Professional Documents
Culture Documents
Articulo Mantequilla PDF
Uploaded by
Adriàn Guillermo Mantilla RoaOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Articulo Mantequilla PDF
Uploaded by
Adriàn Guillermo Mantilla RoaCopyright:
Available Formats
Articles
Quarter-dose quadruple combination therapy for initial
treatment of hypertension: placebo-controlled, crossover,
randomised trial and systematic review
Clara K Chow, Jay Thakkar, Alex Bennett, Graham Hillis, Michael Burke, Tim Usherwood, Kha Vo, Kris Rogers, Emily Atkins, Ruth Webster,
Michael Chou, Hakim-Moulay Dehbi, Abdul Salam, Anushka Patel, Bruce Neal, David Peiris, Henry Krum*, John Chalmers, Mark Nelson,
Christopher M Reid, Mark Woodward, Sarah Hilmer, Simon Thom, Anthony Rodgers
Summary
Background Globally, most patients with hypertension are treated with monotherapy, and control rates are poor Lancet 2017; 389: 1035–42
because monotherapy only reduces blood pressure by around 9/5 mm Hg on average. There is a pressing need for Published Online
blood pressure-control strategies with improved efficacy and tolerability. We aimed to assess whether ultra-low-dose February 9, 2017
http://dx.doi.org/10.1016/
combination therapy could meet these needs.
S0140-6736(17)30260-X
See Comment page 989
Methods We did a randomised, placebo-controlled, double-blind, crossover trial of a quadpill—a single capsule
*Deceased
containing four blood pressure-lowering drugs each at quarter-dose (irbesartan 37·5 mg, amlodipine 1·25 mg,
The George Institute for Global
hydrochlorothiazide 6·25 mg, and atenolol 12·5 mg). Participants with untreated hypertension were enrolled from Health, University of Sydney,
four centres in the community of western Sydney, NSW, Australia, mainly by general practitioners. Participants were Sydney, NSW, Australia
randomly allocated by computer to either the quadpill or matching placebo for 4 weeks; this treatment was followed (Prof C K Chow PhD,
by a 2-week washout, then the other study treatment was administered for 4 weeks. Study staff and participants were J Thakkar MBBS,
A Bennett MPhil,
unaware of treatment allocations, and masking was achieved by use of identical opaque capsules. The primary Prof G Hillis PhD, K Vo BSc,
outcome was placebo-corrected 24-h systolic ambulatory blood pressure reduction after 4 weeks and analysis was by K Rogers PhD, E Atkins PhD,
intention to treat. We also did a systematic review of trials evaluating the efficacy and safety of quarter-standard-dose R Webster PhD, A Salam PhD,
blood pressure-lowering therapy against placebo. This trial is registered with the Australian New Zealand Clinical Prof A Patel PhD,
Prof B Neal PhD, D Peiris PhD,
Trials Registry, number ACTRN12614001057673. The trial ended after 1 year and this report presents the final analysis. Prof J Chalmers PhD,
Prof M Woodward PhD,
Findings Between November, 2014, and December, 2015, 55 patients were screened for our randomised trial, of whom Prof A Rodgers PhD); Westmead
21 underwent randomisation. Mean age of participants was 58 years (SD 11) and mean baseline office and 24-h Hospital, Sydney, NSW,
Australia (Prof C K Chow,
systolic and diastolic blood pressure levels were 154 (14)/90 (11) mm Hg and 140 (9)/87 (8) mm Hg, respectively. One J Thakkar); Kildare Road Medical
individual declined participation after randomisation and two patients dropped out for administrative reasons. The Centre, Sydney, NSW, Australia
placebo-corrected reduction in systolic 24-h blood pressure with the quadpill was 19 mm Hg (95% CI 14–23), and (M Burke PhD); The University
of Sydney, Sydney, NSW,
office blood pressure was reduced by 22/13 mm Hg (p<0·0001). During quadpill treatment, 18 (100%) of 18 participants
Australia (Prof T Usherwood MD,
achieved office blood pressure less than 140/90 mm Hg, compared with six (33%) of 18 during placebo treatment Prof S Hilmer PhD,
(p=0·0013). There were no serious adverse events and all patients reported that the quadpill was easy to swallow. Our Prof A Rodgers); The University
systematic review identified 36 trials (n=4721 participants) of one drug at quarter-dose and six trials (n=312) of of Western Australia, Perth,
WA, Australia (Prof G Hillis);
two drugs at quarter-dose, against placebo. The pooled placebo-corrected blood pressure-lowering effects were
Johns Hopkins Bloomberg
5/2 mm Hg and 7/5 mm Hg, respectively (both p<0·0001), and there were no side-effects from either regimen. School of Public Health,
Baltimore, MD, USA
Interpretation The findings of our small trial in the context of previous randomised evidence suggest that the benefits of (M Chou MBBS); Imperial
College, London, UK
quarter-dose therapy could be additive across classes and might confer a clinically important reduction in blood pressure.
