You might also like
- Health Declaration Form DOT AmendedDocument1 pageHealth Declaration Form DOT AmendedImee S. YuNo ratings yet
- Internal Water and Baseline 18 March 2013Document83 pagesInternal Water and Baseline 18 March 2013Syarifah NordinNo ratings yet
- Job Description of Branch StaffDocument3 pagesJob Description of Branch StaffEleanor JamcoNo ratings yet
- Moa HousekeepingDocument1 pageMoa HousekeepingJoanne Pauline Tenedero - RuelaNo ratings yet
- Health Declaration FormDocument1 pageHealth Declaration FormXyrell Pis-ongNo ratings yet
- Director For Students AffairsDocument4 pagesDirector For Students AffairsSultan Kudarat State University100% (1)
- Cavite Mutiny ReportingDocument6 pagesCavite Mutiny ReportingJunna SumalinogNo ratings yet
- PA - PRO1 2019-015 Submission of Scanned Copy of CF4 As Additional Claim Requirement Until December 31, 2019Document1 pagePA - PRO1 2019-015 Submission of Scanned Copy of CF4 As Additional Claim Requirement Until December 31, 2019Leonard Paris GabatNo ratings yet
- English PortfolioDocument20 pagesEnglish PortfolioIon Pisari100% (1)
- Banned Visitor LetterDocument1 pageBanned Visitor Lettercharonn0100% (2)
- Memo On Safety & Health Protocols PDFDocument5 pagesMemo On Safety & Health Protocols PDFTrangia Plaza MichelleNo ratings yet
- Medical Certificate: Biliran Provincial HospitalDocument1 pageMedical Certificate: Biliran Provincial HospitalArvin Ian Reborn100% (1)
- Annex E Affidavit of Undertaking 2019 ScholarshipsDocument3 pagesAnnex E Affidavit of Undertaking 2019 ScholarshipsGlenn ClementeNo ratings yet
- OJT Convergy'sDocument1 pageOJT Convergy'sChris CioconNo ratings yet
- Feasibility StudyDocument3 pagesFeasibility Studyapi-264484515No ratings yet
- Form KRA1 SUC Levelling-Jun30Document17 pagesForm KRA1 SUC Levelling-Jun30Hadassah ChenNo ratings yet
- Return Service Accomplishment ReportDocument2 pagesReturn Service Accomplishment ReportJp TibayNo ratings yet
- Profile LamcorDocument26 pagesProfile LamcorRaquel Aragon Mien100% (2)
- Format in The Preparation of Project Proposal: A. Identifying InformationDocument2 pagesFormat in The Preparation of Project Proposal: A. Identifying InformationMSWDO STA. MAGDALENANo ratings yet
- OUSEE Admission and Enrollment ProcedureDocument4 pagesOUSEE Admission and Enrollment ProcedureCarlo NuñezNo ratings yet
- Failure To Login and or LogoutDocument1 pageFailure To Login and or LogoutArgie Corbo BrigolaNo ratings yet
- Application For Lto Clinical Lab.Document5 pagesApplication For Lto Clinical Lab.John Emmanuel Sy100% (1)
- 1stnycm ResolutionsDocument4 pages1stnycm ResolutionspenstalkerNo ratings yet
- Sample MemorandumDocument3 pagesSample MemorandumchrisNo ratings yet
- Ordinance No. 019-2011 (Smoke Free Ordinance) PDFDocument16 pagesOrdinance No. 019-2011 (Smoke Free Ordinance) PDFSheina Marie OnrubiaNo ratings yet
- Memorandum of Agreement The University of Mindanao and Davao City National High SchoolDocument9 pagesMemorandum of Agreement The University of Mindanao and Davao City National High SchoolJohn Russell MoralesNo ratings yet
- General Office ProceduresDocument3 pagesGeneral Office ProceduresNoona PlaysNo ratings yet
