You might also like
- Second Quarter Examination in Precalculus Reviewer PDFDocument6 pagesSecond Quarter Examination in Precalculus Reviewer PDFmarie parfan100% (3)
- Clinical Management Review 2023-2024: Volume 2: USMLE Step 3 and COMLEX-USA Level 3From EverandClinical Management Review 2023-2024: Volume 2: USMLE Step 3 and COMLEX-USA Level 3No ratings yet
- MYMT PersonalBudgetWorksheet TrackingWeeklyExpenses Final Version 1 Jan 2004Document7 pagesMYMT PersonalBudgetWorksheet TrackingWeeklyExpenses Final Version 1 Jan 2004gopi100% (2)
- Cocolife HealthCare Schemes & Medical BenefitsDocument7 pagesCocolife HealthCare Schemes & Medical BenefitsMaribel Bonite Peneyra0% (1)
- Quality Assurance Management I To 12Document435 pagesQuality Assurance Management I To 12yesrhNo ratings yet
- 11 Interim Guide in The MGT of Covid19 PDFDocument1 page11 Interim Guide in The MGT of Covid19 PDFDenz Marc Ray AleaNo ratings yet
- Workplace Handbook ReportDocument96 pagesWorkplace Handbook ReportKimm Delos ReyesNo ratings yet
- Dentistry Emergency Management During CovidDocument44 pagesDentistry Emergency Management During CovidDewi Caronita GurusingaNo ratings yet
- Adult Presurgical COVID-19 QuestionnaireDocument1 pageAdult Presurgical COVID-19 QuestionnairegaucheNo ratings yet
- SAFETY OFFICERS LINK MEETING - COVID 19 Prevention at The Workplace PDFDocument48 pagesSAFETY OFFICERS LINK MEETING - COVID 19 Prevention at The Workplace PDFJoanne De JoyaNo ratings yet
- Alert Level 1 Guidelines: Draft As of 27 February 2022Document21 pagesAlert Level 1 Guidelines: Draft As of 27 February 2022Joseph GutierrezNo ratings yet
- PADPH Dental Clinical Protocol Recommendations During The COVID-19 Pandemic - Aug162021Document22 pagesPADPH Dental Clinical Protocol Recommendations During The COVID-19 Pandemic - Aug162021RA RosanesNo ratings yet
- KEAMANAN PRAKTEK ERA PANDEMI, Ari UIDocument37 pagesKEAMANAN PRAKTEK ERA PANDEMI, Ari UIlidya kurniawanNo ratings yet
- PCH PATIENT-Br - DIGITALDocument8 pagesPCH PATIENT-Br - DIGITALRoberto MejiaNo ratings yet
- Appendix 1 PDFDocument1 pageAppendix 1 PDFPJNo ratings yet
- Screening QuestionsDocument1 pageScreening QuestionsPJNo ratings yet
- Special Needs Treatment Plan Audrey Noonan I. Assessment: o o o o o oDocument7 pagesSpecial Needs Treatment Plan Audrey Noonan I. Assessment: o o o o o oapi-663723303No ratings yet
- Treatment and Care of Peripheral Intravenous Extravasations 2016Document5 pagesTreatment and Care of Peripheral Intravenous Extravasations 2016Thắng NguyễnNo ratings yet
- dh2 Treatment PlanningDocument5 pagesdh2 Treatment Planningapi-663741201No ratings yet
- Covid 19 GuidelinesDocument4 pagesCovid 19 GuidelinesMelissa DavidNo ratings yet
- Band 2Document132 pagesBand 2javed javedNo ratings yet
- HealthsafetyDocument32 pagesHealthsafetyapi-346614972No ratings yet
- Covid-19 Management: FAQs by HCWsDocument31 pagesCovid-19 Management: FAQs by HCWsKabirNo ratings yet
- COVID Ready ReckonerDocument10 pagesCOVID Ready ReckonerSanNo ratings yet
- Annex A.1 Recommended Algorithm For Referral and Admission in The Community Isolation UnitDocument1 pageAnnex A.1 Recommended Algorithm For Referral and Admission in The Community Isolation UnitIsrael H. ZantuaNo ratings yet
- Post-COVID-19 Clinical and Management Guidelines For Orthodontic PracticesDocument15 pagesPost-COVID-19 Clinical and Management Guidelines For Orthodontic Practicesdrdentist1981No ratings yet
- Coronavirus (Covid-19) Pre-Screening Questionnaire - Must Be Completed Prior To RegistrationDocument1 pageCoronavirus (Covid-19) Pre-Screening Questionnaire - Must Be Completed Prior To RegistrationJokerul69No ratings yet
- 1 Endodontic EmergencyDocument106 pages1 Endodontic EmergencyAME DENTAL COLLEGE RAICHUR, KARNATAKANo ratings yet