(H-M Dehbi MRes,
Further examination of the quadpill concept is needed to investigate effectiveness against usual treatment options and Prof S Thom PhD, Prof B Neal);
longer term tolerability. Department of Epidemiology
and Preventive Medicine,
Monash University, Melbourne,
Funding National Heart Foundation, Australia; University of Sydney; and National Health and Medical Research
Vic, Australia (Prof H Krum);
Council of Australia. Menzies Institute for Medical
Research, University of
Introduction Many factors contribute to poor blood pressure control, Tasmania, Hobart, Tas,
Australia (Prof M Nelson PhD);
High blood pressure is a leading cause of preventable including low adherence rates, complex guidelines Curtin University, Perth, WA,
morbidity and mortality,1 and the benefits of blood recommending multiple up-titration steps, and treatment Australia (Prof C M Reid PhD);
pressure-lowering treatments are well established.2,3 inertia. Most treated patients only receive monotherapy,4 Charles Perkins Centre,
Despite the plethora of blood pressure-lowering medicines which has low potency even at high doses.5 Furthermore, University of Sydney, Sydney,
NSW, Australia (Prof C K Chow,
available, and the fact that, once found to have high blood the increasingly strong evidence showing benefits of more Prof B Neal); and Royal Prince
pressure, most patients receive some treatment, findings intensive blood pressure lowering6,7 highlights the need for Alfred Hospital, Sydney, NSW,
of multiple large-scale population studies show poor blood new treatment strategies that are more efficacious while Australia (Prof A Patel,
pressure control in many patients globally.4 remaining tolerable. Low-dose combination therapy holds Prof B Neal)
www.thelancet.com Vol 389 March 11, 2017 1035
Articles
Correspondence to:
Prof Clara K Chow, The George Research in context
Institute for Global Health—
Australia, Camperdown, Evidence before this study therapy and found that one and two drugs at quarter-dose led
NSW 2050, Australia Findings of a systematic review and meta-analysis of to placebo-corrected blood pressure reductions of 5/2 mm Hg
cchow@georgeinstitute.org.au 354 randomised, double-blind, placebo-controlled trials of and 7/5 mm Hg, respectively. These reductions were not
blood pressure-lowering therapy showed that associated with any difference in side-effects compared with
half-standard-dose achieved almost 80% as much blood placebo. Our trial provides the first placebo-controlled data on
pressure lowering as did standard dose, and that the blood four quarter doses, indicating a 22/13 mm Hg reduction in
pressure-lowering effect of different classes of drugs was blood pressure.
additive. Although most benefits were maintained at half-dose,
Implications of all the available evidence
most side-effects were avoided. Findings of another trial
Our study provides proof-of-concept for an innovative
showed that four drugs at quarter-dose achieved greater blood
approach of using ultra-low-dose quadruple combination
pressure reduction than did each component at standard dose.
therapy to achieve substantial blood pressure reductions.
Added value of this study Further studies are needed to examine the generalisability of
We systematically reviewed the literature on these findings and assess the longer term effects on efficacy,
placebo-controlled, quarter-dose blood pressure-lowering safety, and tolerability compared with usual care.
For the British National considerable promise in this regard since at low doses the British National Formulary, Martindale: The Complete
Formulary see https://www.bnf. most side-effects are avoided and most benefits are Drug Reference,9 and the Monthly Index of Medical
org
maintained.8 However, there is uncertainty about effects at Specialties.10 Two reviewers (AB, MC) extracted data
ultra-low doses and whether combinations can achieve independently using a standard extraction form. A third
clinically relevant blood pressure reductions. We, therefore, reviewer (AR) resolved any differences. We analysed data
sought to assess efficacy and tolerability of ultra-low-dose using Comprehensive Meta-Analysis, version 3 (Biostat,
combination therapy by conducting a systematic review of Englewood, NJ, USA). We used a fixed-effect model to
quarter-dose blood pressure-lowering therapies and a estimate the effects of quarter-dose blood pressure-
randomised trial of a quadpill containing four common lowering therapy on blood pressure lowering and on
blood pressure-lowering medications, each at quarter- adverse events, compared with placebo. We assessed the
dose. effect on blood pressure using the mean change in systolic
blood pressure and diastolic blood pressure from baseline
Methods to end of study, with stan dar
disation to a baseline of
Systematic review 150/95 mm Hg.8 Adverse events included all that were
We did a systematic review of all randomised trials of reported by trials at follow-up.
quarter-dose blood pressure therapy, identifying
potentially relevant studies from searches of Embase, Clinical trial design and participants
MEDLINE, and the Cochrane Central Registry of The Quadpill study was a randomised, placebo-controlled,
Controlled Trials, with each source searched from double-blind, crossover trial (figure 1). We recruited
inception to June, 2016; we also searched the websites of participants from four centres in the community, predomi
the US Food and Drug Administration and the European nantly through general practices, in western Sydney, NSW,
Medicines Agency. MEDLINE search terms are provided Australia. We judged participants eligible if they met the
See Online for appendix in the appendix (pp 1, 2). We searched trial registers for following inclusion criteria: adults aged 18 years and older;
any ongoing trials, including WHO’s International office systolic blood pressure greater than 140 mm Hg or
Clinical Trials Registry platform, the Australian New diastolic blood pressure greater than 90 mm Hg, or both,
Zealand Clinical Trials Registry, and the Clinical Trials on two readings on separate days; baseline ambulatory
Registry—India. We also retrieved studies from systolic blood pressure greater than 135 mm Hg or diastolic
reference lists of key clinical trials, systematic reviews, blood pressure greater than 85 mm Hg, or both; and not
and published articles, and reviewed the reference taking any blood pressure drugs. Exclusion criteria
lists of eligible studies and systematic reviews included: definite contraindication to one or more
(appendix pp 3–6, 14). We included randomised controlled component agents in the quadpill; the responsible clinician
trials of adult participants (≥18 years of age) in which judged that a change in current therapy would place the
quarter-standard-dose blood pressure-lowering drugs patient at risk; severe or accelerated hypertension;
were compared with placebo for the following drug classes: pregnancy; inability to provide informed consent; and
angiotensin-converting-enzyme inhibitors; angiotensin medical illness with anticipated life expectancy less than
receptor II blockers; β blockers; calcium-channel blockers; 3 months.
and thiazide and thiazide-like diuretics. Quarter-dose was The study protocol was approved by the human research
a quarter of the standard dose, defined as the most and ethics committee at the University of Sydney.
frequently reported usual maintenance dose recorded by We obtained informed consent from all participants.
