You might also like
- Panic at The DojoDocument290 pagesPanic at The DojoJones Devereaux50% (2)
- Fuse Box Passat b6Document19 pagesFuse Box Passat b6Ionut AlbuicaNo ratings yet
- Ayurvedic Sooranam PDFDocument255 pagesAyurvedic Sooranam PDFgautthum78671% (7)
- RSU PE 213 Module on Fundamentals of Games and SportsDocument87 pagesRSU PE 213 Module on Fundamentals of Games and SportsJhon Salazar Madalang60% (5)
- Fluiduty Barre ManualDocument65 pagesFluiduty Barre ManualJack Sellner100% (1)
- Chess Tactics in The GrobDocument11 pagesChess Tactics in The Grobsigiloso100% (1)
- Stargazer Class (D&D 5e)Document10 pagesStargazer Class (D&D 5e)Lucas De CarliNo ratings yet
- Lloyd Bud Winter - Relax and Win - Championship Performance (1981, Oak Tree Pubns) - Libgen - Li PDFDocument292 pagesLloyd Bud Winter - Relax and Win - Championship Performance (1981, Oak Tree Pubns) - Libgen - Li PDFQuan Vu100% (2)
- SEM636 Parts Manual OverviewDocument185 pagesSEM636 Parts Manual OverviewRicardo Barreto100% (1)
- Make Music CardsDocument20 pagesMake Music CardsShannon SmithNo ratings yet
- Catapillar Equipment Pricing 0701-12Document2,849 pagesCatapillar Equipment Pricing 0701-12MARCO ANTONIO64% (11)
- Deutsch Ganz Leicht A1 PDFDocument3 pagesDeutsch Ganz Leicht A1 PDFJavier Cano0% (8)
- Conditioning for Taekwon-doDocument27 pagesConditioning for Taekwon-doBobby KhalsaNo ratings yet
- ACL Return To Sport Guidelines and CriteriaDocument8 pagesACL Return To Sport Guidelines and CriteriaCamila Nicole Madrid GonzalezNo ratings yet
- Rehabilitation and Return To Sport Testing After ADocument6 pagesRehabilitation and Return To Sport Testing After ATotti DevaNo ratings yet
- Evaluación Clínica y Funcional Del HombroDocument9 pagesEvaluación Clínica y Funcional Del HombroLuis Eduardo Cabezas MirandaNo ratings yet
- Y-Balance Test: A Reliability Study Involving Multiple RatersDocument7 pagesY-Balance Test: A Reliability Study Involving Multiple RatersInaauliahanNo ratings yet
- Jurnal RSBMDocument9 pagesJurnal RSBMDiyah AyuningtiyasNo ratings yet
- A Clinician Friendly Test Battery With A Passing Rate Similar - 2023 - PhysicalDocument7 pagesA Clinician Friendly Test Battery With A Passing Rate Similar - 2023 - PhysicalmelcapontesadvNo ratings yet
- RunningDocument21 pagesRunningHossein NajjarzadeNo ratings yet
- A Systematic Review of Bracing Following Reconstruction of The ACLDocument10 pagesA Systematic Review of Bracing Following Reconstruction of The ACLDanar AdhimuktiNo ratings yet
- Rudisill Et Al 2022 Evidence Based Hamstring Injury Prevention and Risk Factor Management A Systematic Review and MetaDocument16 pagesRudisill Et Al 2022 Evidence Based Hamstring Injury Prevention and Risk Factor Management A Systematic Review and MetaFabian SepulvedaNo ratings yet
- Systematic ReviewDocument7 pagesSystematic ReviewErwin WibowoNo ratings yet
- Rotator Cuff Repair vs. Nonoperative Treatment - 2021 (Tema 3)Document12 pagesRotator Cuff Repair vs. Nonoperative Treatment - 2021 (Tema 3)Carlos NoronaNo ratings yet
- Criteria For Progressing Rehabilitation and Determining Return-to-Play Clearance Following Hamstring Strain Injury: A Systematic ReviewDocument13 pagesCriteria For Progressing Rehabilitation and Determining Return-to-Play Clearance Following Hamstring Strain Injury: A Systematic ReviewRaúl GonzálezNo ratings yet
- # Vestibular Rehabilitation Therapy On BalanceDocument17 pages# Vestibular Rehabilitation Therapy On BalancehanNo ratings yet
- Return To Sport Following Bankart RepairDocument6 pagesReturn To Sport Following Bankart RepairphantomkatalynNo ratings yet
- CPAxDocument9 pagesCPAxCarla CrivellaroNo ratings yet
- Adductor Injuries Aspetar PDFDocument11 pagesAdductor Injuries Aspetar PDFsofianosNo ratings yet
- S StreamDocument5 pagesS Streamad_c18No ratings yet
