You might also like
- Pathophysiology of DM IIDocument6 pagesPathophysiology of DM IIJulie SimaurioNo ratings yet
- Columnar Insulin Dosing Chart : (1 ML 1 Unit)Document1 pageColumnar Insulin Dosing Chart : (1 ML 1 Unit)Philippe KinnaerNo ratings yet
- General and Comparative Endocrinology: Ingrid Van Hoek, Sylvie DaminetDocument11 pagesGeneral and Comparative Endocrinology: Ingrid Van Hoek, Sylvie DaminetNguyễn Tấn TàiNo ratings yet
- Thyroid Hormone Profile in Chronic Kidney DiseaseDocument6 pagesThyroid Hormone Profile in Chronic Kidney DiseaserefaNo ratings yet
- Physiology 19 1 1Document4 pagesPhysiology 19 1 1MehNo ratings yet
- Neonatal Hyperbilirubinemia and Elevated Liver Enzymes Associated With Thyroid Hormone Deficiency in NeonatesDocument4 pagesNeonatal Hyperbilirubinemia and Elevated Liver Enzymes Associated With Thyroid Hormone Deficiency in NeonatesOlfiany Laurenzia PongohNo ratings yet
- Tekin 2012Document4 pagesTekin 2012le.m4rtinezoNo ratings yet
- Syaraf InterDocument7 pagesSyaraf Intersatria utamaNo ratings yet
- Pituitary Hyperplasia Resulting From Primary Hypothyroidism: July 2011Document3 pagesPituitary Hyperplasia Resulting From Primary Hypothyroidism: July 2011VanessaNo ratings yet
- Graves Disease Associated With Severe Hypoalbuminemia: Letter To The Editor Acta Medica AnatoliaDocument2 pagesGraves Disease Associated With Severe Hypoalbuminemia: Letter To The Editor Acta Medica AnatoliaAbdur Rachman Ba'abdullahNo ratings yet
- 10 1002@jbm4 10479Document6 pages10 1002@jbm4 10479Wev LimaNo ratings yet
- Prevalence and Associations of Thyroid Dysfunction With Metabolic Markers Blood Glucose and Lipid Profile: A Cross-Sectional StudyDocument6 pagesPrevalence and Associations of Thyroid Dysfunction With Metabolic Markers Blood Glucose and Lipid Profile: A Cross-Sectional StudyOpenaccess Research paperNo ratings yet
- Austin Journal of Nephrology and HypertensionDocument4 pagesAustin Journal of Nephrology and HypertensionAustin Publishing GroupNo ratings yet
- Research ArticleDocument9 pagesResearch ArticleM RifkiNo ratings yet
- Tatalaksana SOPK Terkini Dan Updated Studi Klinis Untuk SOPKDocument29 pagesTatalaksana SOPK Terkini Dan Updated Studi Klinis Untuk SOPKcirererereNo ratings yet
- Thyroid Dysfunction and Anaemia in A Large Population-Based StudyDocument5 pagesThyroid Dysfunction and Anaemia in A Large Population-Based StudyRaissa Metasari TantoNo ratings yet
- 10.1515@jpem 2013 0302Document3 pages10.1515@jpem 2013 0302drToikNo ratings yet
- Thyroid Status and Renal Function in Older Persons in The General PopulationDocument8 pagesThyroid Status and Renal Function in Older Persons in The General PopulationfefNo ratings yet
- TNF ALPHA in Neuropatia Diabetica Articol 2017Document6 pagesTNF ALPHA in Neuropatia Diabetica Articol 2017Pilat BogdanNo ratings yet
- Methylprednisolone in West SyndromeDocument5 pagesMethylprednisolone in West SyndromeBandya SahooNo ratings yet
- RTH 6Document5 pagesRTH 6Ei DrakorNo ratings yet
- 257 FullDocument8 pages257 Fullsundar_kumar0No ratings yet
- ¿Por Qué La Resistencia A La Insulina Puede Ser Una Consecuencia Natural de La TiroidesDocument10 pages¿Por Qué La Resistencia A La Insulina Puede Ser Una Consecuencia Natural de La TiroidesmagalyNo ratings yet