1036 www.thelancet.com Vol 389 March 11, 2017
Articles
Randomisation and masking oedema, skin rash, or itching. The study doctor (JT) and
We randomly allocated participants in a 1:1 ratio to either: a clinical cardiologist, in consultation with the principal
a group receiving the quadpill for 4 weeks, followed by a investigator if needed, judged the severity of adverse
2-week placebo washout, then placebo for 4 weeks; or a events and whether they were related to study treatment.
group receiving placebo, then washout, then the quadpill We provided study drugs and investigations at no cost to
for the same periods. The quadpill was a single participants and we reimbursed nominal amounts to
encapsulated pill containing four common blood pressure- cover travel and parking costs.
lowering drugs, each at quarter-standard-dose, as defined
above (irbesartan 37·5 mg, amlodipine 1·25 mg, hydro Outcomes
chlorothiazide 6·25 mg, and atenolol 12·5 mg). The primary outcome was reduction in mean 24-h
We selected the most commonly used drug from each systolic blood pressure at 4 weeks using ambulatory
class in Australia. We obtained quarter-doses by halving blood pressure monitoring. Secondary outcomes
half-dose tablets using a pill-splitting device, without included: reduction in mean 24-h diastolic blood pressure
crushing, and we weighed the pills to ensure accuracy of and in daytime and night-time systolic and diastolic
halving doses. We then encapsulated the quarter doses blood pressure at 4 weeks; reduction in office systolic and
using gelatine capsules (DBCaps; Capsugel, Morristown, diastolic blood pressure, as measured by a standardised
NJ, USA). All trial medicines were prepared and packaged automated blood pressure cuff; the proportion of
at a manufacturing facility licensed with a Certificate of participants with controlled blood pressure at 4 weeks
Good Manufacturing Practice by the Therapeutic Goods (defined as <135/85 mm Hg 24-h ambulatory blood
Administration of Australia. pressure and <140/90 mm Hg office blood pressure);
Treatment allocations were done at random via a adverse events and prespecified adverse events with
computer-assisted randomisation sequence and were laboratory-associated parameters (ie, rise in alanine
masked to study staff enrolling participants, care aminotransferase and aspartate aminotransferase of
providers, outcome assessors, and participants. The more than three times the upper limit of normal, or
placebo capsule appeared identical and contained doubling if baseline levels were known to be elevated;
four placebo tablets of similar weight to those in the a drop in estimated glomerular filtration rate by more
quadpill. We gave participants a single daily capsule than 20%, as estimated from serum creatinine; and a
quadpill or placebo throughout the trial. We instructed change in levels of sodium, potassium, and uric acid);
patients to take the capsules at the same time each day, and assessment of acceptability and tolerability.
preferably in the morning. In addition to the study drugs,
we provided all participants with education on healthy Patients with untreated high blood pressure
lifestyle options, as recommended by local blood pressure (two office blood pressure measures on two
different days >140/90 mm Hg)
management guidelines that were current at the time.11
Procedures Baseline visit (week 0)
We did 24-h ambulatory blood pressure monitoring Clinical questionnaire, 24-h ambulatory blood pressure,
blood tests
four times (figure 1): at baseline (off study drug);
at 4 weeks (period one treatment or placebo); at 6 weeks
(after 2-week placebo washout); and at 10 weeks (period Randomise
two treatment or placebo). Ambulatory blood pressure
monitoring machines were calibrated according to the
manufacturer’s specification. We recorded office blood
Week 0–4 Quadpill* Placebo
pressure three times at each study visit using an Omron
T9P blood pressure monitor (HEM-759-C1; Omron Visit 2 (week 4): 24-h blood pressure, blood tests, adverse events
Healthcare, Hoofddorp, Netherlands). We averaged the
second and third readings for study analysis. We took
readings while participants were seated and rested, but Week 4–6 2-week washout 2-week washout
not while they had been left unattended.11 Furthermore,
at week 4 and week 10, we did blood biochemistry Visit 3 (week 6): 24-h blood pressure
analyses and administered a questionnaire for clinical
side-effects and medication compliance. At study end, Week 6–10 Placebo Quadpill*
we assessed drug acceptability and tolerability.
We recorded all adverse events and asked patients Final visit (week 10): 24-h blood pressure, blood tests, adverse events,
specifically about clinical adverse events possibly acceptability questionnaire
associated with blood pressure-lowering drugs—ie,
dizziness, blurred vision, syncope or collapse, chest pain Figure 1: Study design
or angina, shortness of breath, cough, wheeze, pedal *Quadpill comprises irbesartan 37·5 mg, amlodipine 1·25 mg, hydrochlorothiazide 6·25 mg, and atenolol 12·5 mg.
www.thelancet.com Vol 389 March 11, 2017 1037
Articles
prognostic covariates. We reported compliance to study
55 screened drug using data for pills (doses) taken and missed doses
over the study period. We used a linear mixed model to
34 not randomised estimate the effect of the treatment on change in mean
11 medically ineligible 24-h systolic blood pressure from baseline for each
10 too busy or declined participation treatment period (primary outcome), according to the
5 white-coat hypertension
9 not contactable Kenward and Roger approach.12 We included all available
data in the model; no missing data were imputed. If a
patient had missing data for one period, we used data
21 eligible for randomisation
from the available period. We did a sensitivity analysis
including only patients with data available from both
1 patient declined study drug initiation periods. We also adjusted the denominator degrees of
freedom of Kenward and Roger13 to optimise for the small
sample size.
20 patients in trial
We tested for carry-over with an unpaired t test of the
main outcome, with order as an effect. We tested period
2 participants withdrew effect by using a paired t test comparing the main
outcome in period one (baseline to week 4) with main
outcome in period two (week 6 to week 10) from the
18 participants completed 10 weeks
same patient. As well as the Kenward and Roger
approach, we also did a sensitivity analysis using a
Figure 2: Trial profile standard paired t test to compare the change in primary
outcome between different periods.
We analysed continuous secondary endpoints with
Participants (n=21)
baseline values (eg, daytime/night-time ambulatory
Age (years) 58 (11)
systolic/diastolic blood pressure) similarly to the primary
Sex endpoint. We analysed other continuous variables without
Male 10 (48%) a baseline value in each period with a paired t test. We have
Female 11 (52%) reported counts and percentages of all adverse events.
University education 9 (43%) We tested for interaction of treatment effect with age
24-h systolic blood pressure/diastolic blood 140 (9)/87 (8) (≤60 vs >60 years), sex, and body-mass index (BMI ≤30 vs
pressure (mm Hg)
>30 kg/m²). We also did subgroup analyses for each
Office systolic blood pressure/diastolic blood 154 (14)/90 (11)
pressure (mm Hg)
variable. We did trial analyses using SAS version 9.4.