- Systematic Review of The Psychometric Properties of The Boston Carpal Tunnel QuestionnaireDocument10 pagesSystematic Review of The Psychometric Properties of The Boston Carpal Tunnel QuestionnaireSirfandi NurNo ratings yet
- 2019 Article 1189Document18 pages2019 Article 1189Cristian Sanabria DueñasNo ratings yet
- 2010 Mars Group Descriptive Epidemiology of The Multicenter ACL Revision Study (MARS) CohortDocument8 pages2010 Mars Group Descriptive Epidemiology of The Multicenter ACL Revision Study (MARS) CohortArmin ParavlićNo ratings yet
- Intra-rater Reliability of a Qualitative Landing Scale for the Single-Hop TestDocument8 pagesIntra-rater Reliability of a Qualitative Landing Scale for the Single-Hop TestFederico BristotNo ratings yet
- Fspor 04 1089882Document13 pagesFspor 04 1089882Barbara-Rose KolozsNo ratings yet
- Artificial Neural Network Learns Clinical Assessment of Spasticity in Modified Ashworth ScaleDocument9 pagesArtificial Neural Network Learns Clinical Assessment of Spasticity in Modified Ashworth ScalePrasasti 19No ratings yet
- Rehabilitation Protocols Following Total Knee Arthroplasty: A Review of Study Designs and Outcome MeasuresDocument20 pagesRehabilitation Protocols Following Total Knee Arthroplasty: A Review of Study Designs and Outcome MeasuresAlvaro AlarconNo ratings yet
- Cartilage Sports16Document19 pagesCartilage Sports16scribidubiduNo ratings yet
- Return To Sport After ACL Reconstruction Rates - DeFazio 2020Document15 pagesReturn To Sport After ACL Reconstruction Rates - DeFazio 2020luisNo ratings yet
- Picot Et Al 2023 Development and Validation of The Ankle Go Score For Discriminating and Predicting Return To SportDocument11 pagesPicot Et Al 2023 Development and Validation of The Ankle Go Score For Discriminating and Predicting Return To Sportpdelcampo1991No ratings yet
- Andrade Gabbettetal 2020 IstheACWRAssociatedwithRiskofTimeLossInjuryinProfessionalTeamSports SportsMedDocument24 pagesAndrade Gabbettetal 2020 IstheACWRAssociatedwithRiskofTimeLossInjuryinProfessionalTeamSports SportsMedSheilani MartinsNo ratings yet
- Return To Play After Hip Arthroscopy: A Systematic Review and Meta-AnalysisDocument9 pagesReturn To Play After Hip Arthroscopy: A Systematic Review and Meta-AnalysisEricNo ratings yet
- Cancer Treatment Reviews: Systematic or Meta-Analysis StudiesDocument14 pagesCancer Treatment Reviews: Systematic or Meta-Analysis StudiesMarioNo ratings yet
- The Assessment Management and Prevention of Calf MDocument29 pagesThe Assessment Management and Prevention of Calf MkevinNo ratings yet
- 1 s2.0 S0031940612000284 Main PDFDocument9 pages1 s2.0 S0031940612000284 Main PDFJuan Pablo Muñoz InocencioNo ratings yet
- Lateral Approach Versus Combined Lateral and Anteromedial Approach For Surgical Treatment of Terrible Triad of Elbow: A Meta-AnalysisDocument6 pagesLateral Approach Versus Combined Lateral and Anteromedial Approach For Surgical Treatment of Terrible Triad of Elbow: A Meta-AnalysisAndrea OsborneNo ratings yet
- 2021 Article 364Document28 pages2021 Article 364Shaun TylerNo ratings yet
- Accepted: Strength and Conditioning Journal Publish Ahead of Print DOI: 10.1519/SSC.0000000000000396Document22 pagesAccepted: Strength and Conditioning Journal Publish Ahead of Print DOI: 10.1519/SSC.0000000000000396Hugo TintiNo ratings yet
- 1 s2.0 S1015958421001019 MainDocument9 pages1 s2.0 S1015958421001019 MaincderosasNo ratings yet
- Complications and Downsides of The Robotic Total Knee Arthroplasty: A Systematic ReviewDocument15 pagesComplications and Downsides of The Robotic Total Knee Arthroplasty: A Systematic Reviewmamyeu1801No ratings yet
- Tarara2015 MMSS TestsDocument7 pagesTarara2015 MMSS TestsDanielBCNo ratings yet