- More Information: Help Stop The Spread of Covid-19Document2 pagesMore Information: Help Stop The Spread of Covid-19timgourNo ratings yet
- Health Assessment Algorithm For Sinovac: YES NODocument1 pageHealth Assessment Algorithm For Sinovac: YES NOKim GomezNo ratings yet
- COVID-19 Advisory - 04072021Document9 pagesCOVID-19 Advisory - 04072021Ryan S. AngelesNo ratings yet
- COVID-19 ER Clinical Pathway: Registration or Triage NurseDocument2 pagesCOVID-19 ER Clinical Pathway: Registration or Triage NurseBassam AlqadasiNo ratings yet
- Cleft Lip and Palate: MethodologyDocument25 pagesCleft Lip and Palate: MethodologyTahani AlmagrhiNo ratings yet
- Update Who Recommendation On Covid-19 For Hospital: Setiawan Jati Laksono 10 April 2020Document34 pagesUpdate Who Recommendation On Covid-19 For Hospital: Setiawan Jati Laksono 10 April 2020Nadya FaradibaNo ratings yet
- Impact of COVID 19 On Dentistry - by Group 9 HSDocument41 pagesImpact of COVID 19 On Dentistry - by Group 9 HSmilahelan999No ratings yet
- Beaumont VisitationDocument2 pagesBeaumont VisitationWXYZ-TV Channel 7 DetroitNo ratings yet
- BDC Guidelines of The New Norm During PandemicDocument18 pagesBDC Guidelines of The New Norm During PandemicJoshua Christian TeopengcoNo ratings yet
- Visitation Information 20200605Document2 pagesVisitation Information 20200605WDIV/ClickOnDetroitNo ratings yet
- Easing RAC Visitor Restrictions 22092020 PDFDocument1 pageEasing RAC Visitor Restrictions 22092020 PDFRichardNo ratings yet
- Havlicek DietaDocument1 pageHavlicek Dietaxxx.juliettaNo ratings yet
- People Who Are at High Risk For Severe Illness From Covid-19Document2 pagesPeople Who Are at High Risk For Severe Illness From Covid-19super_sumoNo ratings yet
- DR Deborah Birx Guidelines For Opening Up America AgainDocument20 pagesDR Deborah Birx Guidelines For Opening Up America AgainJohn EssNo ratings yet
- COVID-19 Guidelines For Film and Video - A Summary For Small Crews and Low-Budget ProductionsDocument29 pagesCOVID-19 Guidelines For Film and Video - A Summary For Small Crews and Low-Budget ProductionsJoel SouzaNo ratings yet
- Isolation Guide enDocument24 pagesIsolation Guide enbasil aliNo ratings yet
- مناقشة 8 فبراير 2022Document5 pagesمناقشة 8 فبراير 2022mustafa muhamedNo ratings yet
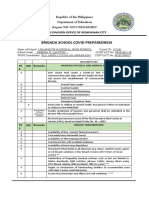
- Brigada School Covid Preparedness: Schools Division Office of Kidapawan CityDocument3 pagesBrigada School Covid Preparedness: Schools Division Office of Kidapawan CityLiezel RollonNo ratings yet
- TD Enterprise Health Screening Form enDocument2 pagesTD Enterprise Health Screening Form enKevin JayNo ratings yet
- Referral Flow Covid City HealthDocument1 pageReferral Flow Covid City HealthJohnPaulOliverosNo ratings yet
- 18 05 2021 MucormycosisDocument1 page18 05 2021 MucormycosisPartho MukherjeeNo ratings yet
- Community Primary Care COVID 19 AlgorithmDocument2 pagesCommunity Primary Care COVID 19 Algorithmsiyakesar4567No ratings yet
- Comprehensive Hec Policy/Guidelines For Universities and Dais On Covid-19Document13 pagesComprehensive Hec Policy/Guidelines For Universities and Dais On Covid-19Malik MoeezNo ratings yet
- Effectiveness of Periodontal Therapy in Patients With Drug-Induced Gingival Overgrowth. Long-Term ResultsDocument6 pagesEffectiveness of Periodontal Therapy in Patients With Drug-Induced Gingival Overgrowth. Long-Term ResultsAna OrtizNo ratings yet
- Travel: Please Consider Before Entering This Building OR WorkplaceDocument1 pageTravel: Please Consider Before Entering This Building OR Workplacevimalraj vtNo ratings yet
- Diagnosis and Treatment Planning in RPDDocument116 pagesDiagnosis and Treatment Planning in RPDvadlamudi chakradharNo ratings yet
- Dental Settings: Key ConceptsDocument7 pagesDental Settings: Key ConceptsVigneshvar SreekanthNo ratings yet