- BMC Nephrology: Risk Factors For Chronic Kidney Disease in Japan: A Community-Based StudyDocument10 pagesBMC Nephrology: Risk Factors For Chronic Kidney Disease in Japan: A Community-Based StudyYudaAmanikoNo ratings yet
- Hyperuricemia Is Associated With Hypertension, Obesity, and Albuminuria in Children With Chronic Kidney DiseaseDocument5 pagesHyperuricemia Is Associated With Hypertension, Obesity, and Albuminuria in Children With Chronic Kidney DiseaseMuh Husni RifaiNo ratings yet
- 10.1515@jpem 2019 0075Document8 pages10.1515@jpem 2019 0075Ahmed BaghdadiNo ratings yet
- Febuxostat Therapy For Patients With Stage 3 CKD and Asymptomatic Hyperuricemia: A Randomized TrialDocument13 pagesFebuxostat Therapy For Patients With Stage 3 CKD and Asymptomatic Hyperuricemia: A Randomized TrialAndreas AdiwinataNo ratings yet
- 2020 01 NatureRevEndocrinologyDocument3 pages2020 01 NatureRevEndocrinologyPutri RsacNo ratings yet
- Mehran 2017Document9 pagesMehran 2017pelinNo ratings yet
- Androgen Receptor Gene CAG Repeat Length andDocument10 pagesAndrogen Receptor Gene CAG Repeat Length anddouglas 87No ratings yet
- Sehgal 2020Document5 pagesSehgal 2020Mutiara RobbaniiNo ratings yet
- Pe 08044Document4 pagesPe 08044Ro KohnNo ratings yet
- Thyroid DisorderDocument19 pagesThyroid DisorderBudi AthAnza SuhartonoNo ratings yet
- Ebj ArticleDocument5 pagesEbj ArticleAllyana de JesusNo ratings yet
- IJPRBS343Document19 pagesIJPRBS343shaileeshah693No ratings yet
- Disorders of Endocrine SystemDocument48 pagesDisorders of Endocrine SystemSHARIM ASGHARNo ratings yet
- Hearing Loss in Patients Using Isotretinoin: Is It A Side Effect or Due To Hyperlipidemia?Document5 pagesHearing Loss in Patients Using Isotretinoin: Is It A Side Effect or Due To Hyperlipidemia?Ajshe ÇekanNo ratings yet
- Apem 2018 23 1 38Document5 pagesApem 2018 23 1 38Dewi PrasetiaNo ratings yet
- Comprehensive Management of PCOS - GPDocument48 pagesComprehensive Management of PCOS - GPtata maretha100% (1)
- 786 TFT and CKD ThesisDocument9 pages786 TFT and CKD ThesisPrabhat KcNo ratings yet
- Thyroid Hormone Research PaperDocument8 pagesThyroid Hormone Research Paperjtbowtgkf100% (1)
- Etiological Evaluation of Primary Congenital Hypothyroidism CasesDocument7 pagesEtiological Evaluation of Primary Congenital Hypothyroidism CasesEgidiaEkaRikaNo ratings yet
- Nejmra 1901214Document13 pagesNejmra 1901214Alejandra HernandezNo ratings yet
- Bioscientific Review (BSR) : Association of Nephropathy With The Thyroid ProfileDocument10 pagesBioscientific Review (BSR) : Association of Nephropathy With The Thyroid ProfileUMT JournalsNo ratings yet
- SAQ 2nd Week (Thyroid Gland)Document15 pagesSAQ 2nd Week (Thyroid Gland)Josephine BediakoNo ratings yet
- Electrocardiographic Changes in Hypothyroidism - A Cross-Sectional StudyDocument5 pagesElectrocardiographic Changes in Hypothyroidism - A Cross-Sectional Study180045No ratings yet
- International Journal of Chemtech Research: Janani Panneer Selvam, Sethu GunasekaranDocument11 pagesInternational Journal of Chemtech Research: Janani Panneer Selvam, Sethu GunasekaranVishnu04No ratings yet