- Effects of Respiratory Resistance Training With A Concurrent Flow Device On Wheelchair AthletesDocument8 pagesEffects of Respiratory Resistance Training With A Concurrent Flow Device On Wheelchair AthletesN onlyNo ratings yet
- 2020 Article 3872Document10 pages2020 Article 3872Gustavo BECERRA PERDOMONo ratings yet
- Ischemic Therapy in Musculoskeletal Medicine (4939)Document9 pagesIschemic Therapy in Musculoskeletal Medicine (4939)RexDavidGidoNo ratings yet
- Jurnal Fraktur PDFDocument9 pagesJurnal Fraktur PDFdwi vaniNo ratings yet
- 2023 - Surgical techniques for medial Patellofemoral ligamentDocument11 pages2023 - Surgical techniques for medial Patellofemoral ligamentorthotraumato30No ratings yet
- WILLIAMS 2022 - Injuries in Elite Men's Rugby Union - An Updated (2012-2020) MA of 11,620 Match and Training InjuriesDocument15 pagesWILLIAMS 2022 - Injuries in Elite Men's Rugby Union - An Updated (2012-2020) MA of 11,620 Match and Training InjuriesMauricio ZeniNo ratings yet
- Corticosteroid Use and Intensive Care Unit-Acquired Weakness: A Systematic Review and Meta-AnalysisDocument10 pagesCorticosteroid Use and Intensive Care Unit-Acquired Weakness: A Systematic Review and Meta-AnalysisEviNo ratings yet
- ASTRO Peer ReviewDocument23 pagesASTRO Peer ReviewEskadmas BelayNo ratings yet
- Whittaker Etal 2015Document9 pagesWhittaker Etal 2015SamuelNo ratings yet
- 1 s2.0 S2059775423004698 MainDocument7 pages1 s2.0 S2059775423004698 MainHalawa205No ratings yet
- Nazari 2019Document31 pagesNazari 2019cris.endo.ceNo ratings yet
- A Pilot Study of Aquatic Prehabilitation in Adults With Knee Osteoarthritis Undergoing Total Knee Arthroplasty - Short Term OutcomeDocument11 pagesA Pilot Study of Aquatic Prehabilitation in Adults With Knee Osteoarthritis Undergoing Total Knee Arthroplasty - Short Term Outcomerizki ikhsanNo ratings yet
- 1 s2.0 S2590109523000022 MainDocument20 pages1 s2.0 S2590109523000022 MainAnonymous HUY0yRexYfNo ratings yet
- Arthrogenic muscle inhibition after ACL reconstruction a scoping review of the efficacy of interventionsDocument11 pagesArthrogenic muscle inhibition after ACL reconstruction a scoping review of the efficacy of interventionsfilipecorsairNo ratings yet
- 1 s2.0 S1072751521021414 MainDocument24 pages1 s2.0 S1072751521021414 MainhendraNo ratings yet
- Swart 2016Document7 pagesSwart 2016TommysNo ratings yet
- Test - Retest Reliability of The One-Repetition Maximum (1RM) Strength Assessment: A Systematic ReviewDocument16 pagesTest - Retest Reliability of The One-Repetition Maximum (1RM) Strength Assessment: A Systematic ReviewbiosoccerNo ratings yet
- Effectiveness of Formal Physical Therapy Following Total Shoulder Arthroplasty: A Systematic ReviewDocument8 pagesEffectiveness of Formal Physical Therapy Following Total Shoulder Arthroplasty: A Systematic ReviewBüşra YılmazNo ratings yet
- Efcacy of Acupuncture CombinedDocument21 pagesEfcacy of Acupuncture Combined4evertigerNo ratings yet
- Physical Therapy in Sport: Margie Olds, Cade Coulter, Dan Marant, Tim UhlDocument7 pagesPhysical Therapy in Sport: Margie Olds, Cade Coulter, Dan Marant, Tim UhlNicol SandovalNo ratings yet
- Lee 2018Document7 pagesLee 2018Kings AndrewNo ratings yet
- Transcatheter Aortic Valve Replacement: A How-to Guide for Cardiologists and Cardiac SurgeonsFrom EverandTranscatheter Aortic Valve Replacement: A How-to Guide for Cardiologists and Cardiac SurgeonsNo ratings yet
- Alentorn Geli 2013 Prevention Part 1Document13 pagesAlentorn Geli 2013 Prevention Part 1sebakinesico-1No ratings yet
- Return To Sport After ACL Reconstruction How, When and WhyDocument6 pagesReturn To Sport After ACL Reconstruction How, When and Whysebakinesico-1No ratings yet
- NIH Public Access: ACL Reconstruction Rehabilitation: A Systematic Review Part IDocument10 pagesNIH Public Access: ACL Reconstruction Rehabilitation: A Systematic Review Part Isebakinesico-1No ratings yet