Time since diagnosis of hypertension (months) 4·2 (5·4)
This trial is registered with the Australian and
New Zealand Clinical Trials Registry, number
Diabetes 2 (10%)
ACTRN12614001057673.
Hyperlipidaemia 5 (24%)
Previous myocardial infarction 0
Role of the funding source
Coronary artery revascularisation 0
The funder had no role in study design, data collection,
Cerebrovascular disease 0
data analysis, data interpretation, or writing of the report.
Previous depression 4 (19%)
KV, KR, CKC, and AR had full access to all data in the
Current smoker 5 (46%)
study. CKC and AR had final responsibility for the
Data are mean (SD) or number of patients (%). decision to submit for publication.
Table 1: Baseline characteristics of trial participants
Results
Between November, 2014, and December, 2015,
Statistical analysis 55 patients were screened for the Quadpill trial, and
We planned a sample size of 50 patients to provide 21 individuals were judged eligible and randomly
90% power at an α of 0·05, to detect a difference in allocated to a treatment group (figure 2). Baseline
systolic blood pressure of 12 mm Hg between the characteristics of the study population are shown in
quadpill and placebo, assuming an SD of the within- table 1. One patient declined participation before study
patient difference of 12 mm Hg and taking into account drug initiation and two participants withdrew at the end
the possibility of a 10% loss to follow-up. The study ended of the first treatment period for social reasons (figure 2).
at 1 year at the end of the budget and staffing time Therefore, 18 patients had complete data for the primary
allocated and the original sample size was not reached. outcome.
Analyses were by intention to treat. All tests were two- The difference in mean 24-h systolic blood pressure
sided. All statistical analyses were unadjusted for between quadpill and placebo periods was 18·7 mm Hg
1038 www.thelancet.com Vol 389 March 11, 2017
Articles
Quadpill treatment period Placebo treatment period Difference* p value
(95% CI)
Baseline (week 0 or End of treatment Baseline (week 0 End of treatment
week 6) (week 4 or week 10) or week 6) (week 4 or week 10)
24-h systolic blood pressure 138·4 (7·3) 119·6 (7·6) 137·1 (10·4) 138·2 (10·0) 18·7 (14·3–23·0) <0·0001
24-h diastolic blood pressure 86·7 (10·6) 73·3 (8·7) 85·1 (9·4) 87·6 (11·9) 14·2 (11·5–16·9) <0·0001
Daytime ambulatory systolic blood 141·7 (7·7) 121·4 (7·9) 140·3 (11·6) 143·7 (10·5) 22·3 (17·7–26·9) <0·0001
pressure
Daytime ambulatory diastolic blood 89·9 (11·0) 75·7 (9·2) 87·9 (9·5) 91·1 (12·5) 15·3 (12·6–18·1) <0·0001
pressure
Night-time ambulatory systolic 128·8 (13·4) 114·4 (9·0) 126·2 (9·2) 125·4 (13·4) 10·4 (2·6–18·3) 0·0128
blood pressure
Night-time ambulatory diastolic 77·7 (12·9) 66·8 (8·9) 77·8 (10·0) 79·4 (13·1) 12·5 (7·9–17·1) <0·0001
blood pressure
Office systolic blood pressure 149·9 (16·7) 122·1 (8·8) 145·8 (10·2) 144·6 (12·2) 22·4 (16·5–28·3) <0·0001
Office diastolic blood pressure 87·4 (10·0) 71·8 (8·9) 86·1 (11·3) 84·8 (12·1) 13·1 (8·9–17·3) <0·0001
Data are mean (SD), unless otherwise stated. *Difference in change between quadpill and placebo period.
Table 2: Effects of quadpill and placebo on blood pressure variables
Study drug allocated when Treatment period when Severity* Action taken Outcome Relation to
adverse event occurred adverse event occurred study drug*
Gastrointestinal illness Quadpill First Mild None Resolved Not related
Headache Quadpill First Mild None Resolved Not related
Dry nose Placebo Second Mild None Resolved Not related
Vertigo Neither Between first and second Mild None Resolved Not related
Dizziness Quadpill First Mild Temporarily discontinued Resolved Related
study drug
Increased urinary Quadpill First Mild None Resolved Possibly related
frequency†
Increased urinary Placebo Second Mild None Resolved Possibly related
frequency†
Respiratory-tract infection Quadpill Second Mild None Resolved Not related
*Judged by the study doctor (JT) and a clinical cardiologist, in consultation with the principal investigator if needed. †Reported by one male patient during the intervention
period and the same patient in the placebo period; we instructed him to consult a local doctor for urological assessment.
Table 3: Adverse events
(95% CI 14·3–23·0), and in 24-h diastolic blood pressure significant interactions by age, sex, or BMI. In one
was 14·2 mm Hg (11·5–16·9). Similarly, the difference in sensitivity analysis, using a standard comparison (paired
office systolic and diastolic blood pressure was 22·4 mm Hg t test), results were virtually identical, with a difference in
(16·5–28·3) and 13·1 mm Hg (8·9–17·3), respectively mean 24-h systolic blood pressure between the quadpill
(table 2). Daytime ambulatory systolic blood pressure, and placebo of 18·7 mm Hg (95% CI 14·3–23·0;
daytime ambulatory diastolic blood pressure, night-time appendix p 12). Similarly, in a second sensitivity analysis,
ambulatory systolic blood pressure, and night-time in which we only included patients who did not have
ambulatory diastolic blood pressure were all significantly missing data (n=18), results were also virtually identical,
lower with the quadpill (table 2). All participants (18/18 with the difference in mean 24-h systolic blood pressure
[100%]) achieved office systolic and diastolic blood pressure of 18·7 mm Hg (95% CI 14·2–23·2).
