You might also like
- Complementary and Alternative Medical Lab Testing Part 19: MiscellaneousFrom EverandComplementary and Alternative Medical Lab Testing Part 19: MiscellaneousNo ratings yet
- HhihhygtfrtdgbhjDocument11 pagesHhihhygtfrtdgbhjKania HidayantiNo ratings yet
- Al Ghazawihavbktyhdi36840Document6 pagesAl Ghazawihavbktyhdi36840Siti AnisadyahNo ratings yet
- Glenmark Remo+Teneli MS D1 (17082021)Document13 pagesGlenmark Remo+Teneli MS D1 (17082021)Bhavani KirthiNo ratings yet
- Hyperlipidemia Induced by Triton WR1339 (Tyloxapol) in Wistar RatsDocument3 pagesHyperlipidemia Induced by Triton WR1339 (Tyloxapol) in Wistar RatsdonNo ratings yet
- Nusrat Jahan Mim ID - 1920495 PHA 207 Sec-01 Assignment (THEOPHYLLINE)Document13 pagesNusrat Jahan Mim ID - 1920495 PHA 207 Sec-01 Assignment (THEOPHYLLINE)Mahadi Hasan KhanNo ratings yet
- CP LGZWHRs Q4 KH BGW LQ TQ NFGDocument7 pagesCP LGZWHRs Q4 KH BGW LQ TQ NFGMacarena Beatriz Piña ValenciaNo ratings yet
- Theophyllin + Kontrasepsi OralDocument6 pagesTheophyllin + Kontrasepsi OralNanda apriliantoNo ratings yet
- Detection Times in UrineDocument6 pagesDetection Times in UrineoooopopopNo ratings yet
- K Etorolac Tormethamine PDFDocument19 pagesK Etorolac Tormethamine PDFMuhammad Khairun NNo ratings yet
- Pharmacokinetic Interaction Between Fluoxetine and Omeprazole in Healthy Male Volunteers: A Prospective Pilot StudyDocument9 pagesPharmacokinetic Interaction Between Fluoxetine and Omeprazole in Healthy Male Volunteers: A Prospective Pilot StudyCurcubeuAuroraNo ratings yet
- Smith - S Anesthesia For Infants and Children (Eighth Edition) 2011-384-391Document8 pagesSmith - S Anesthesia For Infants and Children (Eighth Edition) 2011-384-391Alexiel BathoryNo ratings yet
- A New Approach To The Prophylaxis of Cyclic Vomiting TopiramateDocument5 pagesA New Approach To The Prophylaxis of Cyclic Vomiting TopiramateVianNo ratings yet
- Pharmacokinetics of High-Dose Oral Thiamine Hydrochloride in Healthy SubjectsDocument10 pagesPharmacokinetics of High-Dose Oral Thiamine Hydrochloride in Healthy SubjectsHerawati YustikasariNo ratings yet
- Other Antiemetic Medications: Other 5HT3 Receptor AntagonistsDocument4 pagesOther Antiemetic Medications: Other 5HT3 Receptor AntagonistsYayaNo ratings yet
- Ritalin ADocument8 pagesRitalin ALeonardo David Dearo SimonettiNo ratings yet
- 2014 PR 31 1676 1688 Ugt2bDocument13 pages2014 PR 31 1676 1688 Ugt2bSCYoungNo ratings yet
- 223 2012 Article 9639Document10 pages223 2012 Article 9639Daniela CerianiNo ratings yet
- Eli GardDocument7 pagesEli GardthanaNo ratings yet
- Therapeutic Drug Monitoring Part 2 PDFDocument23 pagesTherapeutic Drug Monitoring Part 2 PDFChandra AvicennaNo ratings yet
- Pomegranate Juice HealingDocument23 pagesPomegranate Juice HealingKingNo ratings yet
- Baltes 2001Document9 pagesBaltes 2001Brahma Hakim Yuanda HutabaratNo ratings yet
- 29 1355 PDFDocument5 pages29 1355 PDFLuthfiAdjiePermanaNo ratings yet
- PredictingAllopurinolResponse in Patient With Gout 2015Document13 pagesPredictingAllopurinolResponse in Patient With Gout 2015นันทสิทธิ์ ศิริวิชญ์ไมตรีNo ratings yet
- JurnalDocument5 pagesJurnalkadekNo ratings yet
- VanmeyelDocument5 pagesVanmeyelGanda SilitongaNo ratings yet
- Pharmacology, Biochemistry and BehaviorDocument5 pagesPharmacology, Biochemistry and BehaviorJames PerianayagamNo ratings yet
