You might also like
- A Modified Hodgkin-Huxley Model To Show The Effect PDFDocument23 pagesA Modified Hodgkin-Huxley Model To Show The Effect PDFjeforand123No ratings yet
- safetyaspect in tDCS in patient and healthy subjectsDocument7 pagessafetyaspect in tDCS in patient and healthy subjectslabsoneducationNo ratings yet
- 2015 Article 938Document8 pages2015 Article 938aladim lamieraNo ratings yet
- 2010 Article 198Document6 pages2010 Article 198Tejo PramonoNo ratings yet
- efficassy and safety of tDCSDocument2 pagesefficassy and safety of tDCSlabsoneducationNo ratings yet
- Medicina 58 01332Document27 pagesMedicina 58 01332Putu DeaNo ratings yet
- NIH Public Access: Author ManuscriptDocument12 pagesNIH Public Access: Author ManuscriptcasNo ratings yet
- Tms 6Document11 pagesTms 6Ghea SugihartiNo ratings yet
- AppendicesDocument14 pagesAppendicesAmmar suudNo ratings yet
- Katayama 98Document14 pagesKatayama 98moiNo ratings yet
- Transcutaneous Electric Nerve Stimulation Therapy in Temporomandibular Disorders - A Systematic ReviewDocument8 pagesTranscutaneous Electric Nerve Stimulation Therapy in Temporomandibular Disorders - A Systematic ReviewIJAR JOURNALNo ratings yet
- Improving Working Memory Exploring The Effect of Transcranial RandomDocument6 pagesImproving Working Memory Exploring The Effect of Transcranial RandomDanish MujibNo ratings yet
- Transcranial Direct Current Stimulation As A Potential Tool For Cognitive Rehabilitation On Alzheimer's DiseaseDocument2 pagesTranscranial Direct Current Stimulation As A Potential Tool For Cognitive Rehabilitation On Alzheimer's DiseaseyayangNo ratings yet
- HHS Public AccessDocument16 pagesHHS Public AccessM C B ESPAÇO TERAPÊUTICO LTDA AUTISMO EM GOIÂNIANo ratings yet
- Transcranial Magnetic Stimulation of The Brain .7Document14 pagesTranscranial Magnetic Stimulation of The Brain .7novianastasia100% (1)
- Transcutaneous Electrical Nerve Stimulation and Transcutaneous Spinal Electroanalgesia: A Preliminary Efficacy and Mechanisms-Based InvestigationDocument7 pagesTranscutaneous Electrical Nerve Stimulation and Transcutaneous Spinal Electroanalgesia: A Preliminary Efficacy and Mechanisms-Based InvestigationAdam ForshawNo ratings yet
- Abstracts / Brain Stimulation 10 (2017) 346 E540 396Document1 pageAbstracts / Brain Stimulation 10 (2017) 346 E540 396Aleja ToPaNo ratings yet
- tDCS in pediatric hemiparesisDocument1 pagetDCS in pediatric hemiparesislabsoneducationNo ratings yet
- Artigo Algologia EADocument10 pagesArtigo Algologia EAThamires BritoNo ratings yet
- The Spatial Representation of Time in Visual CortexDocument1 pageThe Spatial Representation of Time in Visual CortexRoque Lazcano VázquezNo ratings yet
- 2802 FullDocument9 pages2802 FullNatalia NuñezNo ratings yet
- enhancement of cortical excitanbility and ll motor function in troke patient by tDCSDocument6 pagesenhancement of cortical excitanbility and ll motor function in troke patient by tDCSlabsoneducationNo ratings yet
- Monte Silva2010Document6 pagesMonte Silva2010GUSTAVO CARIBÉNo ratings yet
- 1 s2.0 S138824571500231X MainDocument8 pages1 s2.0 S138824571500231X MainTianyi ZhengNo ratings yet
- Effects of Repeated Anodal TDCS Coupled With Cognitive Training For Patients With Severe Traumatic Brain Injury: A Pilot Randomized Controlled TrialDocument10 pagesEffects of Repeated Anodal TDCS Coupled With Cognitive Training For Patients With Severe Traumatic Brain Injury: A Pilot Randomized Controlled TrialAmandaNo ratings yet
