You might also like
- Technical Standards and Guidelines For The Diagnosis of Biotinidase DeficiencyDocument7 pagesTechnical Standards and Guidelines For The Diagnosis of Biotinidase DeficiencySaad KhanNo ratings yet
- Absolute Final Biotinidase OptimizationDocument7 pagesAbsolute Final Biotinidase OptimizationSaad KhanNo ratings yet
- Biophysical Methods for Biotherapeutics: Discovery and Development ApplicationsFrom EverandBiophysical Methods for Biotherapeutics: Discovery and Development ApplicationsTapan K. DasNo ratings yet
- Bala Blood Report Ca, Uric, B12, D3Document3 pagesBala Blood Report Ca, Uric, B12, D3BALANo ratings yet
- Laboratory Test Report: Test Name Result Biological Reference Interval PotassiumDocument2 pagesLaboratory Test Report: Test Name Result Biological Reference Interval PotassiumGangapuram SrikanthNo ratings yet
- Department of Biochemistry Campaign Diabetic Panel: Test Name Result Unit Bio. Ref. Range MethodDocument4 pagesDepartment of Biochemistry Campaign Diabetic Panel: Test Name Result Unit Bio. Ref. Range Methodgsm2008No ratings yet
- Seema 1Document4 pagesSeema 1reenajanjadiaNo ratings yet
- 1-Liver Function Test - PO3921596584-773 - 230517 - 125136Document4 pages1-Liver Function Test - PO3921596584-773 - 230517 - 125136Moksh GujjarNo ratings yet
- Department of Biochemistry Test Name Result Unit Bio. Ref. Interval MethodDocument2 pagesDepartment of Biochemistry Test Name Result Unit Bio. Ref. Interval MethodBapan ChakrabortyNo ratings yet
- Nisha DeviDocument2 pagesNisha DeviSantan Lal DasNo ratings yet
- S62 - Lpl-Nagpur - 2 Plot No. 7, Ground Floor Hotel Sunny Int Besides Gujrati Samaj Bhavan, Dhantoli Nagpur 440012Document2 pagesS62 - Lpl-Nagpur - 2 Plot No. 7, Ground Floor Hotel Sunny Int Besides Gujrati Samaj Bhavan, Dhantoli Nagpur 440012prachi jaiswalNo ratings yet
- Biotin and Other Interferences in Immunoassays: A Concise GuideFrom EverandBiotin and Other Interferences in Immunoassays: A Concise GuideNo ratings yet
- LFT (Liver Function Test) : Biological Reference Results Units Test NameDocument4 pagesLFT (Liver Function Test) : Biological Reference Results Units Test Namemetepraju0210No ratings yet
- SRL Format 2Document1 pageSRL Format 2haroon012023No ratings yet
- EGAC0401Document5 pagesEGAC0401bhanuprasadbkNo ratings yet
- Laboratory Test Report: Test Name Result Biological Reference Interval TSH UltrasensitiveDocument5 pagesLaboratory Test Report: Test Name Result Biological Reference Interval TSH UltrasensitiveP Nagaraju RajuNo ratings yet
- Blood Tests ReportDocument7 pagesBlood Tests ReportLalith GoudNo ratings yet
- Uric Acid (Ua) Test Name Observed Values Units Biological Reference Intervals Uric Acid 10.5Document1 pageUric Acid (Ua) Test Name Observed Values Units Biological Reference Intervals Uric Acid 10.5seravanakumarNo ratings yet
- Biotinidase Deficiency ProposalDocument7 pagesBiotinidase Deficiency ProposalFaryalBalochNo ratings yet
- Final: Patient Name: Dummy 0002UG999999Document1 pageFinal: Patient Name: Dummy 0002UG999999abhimanyu kumarNo ratings yet
- Pharmacokinetics BiotinaDocument10 pagesPharmacokinetics BiotinaneofherNo ratings yet
- Laboratory Test Report: Test Name Result Biological Reference Interval Fasting Plasma GlucoseDocument3 pagesLaboratory Test Report: Test Name Result Biological Reference Interval Fasting Plasma Glucosemasood syedNo ratings yet