less than 140/90 mm Hg while on the quadpill, compared Treatment compliance was high, with a mean number
with six (33%) of 18 while on placebo (risk ratio [RR] 3·01, of capsules missed in the last week of 0·2 (SD 0·4) for
95% CI 1·54–5·89; p=0·0013). Ambulatory blood pressure the quadpill and 0·3 (0·6) for placebo. 18 participants
less than 135/85 mm Hg was achieved by 15 (83%) of who finished the study completed the end-of-study
18 participants while on the quadpill compared with acceptability questionnaire, with all reporting the study
seven (39%) of 18 while on placebo (RR 2·14, 95% CI medication was either very easy (n=13) or easy (n=5) to
1·25–3·65; p=0·0053). swallow. Moreover, all 18 participants reported it was
Tests for both a carry-over effect (p=0·868) and a period either very likely (n=10) or likely (n=8) they would take
effect (p=0·308) were not significant. There were no the quadpill if available for use.
www.thelancet.com Vol 389 March 11, 2017 1039
Articles
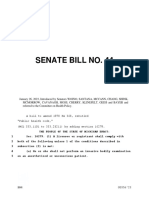
Number of Trials Participants Reduction in diastolic blood pressure Reduction in systolic blood pressure
drugs at (mm Hg) (95% CI) (mm Hg) (95% CI)
quarter-dose
One 36 4721 2·4 (1·9–2·8) 4·7 (3·9–5·4)
Two 6 312 4·4 (3·3–5·5) 6·7 (4·8–8·6)
Three 0 0 n/a n/a
Four 1 18 13·1 (8·9–17·3) 22·4 (16·5–28·3)
20 10 0 25·0 12·5 0
Favours quarter-dose Favours placebo Favours quarter-dose Favours placebo
Figure 3: Efficacy of combination therapy with one, two, three, and four drugs at quarter-dose on blood pressure-lowering, compared with placebo
Data for one and two drugs at quarter-dose are from the systematic review. Data for four drugs at quarter-dose are from the trial reported here. No data were
available for three drugs at quarter-dose (n/a).
There were no serious adverse events and no patients 19/14 mm Hg and achieved an office blood pressure less
had a prespecified adverse event. One participant than 140/90 mm Hg in all participants. When large
reported dizziness while on the quadpill, causing effects are seen in small trials, it is especially important
temporary discontinuation of treatment, and one to review in the context of past evidence; our systematic
reported increased urinary frequency in quadpill and review findings and those of previous similar trials14,15 are
placebo periods, which were judged related or possibly consistent with our finding of a large benefit with
related to study treatment (table 3). minimum side-effects.
Mean heart rate was lower with the quadpill treatment As far as we are aware, our findings are the first
than with placebo, with a difference between groups of placebo-corrected results showing the full effects of
6·5 beats per minute (95% CI 2·3–10·6). There was a four drugs at quarter-dose. Together with our systematic
difference between the quadpill and placebo with respect review finding that one or two drugs at quarter-dose
to changes in creatinine (4·4 mmol/L, 95% CI 0·9–7·8; produces no increase in side-effects compared with
p=0.02), urate (0·03 mmol/L, 0·01–0·04; p=0·003), and placebo—our clinical trial findings suggest considerable
glucose (0·2 mmol/L, 0·02–0·4; p=0·04), but no patient potential advantages for a single capsule containing
had more than a 12% increase in any variable multiple blood pressure-lowering drugs at ultra-low
(appendix p 13). Levels of alanine aminotransferase, dose. A major novel feature of the proposed quadpill
aspartate aminotransferase, sodium, potassium, total approach is the theoretical advantage of initiating therapy
cholesterol, or LDL-cholesterol did not differ between the with a highly effective and tolerable combination versus
quadpill and placebo. starting with fewer agents and titrating up (which in
In the systematic review, 36 trials (4721 participants) practice is rarely done well). Thus, initiation of
were identified that reported the efficacy of one blood combination therapy at very low doses might, for a
pressure-lowering drug at quarter-dose compared worthwhile proportion of patients, achieve the blood
with placebo (appendix pp 7–11). Pooling these data, pressure targets seen in SPRINT16,17 without the multiple
quarter-dose blood pressure-lowering drugs reduced titration steps. However, as yet, there is no direct head-to-
systolic blood pressure by 4·7 mm Hg (95% CI 3·9–5·4) head evidence for the quadpill approach being better
and diastolic blood pressure by 2·4 mm Hg (1·9–2·8; than that used currently, and comparison of the quadpill
figure 3). Adverse events were reported in 14 of these with existing stepped-care approaches is required in
trials (n=1838), with no increase noted in adverse events randomised clinical trials.
for one drug at quarter-dose compared with placebo (RR The main limitations of our trial are the small sample
1·0, 95% CI 0·88–1·10). Furthermore, six trials (n=312) size, short follow-up, and minimum power to assess side-
were identified in which two drugs at quarter-dose were effects. A major barrier to recruitment was identifying
compared with placebo. The pooled reduction in systolic untreated individuals with elevated blood pressure within
and diastolic blood pressure was 6·7 mm Hg (95% CI the settings in which we work. The trial did not aim to
4·8–8·6) and 4·4 mm Hg (3·3–5·5), respectively. No assess the contributions of each component or the
increase in side-effects was noted with two drugs at comparison with other strategies. One further issue is the
quarter-dose compared with placebo (RR 0·93, 95% CI definition of quarter-dose. The strengths of our study
0·29–2·9). No trials of three or four drugs at quarter-dose include the crossover design and use of ambulatory blood
versus placebo were identified in the systematic review. pressure monitoring, hence maximising statistical power,
and the use of randomisation and placebo control to
Discussion minimise bias.