- Liu2019 Article EvaluationOfSerumFreeFattyAcidDocument9 pagesLiu2019 Article EvaluationOfSerumFreeFattyAcidandreiNo ratings yet
- Pedoman CopdDocument42 pagesPedoman CopddaranhtgNo ratings yet
- Radio-Contrast Agent-Induced Hyperthyroidism: Case Report and Review of The LiteratureDocument3 pagesRadio-Contrast Agent-Induced Hyperthyroidism: Case Report and Review of The LiteratureIwan SaputeraNo ratings yet
- A Case of Idiopathic Intracranial Hypertension Due To Chronic Kidney Disease 2472 100X 1000134Document3 pagesA Case of Idiopathic Intracranial Hypertension Due To Chronic Kidney Disease 2472 100X 1000134Betül SulubulutNo ratings yet
- Turkjmedsci-50-354 PubmedDocument6 pagesTurkjmedsci-50-354 PubmedRizka Uda'aNo ratings yet
- Fitoterapia: Jianfeng Xue, Wenjun Ding, Yan LiuDocument5 pagesFitoterapia: Jianfeng Xue, Wenjun Ding, Yan LiuAamir SohailNo ratings yet
- Fitoterapia: Jianfeng Xue, Wenjun Ding, Yan LiuDocument5 pagesFitoterapia: Jianfeng Xue, Wenjun Ding, Yan LiuAamir SohailNo ratings yet
- Hypercalcemia, An Uncommon Presentation of HyperthyroidismDocument2 pagesHypercalcemia, An Uncommon Presentation of HyperthyroidismJOSE LUIS COTRINA CASTAÑEDANo ratings yet
- Hyperthyroid and Hypothyroid Status Was Strongly Associated With Gout and Weakly Associated With HyperuricaemiaDocument11 pagesHyperthyroid and Hypothyroid Status Was Strongly Associated With Gout and Weakly Associated With Hyperuricaemiasiti hazard aldinaNo ratings yet
- Research Article Curcumin Attenuates Ferroptosis and Ameliorates Erectile Function in Diabetic Rats by Activating Nrf2/HO-1 PathwayDocument13 pagesResearch Article Curcumin Attenuates Ferroptosis and Ameliorates Erectile Function in Diabetic Rats by Activating Nrf2/HO-1 Pathwaymohammed fayedNo ratings yet
- Subacute Thyroiditis Presenting As Acute Psychosis: A Case Report and Literature ReviewDocument5 pagesSubacute Thyroiditis Presenting As Acute Psychosis: A Case Report and Literature ReviewFelixpro DotaNo ratings yet
- Research Article: Prevalence, Predictive Factors, and Characteristics of Osteoporosis in Hyperthyroid PatientsDocument8 pagesResearch Article: Prevalence, Predictive Factors, and Characteristics of Osteoporosis in Hyperthyroid PatientsMutiara DamayantiNo ratings yet
- Research Article: Prevalence, Predictive Factors, and Characteristics of Osteoporosis in Hyperthyroid PatientsDocument8 pagesResearch Article: Prevalence, Predictive Factors, and Characteristics of Osteoporosis in Hyperthyroid PatientsMutiara DamayantiNo ratings yet
- Research Article: Prevalence, Predictive Factors, and Characteristics of Osteoporosis in Hyperthyroid PatientsDocument7 pagesResearch Article: Prevalence, Predictive Factors, and Characteristics of Osteoporosis in Hyperthyroid Patientsdek fafaNo ratings yet
- Key Facts Menstrual CycleDocument8 pagesKey Facts Menstrual CycleMari FeNo ratings yet
- Chemical Coordination and Integration NotesDocument22 pagesChemical Coordination and Integration Notesarshi27khan3057No ratings yet
- 239.mudassar DIABETES, PMDC 3811 PAID, Bushra 4011 Not PaidDocument8 pages239.mudassar DIABETES, PMDC 3811 PAID, Bushra 4011 Not PaidraychandwpNo ratings yet
