You might also like
- Sudden Cardiac Death and SportDocument38 pagesSudden Cardiac Death and SportSoad ShedeedNo ratings yet
- Molecular Covid19Document7 pagesMolecular Covid19Calvin LitraNo ratings yet
- How To Balance Acute Myocardial Infarction and COVID-19 - The Protocols From Sichuan Provincial People's HospitalDocument3 pagesHow To Balance Acute Myocardial Infarction and COVID-19 - The Protocols From Sichuan Provincial People's HospitalDedeSumantraNo ratings yet
- Acute Coronary Syndrome & The PLATO Trial: Ticagrelor vs. ClopidogrelDocument42 pagesAcute Coronary Syndrome & The PLATO Trial: Ticagrelor vs. ClopidogrelDedeSumantraNo ratings yet
- Terms of The Creative Commons Attribution Share Alike-3.0 LicenseDocument45 pagesTerms of The Creative Commons Attribution Share Alike-3.0 LicenseDedeSumantraNo ratings yet
- 01 Cir 100 9 918Document6 pages01 Cir 100 9 918DedeSumantraNo ratings yet
- Current Strategy For Treatment of Patients With Wolff-Parkinson-White Syndrome and Asymptomatic PreexcitationDocument4 pagesCurrent Strategy For Treatment of Patients With Wolff-Parkinson-White Syndrome and Asymptomatic PreexcitationDedeSumantraNo ratings yet
- HRS Guidelines For SVT ManagementDocument86 pagesHRS Guidelines For SVT ManagementchirudarsiNo ratings yet
- Localization and Radiofrequency Catheter Ablation of Left-Sided Accessory Pathways During Atria1 FibrillationDocument8 pagesLocalization and Radiofrequency Catheter Ablation of Left-Sided Accessory Pathways During Atria1 FibrillationDedeSumantraNo ratings yet
- Current Strategy For Treatment of Patients With Wolff-Parkinson-White Syndrome and Asymptomatic PreexcitationDocument4 pagesCurrent Strategy For Treatment of Patients With Wolff-Parkinson-White Syndrome and Asymptomatic PreexcitationDedeSumantraNo ratings yet
- Kose 2005Document5 pagesKose 2005DedeSumantraNo ratings yet
- Echocardiographic Quantification of Left Ventricular Systolic FunctionDocument4 pagesEchocardiographic Quantification of Left Ventricular Systolic FunctionDedeSumantraNo ratings yet
- SulfonilureaDocument8 pagesSulfonilureaDedeSumantraNo ratings yet
- Factors Determining Success in Percutaneous Revascularization of Chronic Total Coronary OcclusionDocument7 pagesFactors Determining Success in Percutaneous Revascularization of Chronic Total Coronary OcclusionDedeSumantraNo ratings yet
- DIGOXINDocument19 pagesDIGOXINDedeSumantraNo ratings yet
- Beneficial Effects of Endurance Training On Cardiac and Skeletal Muscle Energy Metabolism in Heart FailureDocument9 pagesBeneficial Effects of Endurance Training On Cardiac and Skeletal Muscle Energy Metabolism in Heart FailureDedeSumantraNo ratings yet
- Kwan Obscure GI BleedDocument16 pagesKwan Obscure GI BleedDedeSumantraNo ratings yet
- Early Vs Delayed Surgical in IEDocument9 pagesEarly Vs Delayed Surgical in IEDedeSumantraNo ratings yet
- Prevention of Activation of Blood Coagulation During Acute Coronary Ischemic Syndromes - Beyond Aspirin and HeparinDocument15 pagesPrevention of Activation of Blood Coagulation During Acute Coronary Ischemic Syndromes - Beyond Aspirin and HeparinDedeSumantraNo ratings yet
- Neuropsychology of Bipolar Disorder: References ReprintsDocument9 pagesNeuropsychology of Bipolar Disorder: References ReprintsDedeSumantraNo ratings yet
- BMC Rehab ResearchDocument4 pagesBMC Rehab ResearchDedeSumantraNo ratings yet
- Exercise Stress-Budi AriefDocument11 pagesExercise Stress-Budi AriefDedeSumantraNo ratings yet
- Neuropsychology of Bipolar Disorder: References ReprintsDocument9 pagesNeuropsychology of Bipolar Disorder: References ReprintsDedeSumantraNo ratings yet