- A Randomized Controlled Study of Segment PDFDocument7 pagesA Randomized Controlled Study of Segment PDFFauzan IndraNo ratings yet
- EJHM - Volume 84 - Issue 1 - Pages 1801-1809-2Document9 pagesEJHM - Volume 84 - Issue 1 - Pages 1801-1809-2Diego Eduardo HurtadoNo ratings yet
- Default Mode Network Mechanisms of Transcranial MagneticDocument20 pagesDefault Mode Network Mechanisms of Transcranial MagneticEdrin VicenteNo ratings yet
- Myofascial Trigger Points and Sensitization: An Updated Pain Model For Tension-Type HeadacheDocument11 pagesMyofascial Trigger Points and Sensitization: An Updated Pain Model For Tension-Type Headacheannisa edwarNo ratings yet
- MJCU - Volume 88 - Issue September - Pages 1601-1614Document9 pagesMJCU - Volume 88 - Issue September - Pages 1601-1614fomoNo ratings yet
- Palm 2016Document14 pagesPalm 2016Bruno KudekenNo ratings yet
- Cagnie2013 Physiological Effects of Dry NeedlingDocument8 pagesCagnie2013 Physiological Effects of Dry NeedlingWahyu FathurrachmanNo ratings yet
- Transcranial Magnetic Stimulation: Juan Jose Lo Pez-Ibor, Marı A Ine S Lo Pez-Ibor and Jose Ignacio PastranaDocument7 pagesTranscranial Magnetic Stimulation: Juan Jose Lo Pez-Ibor, Marı A Ine S Lo Pez-Ibor and Jose Ignacio PastranaJ Ignacio PastranaNo ratings yet
- Research ArticleDocument13 pagesResearch ArticleAnonymous dHL9hx6uUJNo ratings yet
- Mirror TherapyDocument10 pagesMirror TherapyStevani BasryNo ratings yet
- Stagg 2011Document5 pagesStagg 2011Cpeti CzingraberNo ratings yet
- Accepted Manuscript: 10.1016/j.ijosm.2016.05.003Document25 pagesAccepted Manuscript: 10.1016/j.ijosm.2016.05.003yoverNo ratings yet
- 10 1016@j Jpain 2009 04 017Document9 pages10 1016@j Jpain 2009 04 017Carlos Martín De RosasNo ratings yet
- Hypothalamus and Amygdala Response To Acupuncture StimuliDocument13 pagesHypothalamus and Amygdala Response To Acupuncture StimuliAnibal CisternasNo ratings yet
- Motor Cortex Stimulation For Central and Peripheral Deafferentation PainDocument6 pagesMotor Cortex Stimulation For Central and Peripheral Deafferentation PainmoiNo ratings yet
- Velasco 2008Document9 pagesVelasco 2008moiNo ratings yet
- Psychology of Sport & Exercise: Full Length ArticleDocument9 pagesPsychology of Sport & Exercise: Full Length ArticleShyamali Kaushalya FernandoNo ratings yet
- Tens PDFDocument62 pagesTens PDFJay Muhammad100% (1)
- Stress-Induced Pain and Muscle Activity in Patients With Migraine and Tension-Type HeadacheDocument10 pagesStress-Induced Pain and Muscle Activity in Patients With Migraine and Tension-Type HeadacheRicky HerdiantoNo ratings yet
- Peripheral and Central Adaptations After A Median Nerve Neuromobilization Program Completed by Individuals With Carpal Tunnel SyndromeDocument13 pagesPeripheral and Central Adaptations After A Median Nerve Neuromobilization Program Completed by Individuals With Carpal Tunnel SyndromeRafael MoreiraNo ratings yet
- Cognitive Enhancement - StimulationDocument2 pagesCognitive Enhancement - StimulationSwathi KartikNo ratings yet
- Mechanisms of TENSDocument13 pagesMechanisms of TENSOana Budugan0% (1)
- Research Article: Neuroprotective Effects of Cistanches Herba Therapy On Patients With Moderate Alzheimer's DiseaseDocument13 pagesResearch Article: Neuroprotective Effects of Cistanches Herba Therapy On Patients With Moderate Alzheimer's DiseaseVeronica Yosita AnandaNo ratings yet
- Pain Theories PDFDocument7 pagesPain Theories PDFAndreea-Alexandra LupuNo ratings yet