Our trial findings show that a capsule containing four We recorded significant increases in creatinine, urate,
blood pressure-lowering drugs each at quarter-dose and glucose in our study, although no patient had more
reduced 24-h ambulatory blood pressure by roughly than a 12% increase in any measure. There were no
1040 www.thelancet.com Vol 389 March 11, 2017
Articles
longer term follow-up data and any clinical implications titration, which is rarely completed in practice. A quadpill
are uncertain. The small increases in urate are consistent also addresses the individual variation in responsiveness
with previous dose-response analyses for effects of to different agents through provision of a combination
hydrochlorthiazide18 and observations with respect to with a range of modes of action. Improved adherence is
glucose and atenolol.19 Lower systemic pressure can also likely as a result of both decreased pill burden31 and
reduce glomerular perfusion pressure and lead to longer use of lower doses to minimise side-effects.8
term renal benefits for people with raised intraglomerular In summary, our study is the first placebo-controlled
pressure and proteinuria.20–23 However, trials have also trial to indicate that quarter-dose four-drug combination
shown an increase in adverse renal outcomes with therapy could be efficacious in lowering blood pressure.
intensive blood pressure lowering.7,24,25 Long-term It presents a novel approach that could achieve
randomised data are required to determine the clinical substantially greater blood pressure control with a single
implications of the creatinine differences observed in pill, which could have widespread clinical applicability.
this study. Further trials are required to assess contributions of
There has been one previous trial of four-drug different components, and the long-term efficacy and
quarter-dose blood pressure lowering, involving safety in a broader population, both for initial treatment
110 untreated individuals with blood pressure greater and among patients with inadequate control or side-
than 140/90 mm Hg.14 In that trial, a 26/15 mm Hg effects while receiving monotherapy.
reduction was recorded in blood pressure, from a Contributors
baseline of 160/96 mm Hg, with therapy comprising CKC is the chief investigator of the clinical trial, led the writing of the
amlodipine 1·25 mg, atenolol 12·5 mg, bendro protocol and successful funding application, supervised JT, and drafted
the report. JT is a PhD student who primarily implemented the trial
flumethiazide 0·625 mg, and captopril 50 mg. That trial protocol. AB, MB, and TU supported trial recruitment. KV ran all
was unable to estimate a placebo-corrected reduction in statistical analysis, supervised by KR, who was the primary writer of the
blood pressure but did report significantly greater statistical analysis plan. CKC, AR, and GH contributed to trial design.
reductions with the four-drug quarter-dose therapy than AR and CKC had the idea for the trial. AB drafted the protocol and data
collection forms for the systematic review, did the search, data
those seen with each mono therapy at standard dose. abstraction, and data checking as first reviewer, led the statistical
Compared with individual agents, the combination analysis, and drafted the systematic review report. CKC contributed to
showed a greater systolic blood pressure reduction than the idea for the systematic review, revision of the protocol, and review of
amlodipine (8 mm Hg, 95% CI 1–14), atenolol (9 mm Hg, data analyses. MC contributed to the literature search, trial
identification, data abstraction, and data checking as second reviewer,
2–16), bendroflumethiazide (11 mm Hg, 4–18), and and reviewed data analyses. H-MD contributed to data checking as
captopril (7 mm Hg, 1–14). In that trial, no side-effects second reviewer, and review of data analyses. EA assisted with data
were reported in the quadpill group and the only checking and analysis. AR had the idea for the systematic review and
two withdrawals were in the atenolol group. The only supervised research staff working on the project. RW, AS, AP, BN, DP,
HK, JT, JC, MN, CMR, GH, MW, SH, and ST contributed to review of
other trial to date of low-dose antihypertensive therapy the protocol and data analyses. All authors contributed to critical review
with more than two agents assessed three-drug half-dose of this report.
therapy versus placebo in a crossover trial and showed a Declaration of interests
similarly large blood pressure reduction of 18/10 mm Hg CKC is supported by a National Health and Medical Research Council
(p<0·001).15 The placebo-corrected reduction with one- (NHMRC) Career Development Fellowship, co-funded by a National
Heart Foundation Future Leader Fellowship and the Sydney Medical
drug and two-drug standard-dose therapy at similar
Foundation. BN reports grants for a clinical trial from Abbvie,
blood pressure levels is around 9/5 mm Hg and Dr Reddy’s Laboratories, Jannsen, Merck Schering-Plough, and Roche;
17/9 mm Hg, respectively.26 speaking fees from Abbott, Novartis, Pfizer, Roche, and Servier; travel
Poor blood pressure control is a global problem.4,27 fees from Janssen, Roche, and Servier; fees for advisory board
membership from Janssen; is Chair of the Steering Committee for
Initiating treatment with two-drug combination therapy
two ongoing large-scale trials of an SGLT2 inhibitor and member of
has been advocated28 as a more effective means to achieve the Steering Committee for a third; and is supported by an NHMRC
blood pressure control rapidly and with fewer clinic Principal Research Fellowship; all outside the submitted work. All
visits.29 Our study draws on the same underlying honoraria and travel fees are paid to BN’s institution, not as personal
fees. JC reports research grants and honoraria from Servier for the
principles but extends the idea further to initiating
ADVANCE trial, outside the submitted work. AP was supported by a
treatment with multiple ultra-low-dose agents in a single Senior Research Fellowship and Program Grant from NHMRC, during
capsule.30 By comparison with existing approaches to the conduct of the study. DP reports grants from NHMRC, the
blood pressure-lowering therapy, administration of a National Heart Foundation of Australia, and University of Sydney,
during the conduct of the study. ST reports personal fees from Amgen,
single quadruple combination capsule is likely to achieve Lilly, Pfizer, and Sanofi, outside the context of the submitted work; and
more blood pressure-lowering than up-titrating acknowledges support by the UK National Institute of Health Research
monotherapy, since doubling the dose for blood pressure (NIHR) Biomedical Research Centre at Imperial College Healthcare
drugs from half-dose or from standard dose provides NHS Trust and Imperial College London. MW reports consultant fees
from Amgen, outside the submitted work. George Health Enterprises,
only about 1–2 mm Hg further reduction in systolic or the social enterprise arm of The George Institute for Global Health,
diastolic blood pressure.8 Moreover, a quadpill approach has applied for patents in this research area, on which CKC and AR
could address treatment inertia related to the clinician are named as inventors; George Health Enterprises has also received
and patient because it reduces the reliance on stepped investment to develop fixed-dose combinations containing aspirin,
www.thelancet.com Vol 389 March 11, 2017 1041
Articles
statins, and blood pressure-lowering drugs. AB, JT, GH, MB, TU, KV, 14 Mahmud A, Feely J. Low-dose quadruple antihypertensive
KR, EA, RW, MC, H-MD, AS, HK, MN, CMR, and SH declare no combination: more efficacious than individual agents: a preliminary
competing interests. report. Hypertension 2007; 49: 272–75.