- Uric Acid PDFDocument1 pageUric Acid PDFPulkit TalujaNo ratings yet
- Adipose Tissue in Health and DiseaseFrom EverandAdipose Tissue in Health and DiseaseTodd LeffNo ratings yet
- Report 516ce2e4Document6 pagesReport 516ce2e4Samruddhi RathiNo ratings yet
- Parameter Result Unit Biological Ref. Interval: Westergren (Manual)Document2 pagesParameter Result Unit Biological Ref. Interval: Westergren (Manual)Ashish RanjanNo ratings yet
- Diagnostic Report: FinalDocument1 pageDiagnostic Report: FinalAashyNo ratings yet
- Report GNDocument3 pagesReport GNPawan MadhesiyaNo ratings yet
- Department of Biochemistry Campaign Diabetic Check (With PP)Document2 pagesDepartment of Biochemistry Campaign Diabetic Check (With PP)gsm2008No ratings yet
- 370 FullDocument1 page370 FulllorenadelherNo ratings yet
- Patient Profile FormDocument8 pagesPatient Profile FormShaRath KmNo ratings yet
- FTMREPORTDocument1 pageFTMREPORTMAYANK tecnooNo ratings yet
- 1-Frequent Pain Check Profile - PO2526765603-393Document8 pages1-Frequent Pain Check Profile - PO2526765603-393Satyendra SharmaNo ratings yet
- Ravinder Puri C-1Document14 pagesRavinder Puri C-1TasmiyaNo ratings yet
- Unlq6073 PDFDocument8 pagesUnlq6073 PDFSrinu VijayaNo ratings yet
- Biochemistry: Investigation Observed Value Unit Biological Reference IntervalDocument15 pagesBiochemistry: Investigation Observed Value Unit Biological Reference IntervalAshutoshNo ratings yet
- CpeptideDocument1 pageCpeptiderajanarora72No ratings yet
- Individual Variant Interpretation For Pathogenic MutationDocument3 pagesIndividual Variant Interpretation For Pathogenic MutationSukh SukhiNo ratings yet
- Intended Use: Form Catalog NoDocument6 pagesIntended Use: Form Catalog NoRafika RaraNo ratings yet
- Laboratory Test Report: 19 Years / FemaleDocument3 pagesLaboratory Test Report: 19 Years / Femalesneha sahaNo ratings yet
- For Success N Access 1022168537 - DBVE8685Document10 pagesFor Success N Access 1022168537 - DBVE8685vanam tejasviNo ratings yet
- Jasveen 2Document2 pagesJasveen 2rababkr23No ratings yet
- Blood TestDocument2 pagesBlood TestAll You NeedNo ratings yet
- Final: Patient Name: Dummy 0002UG999999Document1 pageFinal: Patient Name: Dummy 0002UG999999Sanket GuptaNo ratings yet
- Health ProfileDocument18 pagesHealth ProfileSahil HussainNo ratings yet
- Jinnah Central Lab: Jinnah Hospital & AIMC Lahore, PakistanDocument2 pagesJinnah Central Lab: Jinnah Hospital & AIMC Lahore, Pakistanafshan liaqatNo ratings yet
- HeaderDocument2 pagesHeader22sa010259No ratings yet
- Inborn Errors of Metabolism (Iem) Summary Report: Sr. No. Test Methodology Result Test TypeDocument2 pagesInborn Errors of Metabolism (Iem) Summary Report: Sr. No. Test Methodology Result Test TypeMallikharjunaRao medaNo ratings yet
- Applications of ZymographyDocument25 pagesApplications of ZymographyXênia SoutoNo ratings yet
- Optimasi Teknik Western Blot Untuk Deteksi Ekspresi Protein Tanaman Padi (Oryza Sativa L.)Document11 pagesOptimasi Teknik Western Blot Untuk Deteksi Ekspresi Protein Tanaman Padi (Oryza Sativa L.)Refhany AfidhaNo ratings yet
- WPPW9722Document3 pagesWPPW9722akumar_948771No ratings yet