- Therapeutic Rewiring by Means of Desynchronizing Brain StimulationDocument9 pagesTherapeutic Rewiring by Means of Desynchronizing Brain StimulationGiovi CastilloNo ratings yet
- Ef Ficacy of Transcutaneous Electrical Nerve Stimulation in People With Pain After Spinal Cord Injury: A Meta-AnalysisDocument7 pagesEf Ficacy of Transcutaneous Electrical Nerve Stimulation in People With Pain After Spinal Cord Injury: A Meta-Analysisxian karachiNo ratings yet
- Melatonina e EndometrioseDocument8 pagesMelatonina e EndometrioseFatima VieiraNo ratings yet
- The Effect of Trigger Point Management by Positional Release Therapy On Tension Type HeadacheDocument7 pagesThe Effect of Trigger Point Management by Positional Release Therapy On Tension Type Headachejohn gibbonsNo ratings yet
- Transcutaneous Electrical Nerve Stimulation Basic ScienceDocument13 pagesTranscutaneous Electrical Nerve Stimulation Basic ScienceMuhammad FahmyNo ratings yet
- 1 s2.0 S0165032721002445 MainDocument10 pages1 s2.0 S0165032721002445 MainAnonymous kvI7zBNNo ratings yet
- TENS Literature - Review - and - Meta - Analysis - Of.99266Document9 pagesTENS Literature - Review - and - Meta - Analysis - Of.99266Adam ForshawNo ratings yet
- 3.BTL-6000 Super Inductive System STUDY Repetitive Peripheral Inductive Stimulation in Musculoskeletal Pain Management EN100 PreviewDocument6 pages3.BTL-6000 Super Inductive System STUDY Repetitive Peripheral Inductive Stimulation in Musculoskeletal Pain Management EN100 Previewf.mariajdbNo ratings yet
- A Review of Brain Stimulation Methods To Treat SubstanceDocument21 pagesA Review of Brain Stimulation Methods To Treat SubstancearturohcuervoNo ratings yet
- 1678 7757 Jaos 25 2 0112Document9 pages1678 7757 Jaos 25 2 0112ndul21No ratings yet
- Intralipid infusion for Myelin Sheath Repair in Multiple Sclerosis and Trigeminal Neuralgia?From EverandIntralipid infusion for Myelin Sheath Repair in Multiple Sclerosis and Trigeminal Neuralgia?No ratings yet
- Clinical Neurophysiology of Fatigue: M.J. Zwarts, G. Bleijenberg, B.G.M. Van EngelenDocument9 pagesClinical Neurophysiology of Fatigue: M.J. Zwarts, G. Bleijenberg, B.G.M. Van EngelenShyamali Kaushalya FernandoNo ratings yet
- Boggio 2009Document6 pagesBoggio 2009Shyamali Kaushalya FernandoNo ratings yet
- Exercise-Induced Central Fatigue: A Review of The Literature With Implications For Dance Science ResearchDocument10 pagesExercise-Induced Central Fatigue: A Review of The Literature With Implications For Dance Science ResearchShyamali Kaushalya FernandoNo ratings yet
- Psychology of Sport & Exercise: Full Length ArticleDocument9 pagesPsychology of Sport & Exercise: Full Length ArticleShyamali Kaushalya FernandoNo ratings yet
- Angius 2016 PDFDocument13 pagesAngius 2016 PDFShyamali Kaushalya FernandoNo ratings yet
- Angius SRDocument23 pagesAngius SRShyamali Kaushalya FernandoNo ratings yet
- No significant effect of 15 tDCS protocols on simple motor reaction timeDocument9 pagesNo significant effect of 15 tDCS protocols on simple motor reaction timeShyamali Kaushalya FernandoNo ratings yet
- Angius 2016 PDFDocument13 pagesAngius 2016 PDFShyamali Kaushalya FernandoNo ratings yet
- Abbiss - 2005 - Models To Explain Fatigue Duringprolonged Endurance Cyclin PDFDocument34 pagesAbbiss - 2005 - Models To Explain Fatigue Duringprolonged Endurance Cyclin PDFShyamali Kaushalya FernandoNo ratings yet
- Beck Anxiety Inventory: Historical BackgroundDocument5 pagesBeck Anxiety Inventory: Historical BackgroundShyamali Kaushalya FernandoNo ratings yet