- Harnal OCAS PI NCDS02 SI Approved 29aug14Document11 pagesHarnal OCAS PI NCDS02 SI Approved 29aug14Teja KusumaNo ratings yet
- Vivo Selectivity For The Bladder Over The Salivary Glands Compared WithDocument13 pagesVivo Selectivity For The Bladder Over The Salivary Glands Compared WithDwi Amalia husnaNo ratings yet
- Experimental Investigations: Original ArticlesDocument8 pagesExperimental Investigations: Original ArticlesAmina HAMMOUTENENo ratings yet
- Theophylline by DP 307 936,933,946,956Document10 pagesTheophylline by DP 307 936,933,946,956Muhammad AbdullahNo ratings yet
- CumulativeReleaseofadrug PDFDocument4 pagesCumulativeReleaseofadrug PDFkumar purushotamNo ratings yet
- Pengaruh Makanan Pada CaptoprilDocument5 pagesPengaruh Makanan Pada CaptoprilNiluh putu Satria maharaniNo ratings yet
- Bioequivalence Studyof Duloxetine HCL 60 MG Capsulesin HealthyDocument6 pagesBioequivalence Studyof Duloxetine HCL 60 MG Capsulesin HealthyMohamed Medhat AliNo ratings yet
- Efficacy and Tolerability of Tamsulosin 0.4 MG in Patients With Symptomatic Benign Prostatic HyperplasiaDocument6 pagesEfficacy and Tolerability of Tamsulosin 0.4 MG in Patients With Symptomatic Benign Prostatic HyperplasiawanggaNo ratings yet
- AIJPMS - Volume 3 - Issue 1 - Pages 15-31Document17 pagesAIJPMS - Volume 3 - Issue 1 - Pages 15-31Eman MahmoudNo ratings yet
- In A Methotrexate Induced Model of Intestinal Mucositis, Olmesartan Reduced Inflammation and Induced Enteropathy Characterized by Severe Diarrhea, Weight Loss, and Reduced Sucrose ActivityDocument7 pagesIn A Methotrexate Induced Model of Intestinal Mucositis, Olmesartan Reduced Inflammation and Induced Enteropathy Characterized by Severe Diarrhea, Weight Loss, and Reduced Sucrose ActivityMohamed IsmailNo ratings yet
- Single-Dose and Multiple-Dose Pharmacokinetics of Zaltoprofen After Oral Administration in Healthy Chinese VolunteersDocument7 pagesSingle-Dose and Multiple-Dose Pharmacokinetics of Zaltoprofen After Oral Administration in Healthy Chinese VolunteersSonia BaruaNo ratings yet
- Babalik. Serum Drug Concentration Turkey. IJTLD Dec 13Document7 pagesBabalik. Serum Drug Concentration Turkey. IJTLD Dec 13Vigilancia EpidemiologicaNo ratings yet
- Bioequivalence Study of Two Formulations of Bisoprolol Fumarate Tablets in Healthy SubjectsDocument7 pagesBioequivalence Study of Two Formulations of Bisoprolol Fumarate Tablets in Healthy SubjectsSan-Clin-Eq LaboratoryNo ratings yet
- Comparative in Vitro Dissolution and in Vivo Bioequivalence of Two Diclofenac Enteric Coated FormulationsDocument5 pagesComparative in Vitro Dissolution and in Vivo Bioequivalence of Two Diclofenac Enteric Coated FormulationsgeoaislaNo ratings yet
- Aghazadeh, Habashi, 2008 PK MLX in Rats, Influência GastrintestinalDocument6 pagesAghazadeh, Habashi, 2008 PK MLX in Rats, Influência GastrintestinalFlávia ElizabeteNo ratings yet
- Formulation and Evaluation of Floating Tablet of Captopril: Sameer Singh, Kalpana Prajapati, A K Pathak, A MishraDocument9 pagesFormulation and Evaluation of Floating Tablet of Captopril: Sameer Singh, Kalpana Prajapati, A K Pathak, A Mishraamalia shaldaNo ratings yet
- Thioguanine 20 MG - ML Oral Suspension PDFDocument4 pagesThioguanine 20 MG - ML Oral Suspension PDFAlexander MeloNo ratings yet
- Ethanolamines: Product InformationDocument1 pageEthanolamines: Product Informationzubair195No ratings yet