15 Wald DS, Morris JK, Wald NJ. Randomized Polypill crossover trial
Acknowledgments in people aged 50 and over. PLoS One 2012; 7: e41297.
The Quadpill study was supported by a Vanguard Grant and
16 Wright JT Jr, Whelton PK, Reboussin DM. A randomized trial of
Ross Hohnen prize from the National Heart Foundation of Australia intensive versus standard blood-pressure control. N Engl J Med
(grant number 100227), University of Sydney Bridging Grant, and 2016; 374: 2294.
National Health and Medical Research Council of Australia (NHMRC) 17 Drawz PE, Pajewski NM, Bates JT, et al, for the SPRINT Study
programme grant. We thank the general practitioners who referred Research Group. Effect of intensive versus standard clinic-based
patients to the trial (Nicholas Bennett, Yvette Castellano, and hypertension management on ambulatory blood pressure: results
Christopher Davis); all participants; Peter Rushton, Yvonne Stanford, from the SPRINT (Systolic Blood Pressure Intervention Trial)
and other staff at Kildare Road Medical Centre; and project staff, ambulatory blood pressure study. Hypertension 2017; 69: 42–50.
Elizabeth Knight, Helen Monaghan, Laurent Billot (chair of Data 18 Peterzan MA, Hardy R, Chaturvedi N, Hughes AD. Meta-analysis of
Monitoring and Safety Committee), Craig Rogers (Pharmaceutical dose-response relationships for hydrochlorothiazide,
Packaging Professionals), and Nick Karrasch (Trialfacts). chlorthalidone, and bendroflumethiazide on blood pressure, serum
potassium, and urate. Hypertension 2012; 59: 1104–09.
References 19 Chang SW, Gong Y, McDonough CW, et al. Melatonin pathway and
1 Lim SS, Vos T, Flaxman AD, et al. A comparative risk assessment of atenolol-related glucose dysregulation: is there a correlation?
burden of disease and injury attributable to 67 risk factors and risk Clin Transl Sci 2016; 9: 114–22.
factor clusters in 21 regions, 1990–2010: a systematic analysis for
the Global Burden of Disease Study 2010. Lancet 2012; 380: 2224–60. 20 Wright JT Jr, Bakris G, Greene T, et al. Effect of blood pressure
lowering and antihypertensive drug class on progression of
2 Turnbull F, for the Blood Pressure Lowering Treatment Trialists’ hypertensive kidney disease: results from the AASK trial. JAMA
Collaboration. Effects of different blood-pressure-lowering 2002; 288: 2421–31.
regimens on major cardiovascular events: results of
prospectively-designed overviews of randomised trials. Lancet 2003; 21 Hunsicker LG, Adler S, Caggiula A, et al. Predictors of the
362: 1527–35. progression of renal disease in the Modification of Diet in Renal
Disease Study. Kidney Int 1997; 51: 1908–19.
3 Staessen JA, Wang JG, Thijs L. Cardiovascular protection and blood
pressure reduction: a meta-analysis. Lancet 2001; 358: 1305–15. 22 Lewis EJ, Hunsicker LG, Clarke WR, et al. Renoprotective effect of
the angiotensin-receptor antagonist irbesartan in patients with
4 Chow CK, Teo KK, Rangarajan S, et al. Prevalence, awareness, nephropathy due to type 2 diabetes. N Engl J Med 2001; 345: 851–60.
treatment, and control of hypertension in rural and urban
communities in high-, middle-, and low-income countries. JAMA 23 Keane WF, Brenner BM, de Zeeuw D, et al. The risk of developing
2013; 310: 959–68. end-stage renal disease in patients with type 2 diabetes and
nephropathy: the RENAAL study. Kidney Int 2003; 63: 1499–507.
5 Wald DS, Law M, Morris JK, Bestwick JP, Wald NJ.
Combination therapy versus monotherapy in reducing blood 24 Peralta CA, McClure LA, Scherzer R, et al. Effect of intensive versus
pressure: meta-analysis on 11,000 participants from 42 trials. usual blood pressure control on kidney function among individuals
Am J Med 2009; 122: 290–300. with prior lacunar stroke: a post hoc analysis of the Secondary
Prevention of Small Subcortical Strokes (SPS3) randomized trial.
6 Xie X, Atkins E, Lv J, et al. Effects of intensive blood pressure Circulation 2016; 133: 584–91.
lowering on cardiovascular and renal outcomes: updated systematic
review and meta-analysis. Lancet 2016; 387: 435–43. 25 Cushman WC, Evans GW, Byington RP, et al. Effects of intensive
blood-pressure control in type 2 diabetes mellitus. N Engl J Med
7 Wright JT Jr, Williamson JD, Whelton PK, et al. A randomized trial 2010; 362: 1575–85.
of intensive versus standard blood-pressure control. N Engl J Med
2015; 373: 2103–16. 26 Law MR, Morris JK, Wald NJ. Use of blood pressure lowering drugs
in the prevention of cardiovascular disease: meta-analysis of
8 Law MR, Wald NJ, Morris JK, Jordan RE. Value of low dose 147 randomised trials in the context of expectations from
combination treatment with blood pressure lowering drugs: prospective epidemiological studies. BMJ 2009; 338: b1665.
analysis of 354 randomised trials. BMJ 2003; 326: 1427.