- Ojt Forms andDocument5 pagesOjt Forms andArvin F. VillodresNo ratings yet
- Case 2 Adjusting To The American Culture - Deva FabiolaDocument1 pageCase 2 Adjusting To The American Culture - Deva FabiolaBucin YoungbloodNo ratings yet
- Overtime Waiver: (On-the-Job Training / Practicum)Document1 pageOvertime Waiver: (On-the-Job Training / Practicum)John Kevin DiciembreNo ratings yet
- GIP Letter PDFDocument1 pageGIP Letter PDFLotes mae RegoyaNo ratings yet
- Seminars Attended ShsDocument2 pagesSeminars Attended ShsDherick RaleighNo ratings yet
- PermitDocument27 pagesPermitJoanna GarciaNo ratings yet
- RC6 SampleDocument6 pagesRC6 SampleSeptiyonoAdiPutroNo ratings yet
- Legal AspectsDocument3 pagesLegal AspectsFRANCINE JANE ALEJONo ratings yet
- Sample PLM CSWDocument15 pagesSample PLM CSWBernard BaluyotNo ratings yet
- Gip Accomplishment Report FormDocument1 pageGip Accomplishment Report FormAnonymous EvbW4o1U7No ratings yet
- Contact - Rizal Technological UniversityDocument9 pagesContact - Rizal Technological UniversityChristopher BrownNo ratings yet
- YFreLegForms - Deed of SaleDocument2 pagesYFreLegForms - Deed of SaleJan Uriel DavidNo ratings yet
- Hrim 128 Feasibility Study PDFDocument67 pagesHrim 128 Feasibility Study PDFGrace De la CruzNo ratings yet
- Application Letter Osa Uniform ExceptionDocument5 pagesApplication Letter Osa Uniform ExceptionJim Bryan RazNo ratings yet
- 13th MONTH PAY ResearchDocument3 pages13th MONTH PAY ResearchFritzTarronasNo ratings yet
- SIKAP Medical Certificate Template Filled OutDocument1 pageSIKAP Medical Certificate Template Filled OutAllen Day100% (1)
- 2307Document16 pages2307Analyn Velasco Matibag100% (1)
- Sample RRL For In-House ReviewDocument2 pagesSample RRL For In-House ReviewAeksio DaervesNo ratings yet
- Strategic PlanDocument11 pagesStrategic PlanPlacido Flores Verzola JrNo ratings yet
- The Architect's Professional Fee and Manner of Payment in An Owner-Architect' AgreementDocument1 pageThe Architect's Professional Fee and Manner of Payment in An Owner-Architect' AgreementYanahcute WattpadNo ratings yet
- Application LetterDocument1 pageApplication LetterMajenta OcampoNo ratings yet
- Maming Gala FormDocument2 pagesMaming Gala FormKoyawin XNo ratings yet
- Affidavit of Loss - CanenciaDocument1 pageAffidavit of Loss - CanenciaGabriellen QuijadaNo ratings yet
- A Case Study of Luntian Multi-Purpose Cooperative PDFDocument8 pagesA Case Study of Luntian Multi-Purpose Cooperative PDFNaruto UzumakiNo ratings yet
- Employee Acknowledgement of Maternity Benefits - SignedDocument2 pagesEmployee Acknowledgement of Maternity Benefits - SignedMarc CaurelNo ratings yet
- Sample Proposal Letter PDFDocument2 pagesSample Proposal Letter PDFRhelf Mae ValenciaNo ratings yet
- The Success of Angel's BurgerDocument1 pageThe Success of Angel's BurgerVanya Danyella BarachitaNo ratings yet
- Contact TracingDocument1 pageContact TracingSheryRose Panis SesoNo ratings yet
- Please Answer The Following Questions Truthfully. 2.: Tick Yes/NoDocument2 pagesPlease Answer The Following Questions Truthfully. 2.: Tick Yes/NoSusan Loida SorianoNo ratings yet
- Passport Application FormDocument2 pagesPassport Application FormMichael MontinolaNo ratings yet