- LFT ReportDocument3 pagesLFT Reportacer.tsk007No ratings yet
- This Is An Electronic Report & Not: To Be Used For Any Legal PurposesDocument1 pageThis Is An Electronic Report & Not: To Be Used For Any Legal PurposesTauseef Taj KianiNo ratings yet
- Patient Name: Kunjamma KUNJF1207544155: FinalDocument5 pagesPatient Name: Kunjamma KUNJF1207544155: FinalPranay BhosaleNo ratings yet
- XIJU5502Document3 pagesXIJU5502Praveen ReddyNo ratings yet
- Jaswanth Redddy Sappp PDFDocument1 pageJaswanth Redddy Sappp PDFAnonymous VT75a3QNo ratings yet
- File PDFDocument1 pageFile PDFSabari PramanikNo ratings yet
- Pathology 22.04.2020 02.45.42.368Document3 pagesPathology 22.04.2020 02.45.42.368Small WondersNo ratings yet
- ReportDocument3 pagesReportPawan MadhesiyaNo ratings yet
- Kit InsertDocument11 pagesKit InsertSaad KhanNo ratings yet
- Elisa: Enzyme-Linked Immunosorbent Assay: Syed Muhammad Khan Bshons. ZoologyDocument47 pagesElisa: Enzyme-Linked Immunosorbent Assay: Syed Muhammad Khan Bshons. ZoologySaad KhanNo ratings yet
- Minerals: Trace ElementsDocument182 pagesMinerals: Trace ElementsSaad KhanNo ratings yet
- The Aga Khan Hospital and Medical College, Karachi.: ConfidentialDocument1 pageThe Aga Khan Hospital and Medical College, Karachi.: ConfidentialSaad KhanNo ratings yet
- CH205 Atomic Absorption SpectrosDocument30 pagesCH205 Atomic Absorption SpectrosSaad KhanNo ratings yet
- MTI (Path) : Medical Training Initiative in PathologyDocument18 pagesMTI (Path) : Medical Training Initiative in PathologySaad KhanNo ratings yet
- eMRCS Pathology 326 MCQsDocument101 pageseMRCS Pathology 326 MCQsSaad KhanNo ratings yet
- Documents To Support Your Application: MTI (Path) Medical Training Initiative in PathologyDocument2 pagesDocuments To Support Your Application: MTI (Path) Medical Training Initiative in PathologySaad KhanNo ratings yet
- Hepatitis C: DR Nosheen ZaidiDocument63 pagesHepatitis C: DR Nosheen ZaidiSaad KhanNo ratings yet
- DR Sarfraz Notes (Contoversial With Explanation)Document16 pagesDR Sarfraz Notes (Contoversial With Explanation)Saad KhanNo ratings yet
- Kaplan: Clinical Chemistry, 5 Edition: Clinical References - Methods of AnalysisDocument9 pagesKaplan: Clinical Chemistry, 5 Edition: Clinical References - Methods of AnalysisSaad KhanNo ratings yet
- FCPS PART 1 Study MaterialDocument1 pageFCPS PART 1 Study MaterialSaad Khan100% (1)
- eMRCS Pathology 326 MCQsDocument101 pageseMRCS Pathology 326 MCQsSaad KhanNo ratings yet
- Biotinidase Deficiency QuestionnereDocument1 pageBiotinidase Deficiency QuestionnereSaad KhanNo ratings yet
- Optimization of Biotinidase Assay: Dr. Faryal Husnain Resident Clinical ChemistryDocument22 pagesOptimization of Biotinidase Assay: Dr. Faryal Husnain Resident Clinical ChemistrySaad KhanNo ratings yet
- eMRCS Microbiology 19 QuestionsDocument7 pageseMRCS Microbiology 19 QuestionsSaad KhanNo ratings yet
- Excellent Important Pearls of Fcps Part1 Collection of Different Important PointsDocument18 pagesExcellent Important Pearls of Fcps Part1 Collection of Different Important PointsSaad KhanNo ratings yet
- Chromosomal MutationsDocument19 pagesChromosomal MutationsJanet BarcimoNo ratings yet
- Chromosomal Abnormalities: AP BiologyDocument28 pagesChromosomal Abnormalities: AP BiologySuzy BaeNo ratings yet
