize & Wheat Milling Plant DEI PDFDocument110 pagesEIA For Maize & Wheat Milling Plant DEI PDFSasira Fionah100% (2)
- Test Bank For Web Development and Design Foundations With Html5 6 e 6th Edition 0132783398Document9 pagesTest Bank For Web Development and Design Foundations With Html5 6 e 6th Edition 0132783398Thomas White100% (23)
- CS 702 Lec10Document9 pagesCS 702 Lec10Muhammad TausifNo ratings yet
- 9 Principles of Income Tax LawsDocument82 pages9 Principles of Income Tax LawsVyankatesh GotalkarNo ratings yet
- Electricity (Innovative Licence) Regulations 2023Document16 pagesElectricity (Innovative Licence) Regulations 2023BernewsAdminNo ratings yet
- Bangladesh Labour Rights ResearchDocument29 pagesBangladesh Labour Rights ResearchMd. Hasan Ali JoyNo ratings yet
- Revised Circular On Secretariat Meeting Held On 9th July, 2023Document4 pagesRevised Circular On Secretariat Meeting Held On 9th July, 2023Mohit SoniNo ratings yet
- A Geometric Method For Kinematics of Delta Robot and Its Path Tracking Control PDFDocument6 pagesA Geometric Method For Kinematics of Delta Robot and Its Path Tracking Control PDFJameszouqunNo ratings yet
- Power Converters Simulation Lab Manual - (2015-2016)Document41 pagesPower Converters Simulation Lab Manual - (2015-2016)Leela KrishnaNo ratings yet
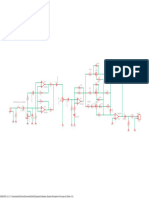
- Unbalanced Dynamic Microphone Pre-AmpDocument1 pageUnbalanced Dynamic Microphone Pre-AmpAhmad FauziNo ratings yet
- Chapter 3 - Excel SolutionsDocument8 pagesChapter 3 - Excel SolutionsHalt DougNo ratings yet
- Craftsman: TractorDocument64 pagesCraftsman: TractorsNo ratings yet
- 9211 4 PR PE Utility Industry Low Product Range 2017Document226 pages9211 4 PR PE Utility Industry Low Product Range 2017Soporte SyeNo ratings yet
- Ideal Home - Complete Guide To Christmas 2016 PDFDocument148 pagesIdeal Home - Complete Guide To Christmas 2016 PDFpetru555100% (2)
- 4 AppleDocument9 pages4 AppleSam Peter GeorgieNo ratings yet
- Missing Dovetail RfiDocument1 pageMissing Dovetail RfiPurushotam TapariyaNo ratings yet
- 11.30 Imran Akram IA CementDocument12 pages11.30 Imran Akram IA CementParamananda SinghNo ratings yet
- LAS IN ENTREPRENEURSHIP WEEK 4Document5 pagesLAS IN ENTREPRENEURSHIP WEEK 4IMELDA CORONACIONNo ratings yet
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (14)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 3.5 out of 5 stars3.5/5 (2)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 3.5 out of 5 stars3.5/5 (33)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 5 out of 5 stars5/5 (5)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisFrom EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisRating: 5 out of 5 stars5/5 (8)