- Visitors Contact Tracing Form Visitors Contact Tracing Form: Signature SignatureDocument1 pageVisitors Contact Tracing Form Visitors Contact Tracing Form: Signature SignatureCherrie Lynne AlbisNo ratings yet
- Male Head of HouseholdDocument3 pagesMale Head of HouseholdAlexander Haruna SaturdayNo ratings yet
- Profile of Contacts - COVID-19 - 041520Document2 pagesProfile of Contacts - COVID-19 - 041520jheanniver nabloNo ratings yet
- 02 StatisticDocument8 pages02 StatistickablasNo ratings yet
- 1 StandardReportDocument24 pages1 StandardReportkablasNo ratings yet
- 02 StatisticDocument16 pages02 StatistickablasNo ratings yet
- Meolcrt-Ciiy: BreastDocument4 pagesMeolcrt-Ciiy: BreastkablasNo ratings yet
- Meolcrt-Ciiy: BreastDocument4 pagesMeolcrt-Ciiy: BreastkablasNo ratings yet
- Chaves, PersonsDocument20 pagesChaves, Personsamareia yapNo ratings yet
- 11 StatisticDocument15 pages11 StatistickablasNo ratings yet
- 001 2021 2 MonDocument6 pages001 2021 2 MonkablasNo ratings yet
- 1 StandardReportDocument15 pages1 StandardReportkablasNo ratings yet
- 1 StandardReportDocument34 pages1 StandardReportkablasNo ratings yet
- 10 StatisticDocument11 pages10 StatistickablasNo ratings yet
- Statutory Construction Power PointDocument22 pagesStatutory Construction Power PointkablasNo ratings yet
- 02 StatisticDocument16 pages02 StatistickablasNo ratings yet
- 10 StatisticDocument15 pages10 StatistickablasNo ratings yet
- PFR Midterm Review GuideDocument7 pagesPFR Midterm Review GuidekablasNo ratings yet
- 001 2020 10 MonDocument13 pages001 2020 10 MonkablasNo ratings yet
- DISBURSEMENT Hapihap Spa and MassageDocument1 pageDISBURSEMENT Hapihap Spa and MassagekablasNo ratings yet
- 4 Ess 22 PatternsDocument21 pages4 Ess 22 PatternsJerico Ortega SantosNo ratings yet
- 4 Ess 22 PatternsDocument21 pages4 Ess 22 PatternsJerico Ortega SantosNo ratings yet
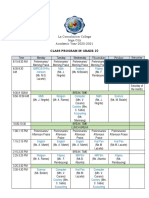
- Class Program in Grade 10: SaturdayDocument2 pagesClass Program in Grade 10: SaturdaykablasNo ratings yet
- PFR Midterm Review Guide IIDocument23 pagesPFR Midterm Review Guide IIkablasNo ratings yet
- Olive Porch OrganicsDocument67 pagesOlive Porch OrganicskablasNo ratings yet
- Statutory Construction NotesDocument32 pagesStatutory Construction Notespriam gabriel d salidaga95% (102)
- 4 Ess 22 PatternsDocument21 pages4 Ess 22 PatternsJerico Ortega SantosNo ratings yet
- AUTHORIZATIONDocument1 pageAUTHORIZATIONkablasNo ratings yet
- Clients Safety GuidelinesDocument2 pagesClients Safety GuidelineskablasNo ratings yet
- Daedalus and Icarus Worksheet 1Document2 pagesDaedalus and Icarus Worksheet 1kablasNo ratings yet
- Summary of Jurisdiction of Philippine CourtsDocument13 pagesSummary of Jurisdiction of Philippine CourtskablasNo ratings yet
- Activity 2.2Document2 pagesActivity 2.2kablasNo ratings yet
- Rent Payment Acknowledgement Letter TemplateDocument1 pageRent Payment Acknowledgement Letter TemplatekablasNo ratings yet
- C7CJ5Z: Payment InformationDocument3 pagesC7CJ5Z: Payment InformationSutri HeydiNo ratings yet
- Module 1 - Tourism Planning and DevelopmentDocument22 pagesModule 1 - Tourism Planning and Developmentjohn paolo aris100% (1)
