You might also like
- BARNES Liver InjuryDocument66 pagesBARNES Liver Injurycrt0518No ratings yet
- Aneurysms & Aortic DissectionDocument36 pagesAneurysms & Aortic Dissectionr100% (1)
- Veeam Certified Engineer Training Program: TextbookDocument203 pagesVeeam Certified Engineer Training Program: TextbookJump AroundNo ratings yet
- Guidelines TAVI TAVRDocument15 pagesGuidelines TAVI TAVRRossellaDisalvo100% (1)
- CABGDocument3 pagesCABGprofarmahNo ratings yet
- Tavi 150923155743 Lva1 App6892Document157 pagesTavi 150923155743 Lva1 App6892Zhivka Kostadinova100% (1)
- 1 Surgery McqsDocument29 pages1 Surgery McqsSherlockHolmesSez50% (6)
- Liver Trauma: DR Tarik El Batrawy Specialist General SurgeryDocument50 pagesLiver Trauma: DR Tarik El Batrawy Specialist General Surgerykata61No ratings yet
- Unit 6 Cardiac Catheterization and AngiographyDocument28 pagesUnit 6 Cardiac Catheterization and AngiographyJack Tomar100% (1)
- HYDRO-GUARD® Water-Based Drilling Fluid Delivering Stable Wellbore ThroughDocument1 pageHYDRO-GUARD® Water-Based Drilling Fluid Delivering Stable Wellbore ThroughFauzan Rahman HaqNo ratings yet
- Thoracic and Abdominal TraumaDocument76 pagesThoracic and Abdominal Traumajhk0428100% (1)
- Flange Loading CheckDocument48 pagesFlange Loading CheckrefuzerNo ratings yet
- Trauma Ginjal: Sub Bagian Urologi Bagian/Smf Bedah FK Uns/Rsud Dr. MoewardiDocument39 pagesTrauma Ginjal: Sub Bagian Urologi Bagian/Smf Bedah FK Uns/Rsud Dr. MoewardiAtika SugiartoNo ratings yet
- RADIO 250 (8) LEC 11 Introduction To Interventional RadiologyDocument4 pagesRADIO 250 (8) LEC 11 Introduction To Interventional Radiologyjmhinos4833No ratings yet
- Jeppesen C-Map Professional Cm93 v3 Wf766Document5 pagesJeppesen C-Map Professional Cm93 v3 Wf766Ihwan Asrul100% (1)
- Questionnaire For Urban Planning PracticalDocument5 pagesQuestionnaire For Urban Planning PracticalNaeem Akhtar Samoon75% (4)
- ACFrOgBJ11ZY9WD49wZ4mx Nu2QyGvK-qmOsUHKXVRSBkfEbfwWLzfDaE3L9 rejnh0YFVdwEJYzgZnIKRyT1AcSkbIft12Sqr5t7NCHqRd2MZQD7DJSwhSvGVKwQbTUPSaBLuf75yV EO1CV72IDocument8 pagesACFrOgBJ11ZY9WD49wZ4mx Nu2QyGvK-qmOsUHKXVRSBkfEbfwWLzfDaE3L9 rejnh0YFVdwEJYzgZnIKRyT1AcSkbIft12Sqr5t7NCHqRd2MZQD7DJSwhSvGVKwQbTUPSaBLuf75yV EO1CV72Iمحمد سعد طهNo ratings yet
- Aorta Replacement and Repair Thoracic Aortic DissectionDocument3 pagesAorta Replacement and Repair Thoracic Aortic DissectionprofarmahNo ratings yet
- CA Gall BladderDocument24 pagesCA Gall BladderTheoder RobinsonNo ratings yet
- Adjuvant Pancreas (Post-Op) AtlasDocument31 pagesAdjuvant Pancreas (Post-Op) AtlasDetelina Walchewa-Nedewa100% (1)
- How To Do Aorta InterventionDocument80 pagesHow To Do Aorta InterventionMohamad ZulfikarNo ratings yet
- Renal Trauma: Classification and Grading: Trauma To The Urinary TractDocument12 pagesRenal Trauma: Classification and Grading: Trauma To The Urinary Tractصلاح الدين الحكيمNo ratings yet
- Radical Surgery For Cancer of The Pancreas: Kothaj PDocument3 pagesRadical Surgery For Cancer of The Pancreas: Kothaj Pyacine26No ratings yet
- Billiary SurgeriesDocument37 pagesBilliary Surgeriesgeorvin marcoNo ratings yet
- CT LiverDocument12 pagesCT LiverWaiz ChNo ratings yet
- M.04 Liver (Part 4) (Dr. Cinio) (10-29-20)Document8 pagesM.04 Liver (Part 4) (Dr. Cinio) (10-29-20)VanessaNo ratings yet
- ABC of Liver and Pancreatic TraumaDocument3 pagesABC of Liver and Pancreatic TraumaDiana DeciuNo ratings yet
- Application of Half Liver Vascular Occlusion Combined With Hepatic Veins Occlusion in Complex Precise Liver Resection of Hepatocellular CarcinomaDocument4 pagesApplication of Half Liver Vascular Occlusion Combined With Hepatic Veins Occlusion in Complex Precise Liver Resection of Hepatocellular CarcinomaOncología CdsNo ratings yet
