You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Control System InstrumentationDocument88 pagesControl System Instrumentationyeay_meNo ratings yet
- Yamaha Yas-207 - Ats-2070 - Cu207 - Ats-Cu2070 - ns-wsw42 PDFDocument50 pagesYamaha Yas-207 - Ats-2070 - Cu207 - Ats-Cu2070 - ns-wsw42 PDFboroda241050% (2)
- Canada - Policy Toolkit For Public Involvement PDFDocument155 pagesCanada - Policy Toolkit For Public Involvement PDFFundación Ellen Riegner de CasasNo ratings yet
- Comparison of The Content of Tobacco Alkaloids and Tobacco-Specific Nitrosamines inDocument8 pagesComparison of The Content of Tobacco Alkaloids and Tobacco-Specific Nitrosamines inFundación Ellen Riegner de CasasNo ratings yet
- Empowerment and Participation: Bridging The Gap Between Understanding and PracticeDocument10 pagesEmpowerment and Participation: Bridging The Gap Between Understanding and PracticeFundación Ellen Riegner de CasasNo ratings yet
- Ublic Articipation Uidelines: Department of Parks and Recreation City of Raleigh January 2010Document57 pagesUblic Articipation Uidelines: Department of Parks and Recreation City of Raleigh January 2010Fundación Ellen Riegner de CasasNo ratings yet
- Assessing The Impacts of Public Participation: Concepts, Evidence and Policy ImplicationsDocument52 pagesAssessing The Impacts of Public Participation: Concepts, Evidence and Policy ImplicationsFundación Ellen Riegner de CasasNo ratings yet
- Patients Participate Position PaperDocument9 pagesPatients Participate Position PaperFundación Ellen Riegner de CasasNo ratings yet
- Europta ReportDocument186 pagesEuropta ReportFundación Ellen Riegner de CasasNo ratings yet
- Citizen Participation World BankDocument117 pagesCitizen Participation World BankFundación Ellen Riegner de CasasNo ratings yet
- Imra HandbookDocument84 pagesImra HandbookFundación Ellen Riegner de CasasNo ratings yet
- Patients Participate: Case StudiesDocument7 pagesPatients Participate: Case StudiesFundación Ellen Riegner de CasasNo ratings yet
- Effects of Flavoring Compounds Used in ElectronicDocument22 pagesEffects of Flavoring Compounds Used in ElectronicFundación Ellen Riegner de CasasNo ratings yet
- IQOS Point-Of-Sale Marketing Strategies in IsraelDocument4 pagesIQOS Point-Of-Sale Marketing Strategies in IsraelFundación Ellen Riegner de CasasNo ratings yet
- Put Your Money Where Your Butt Is: Policy Research Working Paper 4985Document34 pagesPut Your Money Where Your Butt Is: Policy Research Working Paper 4985Fundación Ellen Riegner de CasasNo ratings yet
- New Limitation Change: UnclassifiedDocument506 pagesNew Limitation Change: UnclassifiedalainNo ratings yet
- Narratives of Debt SPEAKERS Program ScheduleDocument2 pagesNarratives of Debt SPEAKERS Program ScheduleAnonymous arCJEXHNGNo ratings yet
- Bba IiiDocument81 pagesBba IiiSajai SureshNo ratings yet
- The Global Trade and Investment EnvironmentDocument84 pagesThe Global Trade and Investment EnvironmentMa. Patricia Lainne TorresNo ratings yet
- Open Hole Wireline LoggingDocument32 pagesOpen Hole Wireline Loggingsanjeet giriNo ratings yet
- Lesson 8-BridgesDocument2 pagesLesson 8-BridgesMohamed MraouiNo ratings yet
- Properties of Laplace Transform - ROCDocument5 pagesProperties of Laplace Transform - ROCrachit guptaNo ratings yet
- Energy Balance: Technological Institute of The PhilippinesDocument56 pagesEnergy Balance: Technological Institute of The Philippineshenriel tambioNo ratings yet
- Datacard150i ManualDocument2 pagesDatacard150i Manualb00sey0% (1)
- Project Estmate (Final)Document65 pagesProject Estmate (Final)Bilal Ahmed BarbhuiyaNo ratings yet
- Sahaj AePs - Retailer ModuleDocument21 pagesSahaj AePs - Retailer Modulemonishmansoori72No ratings yet
- Legal System KuwaitDocument9 pagesLegal System KuwaitAhmed MareeNo ratings yet
- The Operations FunctionDocument35 pagesThe Operations FunctionrajNo ratings yet
- Hot Mix Asphalt: Section 1: IdentificationDocument11 pagesHot Mix Asphalt: Section 1: Identificationfathul syaafNo ratings yet
- Analisis Proses Quality Control Pada Produksi Cylinder Comp Di PT.XDocument8 pagesAnalisis Proses Quality Control Pada Produksi Cylinder Comp Di PT.XAyu AnsyariNo ratings yet
- Performance RubricsDocument2 pagesPerformance RubricsMaria Manoa GantalaNo ratings yet
- Laptops and Desktop-MAY PRICE 2011Document8 pagesLaptops and Desktop-MAY PRICE 2011Innocent StrangerNo ratings yet
- (Martian) : Smith 1Document9 pages(Martian) : Smith 1api-340110801No ratings yet
- CostcoDocument96 pagesCostcoChris DavidsonNo ratings yet
- M.tech Structural Engineering Syllabus 2nd SemesterDocument5 pagesM.tech Structural Engineering Syllabus 2nd SemesterPriyankaNo ratings yet
- Bill Presentment Architecture in Oracle ReceivablesDocument42 pagesBill Presentment Architecture in Oracle Receivablessrees_15No ratings yet
- Multimedia Project Team RolesDocument16 pagesMultimedia Project Team RolesrinaNo ratings yet
- Maxi Driver ManualDocument50 pagesMaxi Driver Manualpp3665No ratings yet
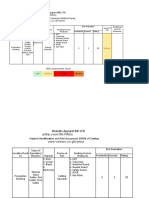
- Brandix Apparel BD LTD: Hazard Identification and Risk Assesment (HIRA) of SwingDocument3 pagesBrandix Apparel BD LTD: Hazard Identification and Risk Assesment (HIRA) of SwingShoaibNo ratings yet
- TW LifecycleDocument7 pagesTW LifecycleSiddhi PisalNo ratings yet
- Material Safety Data Sheet: 1 Chemical Product and Company Identification FENOL LFR (6015-6020-6025-6035)Document5 pagesMaterial Safety Data Sheet: 1 Chemical Product and Company Identification FENOL LFR (6015-6020-6025-6035)Zirve PolimerNo ratings yet
- ERP Implementation: Assignment No 1 By: Syed Hasan Ali Shah 02-111162-213 Bba 8Document5 pagesERP Implementation: Assignment No 1 By: Syed Hasan Ali Shah 02-111162-213 Bba 8Abdur-Rehman QureshiNo ratings yet
- 15MIS0027@DIGI1Document3 pages15MIS0027@DIGI1poojithaaalamNo ratings yet