- Reviewsheet hp04Document4 pagesReviewsheet hp04Jefry AlfarizyNo ratings yet
- Aldosterone Renin RatioDocument2 pagesAldosterone Renin RatioPoon CaniceNo ratings yet
- Brain Mapping KMB 1 + PenilaianDocument5 pagesBrain Mapping KMB 1 + PenilaianAnisNo ratings yet
- Male Reproductive System and Female Reproductive SystemDocument2 pagesMale Reproductive System and Female Reproductive SystemChristian Ezekiel LagmayNo ratings yet
- Biology PancreasDocument10 pagesBiology Pancreasjavier orellana mejiaNo ratings yet
- Prose: 5 The Summit Within: I Never Dreamed I Would Encounter A Snake in My BackyardDocument28 pagesProse: 5 The Summit Within: I Never Dreamed I Would Encounter A Snake in My BackyardSmiley CrochetNo ratings yet
- Glibenclamide For Diabetic Tipe IIDocument5 pagesGlibenclamide For Diabetic Tipe IIAnonymous A1qFGIXACNo ratings yet
- MCQs - CRF & BalanceDocument2 pagesMCQs - CRF & BalanceSara RezaNo ratings yet
- Research ThesisDocument18 pagesResearch ThesisJanAndrianCaingat100% (2)
- Integumentary SystemDocument34 pagesIntegumentary SystemJayrelle D. SafranNo ratings yet
- Vety Endocrine PharmaDocument59 pagesVety Endocrine PharmaSunilNo ratings yet
- Case Study PcosDocument6 pagesCase Study Pcosapi-315331895No ratings yet
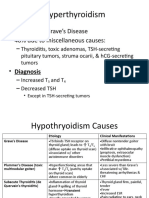
- Hyperthyroidism: - 60% Due To Grave's Disease - 40% Due To Miscellaneous CausesDocument6 pagesHyperthyroidism: - 60% Due To Grave's Disease - 40% Due To Miscellaneous CausesLeitavia D.No ratings yet
- Hormones and The Endocrine System: For Campbell Biology, Ninth EditionDocument106 pagesHormones and The Endocrine System: For Campbell Biology, Ninth EditionLaode Abdul KadirNo ratings yet
- Evaluation and Management of The Adrenal Incidentaloma - UpToDateDocument36 pagesEvaluation and Management of The Adrenal Incidentaloma - UpToDateIoanaNo ratings yet
- Thyroid CancerDocument82 pagesThyroid Cancerom100% (1)
- Material On PHYSIOLOGICAL CHANGES DURING PREGNANCYDocument21 pagesMaterial On PHYSIOLOGICAL CHANGES DURING PREGNANCYAnuradha MauryaNo ratings yet
- Lecture 17 - Thyroid Disorders (Including Struma and CA Thyroid) - Dr. M. Robikhul Ikhsan, SP - PD-KEMD (2021)Document21 pagesLecture 17 - Thyroid Disorders (Including Struma and CA Thyroid) - Dr. M. Robikhul Ikhsan, SP - PD-KEMD (2021)Ivan AditamaNo ratings yet
- Hormonal Imbalance and Its Causes in Young Females: January 2015Document6 pagesHormonal Imbalance and Its Causes in Young Females: January 2015figgernaggotNo ratings yet
- DiabetesDocument17 pagesDiabetesGeorge WondossenNo ratings yet
- Sebaceous CystDocument6 pagesSebaceous CystristaniaNo ratings yet
- HypothyroidismDocument90 pagesHypothyroidismwiwi_13No ratings yet
- Terdapat Hubungan Kadar Estradiol Dengan Ekspresi Kolagen Dan Elastin Pada Vagina Premenopause Dan PascamenopauseDocument9 pagesTerdapat Hubungan Kadar Estradiol Dengan Ekspresi Kolagen Dan Elastin Pada Vagina Premenopause Dan PascamenopausenawangprimailmiafeeNo ratings yet
- 1-Adrenocorticosteroids Chapter39Document94 pages1-Adrenocorticosteroids Chapter39hamidNo ratings yet
- Female and Male Reproductive OrgansDocument2 pagesFemale and Male Reproductive OrgansPink EaintNo ratings yet