- 4 - Lattari 2018 - Effect of TDCS On Time Limit and Rating of Percevied Excertion in Physically Active WomenDocument15 pages4 - Lattari 2018 - Effect of TDCS On Time Limit and Rating of Percevied Excertion in Physically Active WomenShyamali Kaushalya FernandoNo ratings yet
- 2) Inequality GraphsDocument14 pages2) Inequality Graphsmanobilli30No ratings yet
- MandrakeDocument6 pagesMandrakeEmry Kamahi Tahatai KereruNo ratings yet
- Bangla FoodsDocument6 pagesBangla FoodsSubadrika DarmadewiNo ratings yet
- Ece-Research Work 1Document10 pagesEce-Research Work 1Peale ObiedoNo ratings yet
- Material Cost - EOQDocument16 pagesMaterial Cost - EOQSimranNo ratings yet
- For Student-General Chemistry I - Module 6 - Phan Tai HuanDocument41 pagesFor Student-General Chemistry I - Module 6 - Phan Tai HuanEsat Goceri100% (1)
- Minimizing Penalty in Industrialpower Factor Correction by Engaging Apfc UnitDocument15 pagesMinimizing Penalty in Industrialpower Factor Correction by Engaging Apfc UnitabellNo ratings yet
- To 1 SMPN 210 JKT Tahun 2016-2017Document11 pagesTo 1 SMPN 210 JKT Tahun 2016-2017Sugeng Supoyo Pawit DigdotriratnaNo ratings yet
- Chana Masala Powder RecipeDocument215 pagesChana Masala Powder RecipeTIRUPUR OFFICENo ratings yet
- Namma Kalvi 12th Maths Book Back and Creative Questions em 219383Document185 pagesNamma Kalvi 12th Maths Book Back and Creative Questions em 219383TharaneshNo ratings yet
- Drug Metabolism in Fetus and NewbornsDocument20 pagesDrug Metabolism in Fetus and NewbornsBikash SahNo ratings yet
- 00 - Orientation LessonDocument32 pages00 - Orientation LessonRekha ShahNo ratings yet
- Luftwaffe Night Fighter Control MethodsDocument17 pagesLuftwaffe Night Fighter Control MethodsKIRU SILVIU100% (3)
- Despiece Motor Mono PDFDocument55 pagesDespiece Motor Mono PDFGabriel OyagaNo ratings yet
- Noun Form Answers PDFDocument11 pagesNoun Form Answers PDFChinna LingamNo ratings yet
- Toaz - Info Super Coolant Af Nac PRDocument6 pagesToaz - Info Super Coolant Af Nac PRsugi yantoNo ratings yet
- Astm C1396 C1396M-17Document8 pagesAstm C1396 C1396M-17Stefano CamillucciNo ratings yet
- NCERT Solutions For Class 8 Science Chapter 6Document4 pagesNCERT Solutions For Class 8 Science Chapter 6D Rong saNo ratings yet
- Food DirectoryDocument20 pagesFood Directoryyugam kakaNo ratings yet
- Acoustic Design For Call CenterDocument16 pagesAcoustic Design For Call CenteraliNo ratings yet
- Liugong 938l Wheel Loader Parts ManualDocument20 pagesLiugong 938l Wheel Loader Parts Manualviolet100% (56)
- Mapsco Street GuidesDocument5 pagesMapsco Street Guidesapi-256961360No ratings yet
- Metacut 350: Operating and Instructions ManualDocument20 pagesMetacut 350: Operating and Instructions ManualRohman AzizNo ratings yet
- Life Without GravityDocument2 pagesLife Without GravityRomel Antonio Zorrilla RamirezNo ratings yet
- Building Schedule 050721Document6 pagesBuilding Schedule 050721Parth DaxiniNo ratings yet
- Ms 01 140Document74 pagesMs 01 140Prateek RajNo ratings yet
- Bushings BrochureDocument14 pagesBushings Brochurebpd21No ratings yet
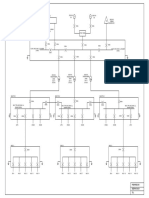
- Conceptual SLDDocument1 pageConceptual SLDakhilNo ratings yet
- MANAURITE XM Material PDFDocument8 pagesMANAURITE XM Material PDFkbc404No ratings yet
- Structural Modelling and Analysis using BIM ToolsDocument137 pagesStructural Modelling and Analysis using BIM ToolsManuel Solís López100% (1)