- ARROcase Borderline Resectable Pancreas JordanKharofaDocument20 pagesARROcase Borderline Resectable Pancreas JordanKharofaArtist ArtistNo ratings yet
- Peitzman Trauma HepáticoDocument11 pagesPeitzman Trauma HepáticoLety Carmona ArevaloNo ratings yet
- Management of Traumatic Liver Injuries: DR Junaid Ahmad SofiDocument80 pagesManagement of Traumatic Liver Injuries: DR Junaid Ahmad SofiNatalindah Jokiem Woecandra T. D.No ratings yet
- Cardiothoracics ReviewDocument44 pagesCardiothoracics ReviewGrace LNo ratings yet
- Ninomiya 等 - 2020 - Clip on Staple Method to Prevent Bile Leakage in ADocument4 pagesNinomiya 等 - 2020 - Clip on Staple Method to Prevent Bile Leakage in A蔡一鹏No ratings yet
- The LiverDocument13 pagesThe LiverLizbeth QuinteroNo ratings yet
- Bab 12 TuberkulosisDocument22 pagesBab 12 TuberkulosisnursyahilaNo ratings yet
- Hipertensi Portal Donny SandraDocument67 pagesHipertensi Portal Donny SandrabobyNo ratings yet
- Site: Course: Hepatocellular Carcinoma Book: Learning Materials Printed By:david Ryan Date: Friday, 10 April 2020, 2:04 AMDocument14 pagesSite: Course: Hepatocellular Carcinoma Book: Learning Materials Printed By:david Ryan Date: Friday, 10 April 2020, 2:04 AMDavid RyanNo ratings yet
- 16-Slice CT Hepatic Venography: Pictorial EssayDocument7 pages16-Slice CT Hepatic Venography: Pictorial EssayphuocthuyetNo ratings yet
- (RADIO 250) LEC 08 Introduction To Interventional RadiologyDocument4 pages(RADIO 250) LEC 08 Introduction To Interventional RadiologyWilliam PinzonNo ratings yet
- Liver: What Is TheDocument37 pagesLiver: What Is TheAnkur MandeliaNo ratings yet
- BookDocument21 pagesBookShaastieNo ratings yet
- Insertion of Umbilical Lines in NeonatesDocument6 pagesInsertion of Umbilical Lines in Neonatesgaaneshsubra5No ratings yet
- RCA OstijalnaDocument8 pagesRCA Ostijalnaediz71No ratings yet
- CT Contrast Injection and ProtocolsDocument35 pagesCT Contrast Injection and ProtocolskeziasNo ratings yet
- The Spleen: Splenic Trauma and Splenectomy: TrunkDocument3 pagesThe Spleen: Splenic Trauma and Splenectomy: TrunkAsish GeiorgeNo ratings yet
- CT ProtocolsDocument62 pagesCT ProtocolssanyengereNo ratings yet
- Sakamoto 2017Document6 pagesSakamoto 2017Chris WuNo ratings yet
- Cervix DelineationDocument22 pagesCervix Delineationfadli puteraNo ratings yet
- Surgical Management of Benign Causes of Obstructive JaundiceDocument29 pagesSurgical Management of Benign Causes of Obstructive JaundiceNaviNo ratings yet
- Colecistogastrostomia-Biopsia de HigadoDocument8 pagesColecistogastrostomia-Biopsia de HigadoWildor Herrera GuevaraNo ratings yet
- Laparoscopic Cholecystectomy - StatPearls - NCBI BookshelfDocument1 pageLaparoscopic Cholecystectomy - StatPearls - NCBI BookshelfOmar HamwiNo ratings yet
- Budd Chiari SyndromeDocument37 pagesBudd Chiari SyndromeNader SaadNo ratings yet
- Word - TEVARDocument6 pagesWord - TEVARPutra AchmadNo ratings yet
- Management of Abdominal Vascular Injury: DR Bashir Bin Yunus General Surgry Unit Akth 3/12/18Document62 pagesManagement of Abdominal Vascular Injury: DR Bashir Bin Yunus General Surgry Unit Akth 3/12/18Fendry KolondamNo ratings yet
- EAU 2024 Pocket GuidelinesDocument571 pagesEAU 2024 Pocket Guidelinesgreatkhanjee82No ratings yet
- Aortic Aneurysm: DR Rahul CDocument79 pagesAortic Aneurysm: DR Rahul CIrwan Meidi LubisNo ratings yet
- 2-Liver Surgery BasicsDocument14 pages2-Liver Surgery Basicsrobertvergara.rbgmNo ratings yet
- Management of Rectal Cancer... by DR Kassahun GirmaDocument50 pagesManagement of Rectal Cancer... by DR Kassahun GirmaKassahun Girma Gelaw100% (1)
- Dynamic Abdominal CTDocument42 pagesDynamic Abdominal CTfauziNo ratings yet