- Price ListDocument2 pagesPrice ListDedeSumantraNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- PNLE III For Care of Clients With Physiologic and Psychosocial AlterationsDocument10 pagesPNLE III For Care of Clients With Physiologic and Psychosocial AlterationsANGELINE PALATINO100% (1)
- Goat anatomy and physiology guideDocument8 pagesGoat anatomy and physiology guideLochi GmNo ratings yet
- Allis Chalmers 840 840b Articulated Wheel Loader Forklift Parts CatalogDocument20 pagesAllis Chalmers 840 840b Articulated Wheel Loader Forklift Parts CatalogCarl100% (42)
- Snap-On EEDM504D ManualDocument15 pagesSnap-On EEDM504D ManualSnafu168No ratings yet
- Text CDocument1,100 pagesText CAli NofalNo ratings yet
- MD Lecture 1 - Intro To MDDocument19 pagesMD Lecture 1 - Intro To MDADITYA VERMANo ratings yet
- Father Dámaso: María Clara Quotes in Noli Me TangereDocument11 pagesFather Dámaso: María Clara Quotes in Noli Me TangereSilver ArgentNo ratings yet
- Water SprayDocument2 pagesWater SpraySaba SamankanNo ratings yet
- How to Give a Woman the Most Powerful OrgasmDocument10 pagesHow to Give a Woman the Most Powerful OrgasmFederico Ceferino BrizuelaNo ratings yet
- Format No. 1-2019-PSS-01 Rev.1Document1 pageFormat No. 1-2019-PSS-01 Rev.1nithinNo ratings yet
- In Situ Cell Death KitDocument27 pagesIn Situ Cell Death KitckapodisNo ratings yet
- Econ Double Regulating ValvesDocument18 pagesEcon Double Regulating ValvesElimKaAdda100% (1)
- PROJECT IMS QEHS PLAN LEGAL REGISTERDocument4 pagesPROJECT IMS QEHS PLAN LEGAL REGISTERPriyanka JNo ratings yet
- The Scientific Facts About WaterDocument7 pagesThe Scientific Facts About WaterNizam HasniNo ratings yet
- UK-India Coffee Market ReportDocument27 pagesUK-India Coffee Market ReportNikhil MunjalNo ratings yet
- C CA AS SC CL Liin Niiq QU UE E // C CA AS SE ER RE EP PO OR RT TDocument7 pagesC CA AS SC CL Liin Niiq QU UE E // C CA AS SE ER RE EP PO OR RT TG Virucha Meivila IINo ratings yet
- PAES 422-1-2012 - Agricultural Structures - Poultry Dressing Slaughtering Plan - Part 1 Small Sca PDFDocument32 pagesPAES 422-1-2012 - Agricultural Structures - Poultry Dressing Slaughtering Plan - Part 1 Small Sca PDFJohn VelacioNo ratings yet
- Surgery Hazel Final1Document21 pagesSurgery Hazel Final1Sittie RamosNo ratings yet
- Axell Wireless Cellular Coverage Solutions BrochureDocument8 pagesAxell Wireless Cellular Coverage Solutions BrochureBikash ShakyaNo ratings yet
- BurgerKing Versus McDonaldsDocument4 pagesBurgerKing Versus McDonaldsmarkus johannessenNo ratings yet
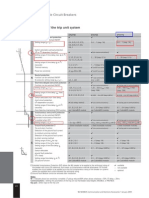
- ETU 776 TripDocument1 pageETU 776 TripbhaskarinvuNo ratings yet
- National Ehealth: "Moving Towards Efficient Healthcare"Document30 pagesNational Ehealth: "Moving Towards Efficient Healthcare"nurul fatma diyanaNo ratings yet
- Euphoria Special Edition Rue ScriptDocument24 pagesEuphoria Special Edition Rue ScriptMoldovan EdithNo ratings yet
- Can You Distinguish Neutral, Formal and Informal Among The Following Groups of WordsDocument3 pagesCan You Distinguish Neutral, Formal and Informal Among The Following Groups of WordsВікторія РудаNo ratings yet
- Service Manual: Side by Side S20B RSB21-A/GDocument16 pagesService Manual: Side by Side S20B RSB21-A/GjicutuNo ratings yet
- TBT Accident Prevention 1Document2 pagesTBT Accident Prevention 1zaimNo ratings yet
- Introduction To CommerceDocument30 pagesIntroduction To Commerceapi-24690719591% (11)
- Fundamentals of Compressible Flow: Measurement Diagnostics and Experimental Facilities For Compressible FlowDocument6 pagesFundamentals of Compressible Flow: Measurement Diagnostics and Experimental Facilities For Compressible Flowkushal bosuNo ratings yet
- MBR-STP Design Features PDFDocument7 pagesMBR-STP Design Features PDFManjunath HrmNo ratings yet
- Auto TransformerDocument16 pagesAuto TransformerMaisarahNo ratings yet