- Excipients Transit IntestinalDocument7 pagesExcipients Transit IntestinalHernando Garay RozoNo ratings yet
- Multiple-Dose Acetaminophen Pharmacokinetics: Ayres"Document6 pagesMultiple-Dose Acetaminophen Pharmacokinetics: Ayres"did youNo ratings yet
- 83 - 206289 Atropine Clinpharm PreaDocument28 pages83 - 206289 Atropine Clinpharm PreaAlishba MushtaqNo ratings yet
- Jobelyn® Ameliorates Anxiety Response and Oxido-Inflammatory Markers Induced by Tramadol Use and Discontinuation in RatsDocument17 pagesJobelyn® Ameliorates Anxiety Response and Oxido-Inflammatory Markers Induced by Tramadol Use and Discontinuation in RatsMediterr J Pharm Pharm SciNo ratings yet
- Salbutamol Drug Study Generic Name: Brand NameDocument4 pagesSalbutamol Drug Study Generic Name: Brand NameLyn ConsingNo ratings yet
- David J. Greenblatt D. (ZOLPIDEM)Document8 pagesDavid J. Greenblatt D. (ZOLPIDEM)Paulina AlonsoNo ratings yet
- Use of Very-High-Dose Olanzapine in Treatment-Resistant SchizophreniaDocument4 pagesUse of Very-High-Dose Olanzapine in Treatment-Resistant SchizophreniaPutu Agus GrantikaNo ratings yet
- V37-4 Art 3 pp186-193Document8 pagesV37-4 Art 3 pp186-193wikka94No ratings yet
- Octreotid La Copii Cu HilotoraceDocument3 pagesOctreotid La Copii Cu HilotoraceMaria CostandachiNo ratings yet
- Oral Administration of Tannins and Flavonoids in Children With Acute Diarrhea: A Pilot, Randomized, Control-Case StudyDocument6 pagesOral Administration of Tannins and Flavonoids in Children With Acute Diarrhea: A Pilot, Randomized, Control-Case StudyAnonymous jM0QFnr0No ratings yet
- Asha Nayshalya Jafri (1511011004) Winny Rhamadani (1511011005) Nadya Prafita (1511011007) Indriyani (1511011008) Hurul Aini (1511011011)Document40 pagesAsha Nayshalya Jafri (1511011004) Winny Rhamadani (1511011005) Nadya Prafita (1511011007) Indriyani (1511011008) Hurul Aini (1511011011)Nadya PrafitaNo ratings yet
- Topamax Dosing Crushing Tablets and Special Administration Suspensionng Tube and RectalDocument3 pagesTopamax Dosing Crushing Tablets and Special Administration Suspensionng Tube and Rectalswhitton135No ratings yet
- Pubmed 15563759Document2 pagesPubmed 15563759Manigandan EdNo ratings yet
- Comparison of Octreotide and Hyoscine in Controlling Gastrointestinal Symptoms Due To Malignant Inoperable Bowel ObstructionDocument4 pagesComparison of Octreotide and Hyoscine in Controlling Gastrointestinal Symptoms Due To Malignant Inoperable Bowel ObstructionThiago GomesNo ratings yet
- Rasti 2007Document4 pagesRasti 2007agusNo ratings yet
- ID Evaluasi Sistem Pengelolaan Obat Instala PDFDocument6 pagesID Evaluasi Sistem Pengelolaan Obat Instala PDFWindy Gigiers SeptianiNo ratings yet
- Jurnal CovidDocument6 pagesJurnal CovidHanif MiftahNo ratings yet
- Tugas TSF KelompokDocument5 pagesTugas TSF KelompokWindy Gigiers SeptianiNo ratings yet
- Comparison Dipropionate: of Inhaled Twice PrednisoneDocument4 pagesComparison Dipropionate: of Inhaled Twice PrednisoneWindy Gigiers SeptianiNo ratings yet
- Role of Gastroesophageal Reflux Disease in Asthmatic PatientsDocument10 pagesRole of Gastroesophageal Reflux Disease in Asthmatic PatientsWindy Gigiers SeptianiNo ratings yet
- Theophylline PDFDocument3 pagesTheophylline PDFWindy Gigiers SeptianiNo ratings yet
- LupaDocument4 pagesLupaWindy Gigiers SeptianiNo ratings yet
- Medication Adherence in The Real WorldDocument13 pagesMedication Adherence in The Real WorldCognizantNo ratings yet