- NIH Public Access: ACL Reconstruction Rehabilitation: A Systematic Review Part IDocument10 pagesNIH Public Access: ACL Reconstruction Rehabilitation: A Systematic Review Part Isebakinesico-1No ratings yet
- Treatment of Anterior Cruciate Ligament Injuries in Professional Soccer Players by Orthopedic SurgeonsDocument6 pagesTreatment of Anterior Cruciate Ligament Injuries in Professional Soccer Players by Orthopedic Surgeonssebakinesico-1No ratings yet
- Alentorn Geli 2013 Prevention Part 1Document13 pagesAlentorn Geli 2013 Prevention Part 1sebakinesico-1No ratings yet
- Pronóstico de Las Pruebas Deportivas para El Riesgo de Nuevas Lesiones PDFDocument39 pagesPronóstico de Las Pruebas Deportivas para El Riesgo de Nuevas Lesiones PDFsebakinesico-1No ratings yet
- Van Me Lick 2016Document14 pagesVan Me Lick 2016Nicole Francisca Muñoz SalazarNo ratings yet
- Van Me Lick 2016Document14 pagesVan Me Lick 2016Nicole Francisca Muñoz SalazarNo ratings yet
- PAPER 2 SEMANA 1 2017-The Limits of Exercise Physiology - From Performance To HealthDocument12 pagesPAPER 2 SEMANA 1 2017-The Limits of Exercise Physiology - From Performance To Healthsebakinesico-1No ratings yet
- Return To Sport After ACL Reconstruction How, When and WhyDocument6 pagesReturn To Sport After ACL Reconstruction How, When and Whysebakinesico-1No ratings yet
- Pronóstico de Las Pruebas Deportivas para El Riesgo de Nuevas Lesiones PDFDocument39 pagesPronóstico de Las Pruebas Deportivas para El Riesgo de Nuevas Lesiones PDFsebakinesico-1No ratings yet
- PAPER 1 SEMANA 1 2017-Cellular and Molecular Exercise Physiology - Historical Perspective For The Discovery of Mechanisms Contributing To SkeletDocument13 pagesPAPER 1 SEMANA 1 2017-Cellular and Molecular Exercise Physiology - Historical Perspective For The Discovery of Mechanisms Contributing To Skeletsebakinesico-1No ratings yet
- One Page Dungeon - Eric Diaz - The Wretched HiveDocument1 pageOne Page Dungeon - Eric Diaz - The Wretched HiveAndy HaydenNo ratings yet
- Catalogo FiltrosDocument65 pagesCatalogo FiltrospatricioNo ratings yet
- B4164T3 2014 Service ScheduleDocument4 pagesB4164T3 2014 Service ScheduleFábio MagnoNo ratings yet
- NXEA Timetable 6 WebDocument19 pagesNXEA Timetable 6 Webapeerbux123No ratings yet
- Department of Mechanical Engineering, Government Engineering College, ModasaDocument1 pageDepartment of Mechanical Engineering, Government Engineering College, ModasaChirag N PatelNo ratings yet
- Sepak TakrawDocument8 pagesSepak TakrawMuhd Zulhilmi HazliNo ratings yet
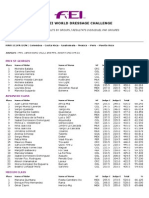
- 2013 WDC General Zone 2 ResultsDocument3 pages2013 WDC General Zone 2 ResultsPuertoRicoEcuestreNo ratings yet
- 05 - DD Tools1Document27 pages05 - DD Tools1Slim.BNo ratings yet
- League of Legends Macro GuideDocument3 pagesLeague of Legends Macro Guidevolwer02100No ratings yet
- Saudi Aramco Inspection Checklist: Final Inspection For Types I - V Fences SAIC-M-1005 30-Oct-17 CivilDocument4 pagesSaudi Aramco Inspection Checklist: Final Inspection For Types I - V Fences SAIC-M-1005 30-Oct-17 CivilAhmad BassemNo ratings yet
- Piper Cams Technical AdviceDocument4 pagesPiper Cams Technical AdviceBruno BinNo ratings yet
- WMKK PDFDocument78 pagesWMKK PDFJustin OngNo ratings yet
- m8 Dirtywave GuideDocument1 pagem8 Dirtywave Guidekqwt2z8qcxNo ratings yet
- Projectile Motion EDEXCELDocument16 pagesProjectile Motion EDEXCELThoon Nadi NaiNo ratings yet
- Copia de Inventario 25 Nov 22Document91 pagesCopia de Inventario 25 Nov 22Gretel Maite Mendoza PulidoNo ratings yet
- Astorga National High SchoolDocument2 pagesAstorga National High SchoolRuffa May OlayaNo ratings yet
- BPW-Luftfederungen 15731301eDocument20 pagesBPW-Luftfederungen 15731301eAhmed Abo ElkomsanNo ratings yet