- Pobble Barkast, A Sensible Stalwart Gnome With A Passion For His Craft, Regularly Finding Work AmongDocument1 pagePobble Barkast, A Sensible Stalwart Gnome With A Passion For His Craft, Regularly Finding Work AmongJack ClintonNo ratings yet
- The JourneyDocument4 pagesThe JourneyTAMISH GAMBHIR 2112664No ratings yet
- Document 3Document3 pagesDocument 3Mae BalmaterNo ratings yet
- Amadeus Training Course 3927784553Document1 pageAmadeus Training Course 3927784553Erblina GjimishkaNo ratings yet
- Access and Interpret Product Information: D2.TTA - CL2.01 Assessor ManualDocument66 pagesAccess and Interpret Product Information: D2.TTA - CL2.01 Assessor ManualCindy joy TisbeNo ratings yet
- Local Tour Itinerary: Cebu City Tour Other Expenses (Optional)Document6 pagesLocal Tour Itinerary: Cebu City Tour Other Expenses (Optional)Eurresse TalisicNo ratings yet
- Travel Document For Maallemi - Amel - Olvp8qDocument1 pageTravel Document For Maallemi - Amel - Olvp8qAmalNo ratings yet
- DHNHHCM - Writing Test 2Document6 pagesDHNHHCM - Writing Test 2Phạm Anh TuấnNo ratings yet
- Ticket 4 60457669 27455912Document2 pagesTicket 4 60457669 27455912narayanaNo ratings yet
- Tourism Network and Supply Components: The TravelerDocument9 pagesTourism Network and Supply Components: The TravelerAngela MendozaNo ratings yet
- EmiratesTicket1 1Document3 pagesEmiratesTicket1 1azzadari0555No ratings yet
- JapDocument7 pagesJaposho99No ratings yet
- Cls 8, 2019Document2 pagesCls 8, 2019Andreea RaduNo ratings yet
- VGM 29Document1 pageVGM 29Shilpa DograNo ratings yet
- Quality Service Management in Tourism and Hospitality Module 1Document105 pagesQuality Service Management in Tourism and Hospitality Module 1Redhorse1100% (9)
- SIA B - Case StudyDocument2 pagesSIA B - Case StudyDhanashree GharatNo ratings yet
- 5 Star Hotels PDFDocument5 pages5 Star Hotels PDFSenthil Kumar100% (2)
- Evolve - L1 - Midterm - Units 7-12 - ADocument6 pagesEvolve - L1 - Midterm - Units 7-12 - ASongsitNo ratings yet
- Lta GuidelineDocument2 pagesLta Guidelinevenkatesh8919chNo ratings yet
- Pnr/Booking Ref.: Ljsukf: Indigo Passenger - 1/1 Mr. Gubbala MaharajuDocument3 pagesPnr/Booking Ref.: Ljsukf: Indigo Passenger - 1/1 Mr. Gubbala MaharajuKoteswar MandavaNo ratings yet
- Alwi BatikDocument2 pagesAlwi BatikMuh Alwi Umar SyecherBerkhidmahNo ratings yet
- HIDDEN TREASURES OF SIKKIM 2.0 With Kanupriya - Winter EditionDocument10 pagesHIDDEN TREASURES OF SIKKIM 2.0 With Kanupriya - Winter EditionShikha NairNo ratings yet
- VISA REQUIREMENTS AND COST ResearchDocument8 pagesVISA REQUIREMENTS AND COST Researchmariam hassanNo ratings yet
- Geography AssignmentDocument19 pagesGeography AssignmentIlliden ian jrNo ratings yet
- E Ticket Itinerary and ReceiptDocument6 pagesE Ticket Itinerary and ReceiptGraham EvansNo ratings yet
- A8D460782594700B86947B300Document2 pagesA8D460782594700B86947B300nathumeghwalsagwaNo ratings yet
- LandAir Paradise Travels and Tours - Feasibility StudyDocument74 pagesLandAir Paradise Travels and Tours - Feasibility StudyMarnelli CatalanNo ratings yet
- V-AIR Headset PF Final Version 1Document71 pagesV-AIR Headset PF Final Version 1K BNo ratings yet