- List Maret 2023Document32 pagesList Maret 2023Klinik MMCNo ratings yet
- Working With Addicted PopulationsDocument9 pagesWorking With Addicted PopulationsWhimsical BrunetteNo ratings yet
- hw499 Unit5 3 Assignment Acupuncture Rachel MartinezDocument10 pageshw499 Unit5 3 Assignment Acupuncture Rachel Martinezapi-557736833No ratings yet
- 603 Integratedpharmacotherapy IIIsyllabus 081213Document11 pages603 Integratedpharmacotherapy IIIsyllabus 081213Ali AlyahawiNo ratings yet
- Lesson 3 Dosing SchedulingDocument20 pagesLesson 3 Dosing SchedulingAngelica GomezNo ratings yet
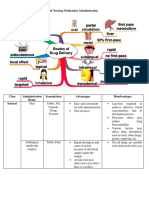
- Different Routes of Nursing Medication AdministrationDocument13 pagesDifferent Routes of Nursing Medication AdministrationRonica MendozaNo ratings yet
- Guide To Patient Support and Regional Cancer ServicesDocument76 pagesGuide To Patient Support and Regional Cancer Servicesgiovanna2004No ratings yet
- Dr. Lisa Marsch's NPF PresentationDocument32 pagesDr. Lisa Marsch's NPF PresentationNational Press Foundation100% (1)
- Pregabalin To Gabapentin Dose Conversion InformationDocument2 pagesPregabalin To Gabapentin Dose Conversion InformationVale RijaNo ratings yet
- Obat TaxolDocument53 pagesObat TaxolerdynNo ratings yet
- Role of Pharmacoeconomics in Formulary Management DecisionsDocument11 pagesRole of Pharmacoeconomics in Formulary Management DecisionsZakir AliNo ratings yet
- Cognitive Behavioral TherapyDocument10 pagesCognitive Behavioral TherapySean Flanderhijn100% (2)
- Proton FLASH Radiotherapy For The Treatment of Symptomatic Bone Metastases4Document8 pagesProton FLASH Radiotherapy For The Treatment of Symptomatic Bone Metastases4karnjNo ratings yet
- Usmle Physician Tasks/CompetenciesDocument12 pagesUsmle Physician Tasks/CompetenciesSara DziNo ratings yet
- Regimen Kanker RektumDocument8 pagesRegimen Kanker RektumNurul Kamilah SadliNo ratings yet
- Sword HealthDocument20 pagesSword HealthPranay VistaaNo ratings yet
- 2019E 14 - Supportive Care and Managment of Side EffectsDocument82 pages2019E 14 - Supportive Care and Managment of Side Effectsrusgal8992No ratings yet
- Apsy 603 Dual Relationship Assignment 4Document18 pagesApsy 603 Dual Relationship Assignment 4api-161848380100% (1)
- Treatment of Lupus Nephritis-1Document12 pagesTreatment of Lupus Nephritis-1Elizabeth MosqueraNo ratings yet
- PSY224-The Theory and Practice of Group Psychotherapy, 6th Edition-Irvin Yalom, Molyn Leszcz-2020Document762 pagesPSY224-The Theory and Practice of Group Psychotherapy, 6th Edition-Irvin Yalom, Molyn Leszcz-2020Raamiah Edwards100% (1)
- EsomeprazoleDocument2 pagesEsomeprazolenikki shein bullongNo ratings yet
- Family Therapy With AdolescentsDocument12 pagesFamily Therapy With AdolescentsFlorica PodariuNo ratings yet
- Part I - Antibiotics and The Human MicrobiomeDocument5 pagesPart I - Antibiotics and The Human MicrobiomeRejean Isip100% (3)
- Aaron T Beck PresentationDocument23 pagesAaron T Beck Presentationawilliams_976125100% (3)
- 2 Determination of Dose and Dosing IntervalDocument36 pages2 Determination of Dose and Dosing IntervalSreya Sanil100% (1)
- Investigational DrugsDocument25 pagesInvestigational Drugsamjad.46987No ratings yet
- Women and Pain Fact SheetDocument2 pagesWomen and Pain Fact SheetMustafa FahamNo ratings yet
- Reality TherapyDocument9 pagesReality TherapyVince ArqueroNo ratings yet