- Gi Bleed RadiologyDocument60 pagesGi Bleed RadiologyDINESHNo ratings yet
- Esophageal Carcinoma: Mark Louie M. Lanting, MDDocument44 pagesEsophageal Carcinoma: Mark Louie M. Lanting, MDlouie10279098No ratings yet
- Colorectal CA CME-CVLDocument32 pagesColorectal CA CME-CVLAbu ZidaneNo ratings yet
- Genitourinary Trauma: Kidney, Ureter, Bladder, Urethra, GenitaliaDocument42 pagesGenitourinary Trauma: Kidney, Ureter, Bladder, Urethra, GenitaliaOrin SujasmanNo ratings yet
- MKN 050Document5 pagesMKN 050sharondsouza14No ratings yet
- Difficult Acute Cholecystitis: Treatment and Technical IssuesFrom EverandDifficult Acute Cholecystitis: Treatment and Technical IssuesNo ratings yet
- Lecture-22 Prolonged PregnancyDocument24 pagesLecture-22 Prolonged PregnancyMadhu Sudhan PandeyaNo ratings yet
- 34-Digital Marketing Assignment BriefDocument3 pages34-Digital Marketing Assignment BriefNabeel hassanNo ratings yet
- Review 11 - Linking VerbsDocument1 pageReview 11 - Linking VerbsCindy TranNo ratings yet
- Surg2 Primary Aldosteronism AssignmentDocument8 pagesSurg2 Primary Aldosteronism AssignmentDarain Mohammed MeirNo ratings yet
- Antibiotics in The Swine IndustryDocument10 pagesAntibiotics in The Swine IndustryCameronNo ratings yet
- Antisol - 15Document3 pagesAntisol - 15Hakan KuruoğluNo ratings yet
- GS33J01A10-01EN Main Centum VP Part Selection R6Document40 pagesGS33J01A10-01EN Main Centum VP Part Selection R6timsar1357No ratings yet
- Quang L Minh-New SAT Practise Test - ExamPrintReportDocument41 pagesQuang L Minh-New SAT Practise Test - ExamPrintReportKhoa NhậtNo ratings yet
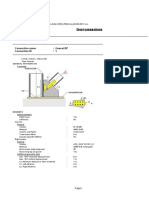
- Steel Connections: Detailed ReportDocument7 pagesSteel Connections: Detailed Reportgv Sathishkumar KumarNo ratings yet
- Walter J. Matweychuk, PH.DDocument3 pagesWalter J. Matweychuk, PH.DVenica AllenNo ratings yet
- 2.1 Linear Static Analysis Procedure, LSPDocument3 pages2.1 Linear Static Analysis Procedure, LSPSrinivas NagarajNo ratings yet
- Some Simple Economics of BlockchainDocument39 pagesSome Simple Economics of BlockchainVijay KumarNo ratings yet
- Sikafloor - 325: 2-Part PUR Resin Self Smoothing Screed and Seal CoatDocument6 pagesSikafloor - 325: 2-Part PUR Resin Self Smoothing Screed and Seal CoatmilanbrasinaNo ratings yet
- DLL Science-6 Q3 W6Document4 pagesDLL Science-6 Q3 W6juvelyn.aclaoNo ratings yet
- Handbook: Handbook FST + CAN-BUS 1Document35 pagesHandbook: Handbook FST + CAN-BUS 1ngelectronic5226No ratings yet
- Reported Speech Don T Look Up Subs Activity 3Document6 pagesReported Speech Don T Look Up Subs Activity 3Louis RousselNo ratings yet
- Draft Award Letter - GlobalDocument2 pagesDraft Award Letter - GlobalV U P RaoNo ratings yet
- Yehezkiel Girsang - Karya Tulis IlmiahDocument12 pagesYehezkiel Girsang - Karya Tulis Ilmiahkielo grsgNo ratings yet
- MP Lab ManualDocument11 pagesMP Lab ManualRaj KumarNo ratings yet
- Student ID Number:: KIT501 ICT Systems Administration FundamentalsDocument5 pagesStudent ID Number:: KIT501 ICT Systems Administration FundamentalsreachranandNo ratings yet
- Overload Relays: 6/14 DescriptionDocument18 pagesOverload Relays: 6/14 DescriptionPedro Joel AguilarNo ratings yet
- Curriculum Vitae Anthony DacunoDocument2 pagesCurriculum Vitae Anthony DacunoanthonyNo ratings yet
- Free Download Scattering Methods and Their Application in Colloid and Interface Science Otto Glatter Full Chapter PDFDocument51 pagesFree Download Scattering Methods and Their Application in Colloid and Interface Science Otto Glatter Full Chapter PDFjake.hernandez483100% (17)
- PKK Kanak-Kanak Berkeperluan KhasDocument11 pagesPKK Kanak-Kanak Berkeperluan Khassyisyirararoro100% (1)
- Tremere NethanusDocument4 pagesTremere NethanusNataniel RibeiroNo ratings yet