- Transmission 1: COVID-19 Spreads Primarily Through Contact With An Transmission 2: COVID-19 Also Spreads When A Person Touches ADocument7 pagesTransmission 1: COVID-19 Spreads Primarily Through Contact With An Transmission 2: COVID-19 Also Spreads When A Person Touches AShahadat HossainNo ratings yet
- Flow For Visitors Eng Sxxuf6Document1 pageFlow For Visitors Eng Sxxuf6James ChoongNo ratings yet
- May 14 Guidelines For Preoperative COVID19 Testing For Elective Cancer SurgeryDocument2 pagesMay 14 Guidelines For Preoperative COVID19 Testing For Elective Cancer Surgeryarjumardi azrahNo ratings yet
- Eng 2116 - Doc Redesign ProgramDocument2 pagesEng 2116 - Doc Redesign Programapi-288266811No ratings yet
- Special Needs TX PlanDocument6 pagesSpecial Needs TX Planapi-662638224No ratings yet
- Management of Acute Dental Problems During Covid 19Document11 pagesManagement of Acute Dental Problems During Covid 19Faiqotul KumalaNo ratings yet
- Recommendations For Completing A Home Visit During COVID-19 PandemicDocument4 pagesRecommendations For Completing A Home Visit During COVID-19 PandemicMaCristyJoneferRevamonteNo ratings yet
- Pre and Post Op Care of Cataract in MCHDocument4 pagesPre and Post Op Care of Cataract in MCHAthira PSNo ratings yet
- Good Health in the Tropics: Advice to Travellers and SettlersFrom EverandGood Health in the Tropics: Advice to Travellers and SettlersNo ratings yet
- Philosophical Perspective of The Self Understanding The SelfDocument16 pagesPhilosophical Perspective of The Self Understanding The Selfmarie parfanNo ratings yet
- Employment and Career Opportunities of A DentistDocument8 pagesEmployment and Career Opportunities of A Dentistmarie parfanNo ratings yet
- Emotional Intelligence: 3 Strategies To Improve EIDocument6 pagesEmotional Intelligence: 3 Strategies To Improve EImarie parfanNo ratings yet
- Spiritual Self: Will. Intelligence and AbilitiesDocument1 pageSpiritual Self: Will. Intelligence and Abilitiesmarie parfanNo ratings yet
- 4TH QTR Reviewer IotDocument1 page4TH QTR Reviewer Iotmarie parfanNo ratings yet
- 4TH QTR Reviewer GchemDocument6 pages4TH QTR Reviewer Gchemmarie parfanNo ratings yet
- 5b CorporateAttiresDocument119 pages5b CorporateAttiresmarie parfanNo ratings yet
- Wisdom) Physics) : PHILOSOPHY Philos+sophia (Love of METAPHYSICS Meta+physika (BeyondDocument2 pagesWisdom) Physics) : PHILOSOPHY Philos+sophia (Love of METAPHYSICS Meta+physika (Beyondmarie parfanNo ratings yet
- Oral Communication Mid Terms Reviewer 1Document7 pagesOral Communication Mid Terms Reviewer 1marie parfanNo ratings yet
- Reaction Paper: IssueDocument2 pagesReaction Paper: Issuemarie parfanNo ratings yet
- "Knowing Oneself": "How Well Do I Know Myself?"Document20 pages"Knowing Oneself": "How Well Do I Know Myself?"marie parfanNo ratings yet
- Circulatory System: Science ReviewerDocument5 pagesCirculatory System: Science Reviewermarie parfanNo ratings yet
- General Biology Reviewer (2: I. PLANT BIOLOGY: Anatomy and PhysiologyDocument12 pagesGeneral Biology Reviewer (2: I. PLANT BIOLOGY: Anatomy and Physiologymarie parfanNo ratings yet
- Science 1st Quarter MT ReviewerDocument2 pagesScience 1st Quarter MT Reviewermarie parfanNo ratings yet
- Required Start-Up Capital: Investments AmountsDocument2 pagesRequired Start-Up Capital: Investments Amountsmarie parfanNo ratings yet
- Investments Amount PHP 8,873,050.00: Members: Comilang, Chan, Fuenzalida, Perez & Sampaga Section: SE124Document2 pagesInvestments Amount PHP 8,873,050.00: Members: Comilang, Chan, Fuenzalida, Perez & Sampaga Section: SE124marie parfanNo ratings yet
- Reviewer in Empowerment TechnologyDocument2 pagesReviewer in Empowerment Technologymarie parfanNo ratings yet
- Business CycleDocument22 pagesBusiness Cyclemarie parfanNo ratings yet