27 Sever PS, Messerli FH. Hypertension management 2011: optimal
9 Brayfield A. Martindale: the complete drug reference. combination therapy. Eur Heart J 2011; 32: 2499–506.
http://www.pharmpress.com/product/MC_MART/
martindale-the-complete-drug-reference (accessed Jan 18, 2017). 28 Byrd JB, Zeng C, Tavel HM, et al. Combination therapy as initial
treatment for newly diagnosed hypertension. Am Heart J 2011;
10 MIMS. Monthly index of medical specialties. http://www.mims. 162: 340–46.
com/resources/portal/common/document/mims/mimsau.htm
(accessed Nov 17, 2016). 29 Feldman RD, Zou GY, Vandervoort MK, Wong CJ, Nelson SA,
Feagan BG. A simplified approach to the treatment of uncomplicated
11 National Heart Foundation of Australia. Guide to management of hypertension: a cluster randomized, controlled trial. Hypertension
hypertension 2008: assessing and managing raised blood pressure 2009; 53: 646–53.
in adults—updated December, 2010. https://heartfoundation.org.
au/images/uploads/publications/ 30 Salam A, Webster R, Singh K, et al. TRIple pill vs Usual care
HypertensionGuidelines2008to2010Update.pdf (accessed Management for Patients with mild-to-moderate Hypertension
Jan 18, 2017). (TRIUMPH): study protocol. Am Heart J 2014; 167: 127–32.
12 Kenward MG, Roger JH. The use of baseline covariates in crossover 31 Webster R, Patel A, Selak V, et al. Effectiveness of fixed dose
studies. Biostatistics 2010; 11: 1–17. combination medication (“polypills”) compared with usual care in
patients with cardiovascular disease or at high risk: a prospective,
13 Kenward MG, Roger JH. An improved approximation to the individual patient data meta-analysis of 3140 patients in
precision of fixed effects from restricted maximum likelihood. six countries. Int J Cardiol 2016; 205: 147–56.
Comput Stat Data Anal 2009; 53: 2583–95.
1042 www.thelancet.com Vol 389 March 11, 2017
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- 51 Firefighter Interview QuestionsDocument17 pages51 Firefighter Interview QuestionsMa Jamie Lhen100% (1)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Disability EvaluationDocument11 pagesDisability Evaluationramhariphysio63% (8)
- Las Peh 2Document3 pagesLas Peh 2Paul Vincent LauretaNo ratings yet
- PRC Case Form Midwifery NEWDocument4 pagesPRC Case Form Midwifery NEWسانو روديل88% (41)
- Tips For Passing NclexDocument2 pagesTips For Passing NclexNimraj PatelNo ratings yet
- 06. ĐỀ THI VÀO LỚP 10-ĐỒNG NAI (2020-2021)Document8 pages06. ĐỀ THI VÀO LỚP 10-ĐỒNG NAI (2020-2021)hoa phamNo ratings yet
- Great Eastern Life - Confidential Medical Certificate (Other Illnesses) - CLMLAMCODocument2 pagesGreat Eastern Life - Confidential Medical Certificate (Other Illnesses) - CLMLAMCOsimpoonNo ratings yet
- The Complete Tattoo Bible Pt1Document50 pagesThe Complete Tattoo Bible Pt1bhatiagaganNo ratings yet
- Metabolic Syndrome DiseasesDocument8 pagesMetabolic Syndrome DiseasesMahmoud SelimNo ratings yet
- Module 3Document3 pagesModule 3Charles JoseNo ratings yet
- Chakra Mantra MagickDocument36 pagesChakra Mantra MagickPaul Asturbiaris100% (4)
- Maternal Child Nutrition - 2013 - Pelletier - The Principles and Practices of Nutrition Advocacy Evidence ExperienceDocument18 pagesMaternal Child Nutrition - 2013 - Pelletier - The Principles and Practices of Nutrition Advocacy Evidence ExperienceCatarina MaguniNo ratings yet
- B. Jungian Psychology and Its Archetypal InsightsDocument6 pagesB. Jungian Psychology and Its Archetypal InsightskatburnerNo ratings yet
- Access Florida Application Details 657074801Document5 pagesAccess Florida Application Details 657074801Norman AndrewsNo ratings yet
- Coles Medical Practice in New Zealand 2013 PDFDocument260 pagesColes Medical Practice in New Zealand 2013 PDFgus_lionsNo ratings yet
- Pharmacokinetic and Pharmacodynamic Profile of EmpagliflozinDocument13 pagesPharmacokinetic and Pharmacodynamic Profile of EmpagliflozinRajah HadiNo ratings yet
- Beige Simple Student Internship Resume PDFDocument3 pagesBeige Simple Student Internship Resume PDFZorica JerotijevicNo ratings yet
- Vitality Book (1606456525)Document57 pagesVitality Book (1606456525)Ritu ShewaniNo ratings yet
- Forklift ForkDocument10 pagesForklift ForkDiah Novita SariNo ratings yet
- Michigan Senate Bill 0044 (2023)Document2 pagesMichigan Senate Bill 0044 (2023)WDIV/ClickOnDetroitNo ratings yet
- Raw Q3 Las 1Document15 pagesRaw Q3 Las 1Abegail CastilloNo ratings yet
- 2022 CHAI HIV Market Report 12.8.22Document45 pages2022 CHAI HIV Market Report 12.8.22Rakesh KumarNo ratings yet
- Adlerian PPTS&TDocument20 pagesAdlerian PPTS&TPamela joyce c. santosNo ratings yet
- Definition of Counselling Training ProgramDocument2 pagesDefinition of Counselling Training ProgramAdrienne AumanNo ratings yet
- Crime Preventive MeasuresDocument3 pagesCrime Preventive MeasuresNumra AttiqNo ratings yet
- Adrenal Gland DisordersDocument5 pagesAdrenal Gland Disordersdujana rastanawiNo ratings yet
- How To Improve Clinical Pharmacy Practice Using Key Performance IndicatorsDocument5 pagesHow To Improve Clinical Pharmacy Practice Using Key Performance IndicatorsTaufik Qur RaufNo ratings yet
- Case Study FormatDocument29 pagesCase Study FormatPradip ChougaleNo ratings yet
- DPR - Project Location and FacilitiesDocument2 pagesDPR - Project Location and FacilitiesRAKSHITH M SNo ratings yet
- New PE11-Q3-M1-The-Role-of-Physical-Activity-Assessment-in-Managing-Ones-StressDocument12 pagesNew PE11-Q3-M1-The-Role-of-Physical-Activity-Assessment-in-Managing-Ones-StressMary Ann LomboyNo ratings yet