- How To Interpret A KaryotypeDocument2 pagesHow To Interpret A KaryotypeLiberty NguyenNo ratings yet
- Karyotypes and Chromo Disorders NotesDocument19 pagesKaryotypes and Chromo Disorders NotesLester ParadilloNo ratings yet
- Chromosomal AbnormalitiesDocument27 pagesChromosomal Abnormalitiessapu-98No ratings yet
- The Ishihara Color Test For Color BlindnessDocument13 pagesThe Ishihara Color Test For Color Blindnesslensi tirta tri buana100% (1)
- Recurrent Abortions and Chromosomal Defects - Edited 1 - Chrysantine ParamayudaDocument10 pagesRecurrent Abortions and Chromosomal Defects - Edited 1 - Chrysantine ParamayudaEndrianus Jaya PutraNo ratings yet
- Supplementary Information To Chapter 32: Inborn Errors of Metabolism General ConsiderationsDocument24 pagesSupplementary Information To Chapter 32: Inborn Errors of Metabolism General ConsiderationsAaron JoseNo ratings yet
- Neuromuscular Disorders in Childhood: Professor Kevin Dunne Department of Paediatrics RcsiDocument30 pagesNeuromuscular Disorders in Childhood: Professor Kevin Dunne Department of Paediatrics RcsiIbrahimNo ratings yet
- Pedigree Worksheet Answer KeyDocument1 pagePedigree Worksheet Answer Keyapi-477608730100% (8)
- 3 - PorphyriasDocument14 pages3 - PorphyriasHamzehNo ratings yet
- Data Perbaikan Peserta KSN-K 2021: No Nama - Peserta NisnDocument10 pagesData Perbaikan Peserta KSN-K 2021: No Nama - Peserta NisnRianty LstNo ratings yet
- Clinical - Approach - To - The - Diagnosis IEM PDFDocument15 pagesClinical - Approach - To - The - Diagnosis IEM PDFVictor Lage de AraujoNo ratings yet
- Chromosomal DisordersDocument17 pagesChromosomal DisordersJosh Rosenberg100% (1)
- ThalassemiaDocument10 pagesThalassemiaAmanda Scarlet100% (1)
- Errors in Meiosis QuizDocument3 pagesErrors in Meiosis QuizLorena ariateNo ratings yet
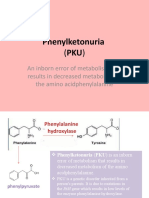
- Phenylketonuria: An Inborn Error of Metabolism That Results in Decreased Metabolism of The Amino AcidphenylalanineDocument8 pagesPhenylketonuria: An Inborn Error of Metabolism That Results in Decreased Metabolism of The Amino Acidphenylalanineელენე ბუჩუკურიNo ratings yet
- Sindrome de DownDocument27 pagesSindrome de DownKhissi BArzaNo ratings yet
- Case Study - Muscular DystrophyDocument18 pagesCase Study - Muscular DystrophyJohn Rey BayoguingNo ratings yet
- Ukg Asahan - ExcelDocument124 pagesUkg Asahan - ExcelSutantoNo ratings yet
- Duchenne and Becker Muscular DystrophyDocument8 pagesDuchenne and Becker Muscular DystrophyRumela Ganguly ChakrabortyNo ratings yet
- Autosomal Recessive DisorderDocument17 pagesAutosomal Recessive DisorderAndrea Love PalomoNo ratings yet
- Muscular DystrophyDocument14 pagesMuscular Dystrophyapi-439738433No ratings yet
- Mutations and Genetic Disorders 4Document28 pagesMutations and Genetic Disorders 4MaleehaNo ratings yet
- SDR Hutchinson GilfordDocument22 pagesSDR Hutchinson GilfordVintilă BogdanNo ratings yet
- Babyshield TMS Fact SheetDocument399 pagesBabyshield TMS Fact SheetSunny RockyNo ratings yet
- ALKAPTONURIADocument15 pagesALKAPTONURIAJean Claude Balancio100% (1)
- Daftar Peserta FizDocument39 pagesDaftar Peserta FizFefin IriantiNo ratings yet
- Murder MysteryDocument13 pagesMurder Mysteryapi-451162079No ratings yet
- Cell CycleDocument69 pagesCell CycleJustine FariscalNo ratings yet