- Rivera M3 - Lesson 1 - CiaDocument8 pagesRivera M3 - Lesson 1 - Ciamarie parfanNo ratings yet
- 3 The Spiritual SelfDocument42 pages3 The Spiritual Selfmarie parfanNo ratings yet
- Ex 7 Heat Effects PDFDocument21 pagesEx 7 Heat Effects PDFmarie parfanNo ratings yet
- International Education For Action Research: The Bamenda ModelDocument13 pagesInternational Education For Action Research: The Bamenda ModelIan Hughes100% (1)
- Feminism and RapeDocument16 pagesFeminism and RapeRenataKedavraNo ratings yet
- Mens Health 15 Minute Training Guide Issue 2016 PreviewDocument5 pagesMens Health 15 Minute Training Guide Issue 2016 PreviewHelton Azevedo0% (1)
- Why Facts Don T Change Our MindsDocument9 pagesWhy Facts Don T Change Our MindsGeorge Herbert Mody100% (1)
- Emergency Action AND Fire Prevention Plan: Sample Written Safety Program ForDocument6 pagesEmergency Action AND Fire Prevention Plan: Sample Written Safety Program ForVinod ChaudhariNo ratings yet
- Stock Opname Apotek Tanggal 01 April 2023Document6 pagesStock Opname Apotek Tanggal 01 April 2023vinisr48No ratings yet
- Chapter 12 - Congenital and Acquired ImmunodeficienciesDocument11 pagesChapter 12 - Congenital and Acquired ImmunodeficienciesFYMNo ratings yet
- Chapter 10 - Contract Catering (Non-Crl) : Sponsor - DIODocument8 pagesChapter 10 - Contract Catering (Non-Crl) : Sponsor - DIOCANDYNo ratings yet
- Guide To Implementing Iso 22000Document34 pagesGuide To Implementing Iso 22000getaneh abebeNo ratings yet
- Bio-Psycho-Social Formulation and Differential Diagnosis: Psychiatric Assessment With Helen M. Farrell, M.DDocument12 pagesBio-Psycho-Social Formulation and Differential Diagnosis: Psychiatric Assessment With Helen M. Farrell, M.DJ.C. GarzaNo ratings yet
- 14 Water BangladeshDocument14 pages14 Water BangladeshA S M Hefzul KabirNo ratings yet
- ICT & Ageing: European Study On Users, Markets and TechnologiesDocument45 pagesICT & Ageing: European Study On Users, Markets and TechnologiesBart ColletNo ratings yet
- 4ndzvyovxipmju1rfmhykayfDocument3 pages4ndzvyovxipmju1rfmhykayfKunal GuptaNo ratings yet
- Ou Must Score 60 Marks Out of 100 To Pass The ExaminationDocument6 pagesOu Must Score 60 Marks Out of 100 To Pass The ExaminationRajeshKannan VeluchamyNo ratings yet
- "Cloud Castle" 2.0Document2 pages"Cloud Castle" 2.0Spencer PelejoNo ratings yet
- Tpbo Paper 1Document71 pagesTpbo Paper 1RaghuNo ratings yet
- MH096Document3 pagesMH096Rocío CPérezNo ratings yet
- Diversity InclusionDocument20 pagesDiversity InclusionMarco Ramirez100% (2)
- Kami Export - Ava Cortis - Anna Garcia Autopsy ReportDocument3 pagesKami Export - Ava Cortis - Anna Garcia Autopsy ReportagcortisNo ratings yet
- Eguide: Contamination Control in Pharmaceutical IndustryDocument17 pagesEguide: Contamination Control in Pharmaceutical Industrygsv988No ratings yet
- Sample of QuestionsDocument16 pagesSample of QuestionsAhmed Kh. Abu WardaNo ratings yet
- Mobile Elevating Work PlatformsDocument13 pagesMobile Elevating Work PlatformsRauf HuseynovNo ratings yet
- S1 Guidelines "Lumbar Puncture and Cerebrospinal Fluid Analysis"Document28 pagesS1 Guidelines "Lumbar Puncture and Cerebrospinal Fluid Analysis"alejandro montesNo ratings yet
- ESPN - Social Investment Synthesis Report (FINAL 210415) - Report CLEANDocument46 pagesESPN - Social Investment Synthesis Report (FINAL 210415) - Report CLEANMarcello D'AmicoNo ratings yet
- Overall ReflectionDocument2 pagesOverall Reflectionapi-508053077No ratings yet
- Salmeh 2020Document6 pagesSalmeh 2020mohammad ali salmehNo ratings yet
- SR Secondary TMA ALL Subject2019 PDFDocument119 pagesSR Secondary TMA ALL Subject2019 PDFRahil ShamsiNo ratings yet
- (3 Metilpentil) AminaDocument10 pages(3 Metilpentil) AminaleonardoNo ratings yet