You might also like
- Cash Flow Statement and Balance Sheet of A Solar Power Plant in APDocument35 pagesCash Flow Statement and Balance Sheet of A Solar Power Plant in APSriharsha Vavilala100% (1)
- Osha CFR 1910Document16 pagesOsha CFR 1910CI Amilcar100% (3)
- Large-Bowel Obstruction: Nihal Hamouda, MD Scott A. Jorgensen, MD Alexander J. Towbin, MD and Richard Towbin, MDDocument3 pagesLarge-Bowel Obstruction: Nihal Hamouda, MD Scott A. Jorgensen, MD Alexander J. Towbin, MD and Richard Towbin, MDDian FikriNo ratings yet
- Duplication Cyst of Pyloric Canal: A Rare Cause of Pediatric Gastric Outlet Obstruction: Rare Case ReportDocument4 pagesDuplication Cyst of Pyloric Canal: A Rare Cause of Pediatric Gastric Outlet Obstruction: Rare Case Reportfebyan yohanesNo ratings yet
- Apple Peel Small Bowel, A Review of Four Cases: Surgical and Radiographic AspectsDocument8 pagesApple Peel Small Bowel, A Review of Four Cases: Surgical and Radiographic AspectsraecmyNo ratings yet
- Combined Duodenal and Jejunal Atresia Forming A BiDocument3 pagesCombined Duodenal and Jejunal Atresia Forming A BiOvamelia JulioNo ratings yet
- Association of Duodenal Atresia, Malrotation, Ventricular Septal Defect, Endocardial Cushion Defect, Atrial Septal Defect, and Patent Ductus Arteriosus in A Down Syndrome PatientDocument3 pagesAssociation of Duodenal Atresia, Malrotation, Ventricular Septal Defect, Endocardial Cushion Defect, Atrial Septal Defect, and Patent Ductus Arteriosus in A Down Syndrome PatientasclepiuspdfsNo ratings yet
- Gastroschisis: Etiology, Diagnosis, Delivery Options, and CareDocument6 pagesGastroschisis: Etiology, Diagnosis, Delivery Options, and CareCarolina TorresNo ratings yet
- TrabajoDocument4 pagesTrabajopilarNo ratings yet
- RLQ PainDocument20 pagesRLQ PainBEATRICE SOPHIA PARMANo ratings yet
- Malrotation and atresia diagnosis with contrast studyDocument2 pagesMalrotation and atresia diagnosis with contrast studywp4saleNo ratings yet
- Template 1Document3 pagesTemplate 1Mohd KhalilNo ratings yet
- Pemeriksaan NeurologiDocument6 pagesPemeriksaan NeurologinnisamaliaNo ratings yet
- Colonic StenosisDocument3 pagesColonic StenosisBell SwanNo ratings yet
- World Surgery: DuodenumDocument2 pagesWorld Surgery: DuodenumBeladiena Citra SiregarNo ratings yet
- Plain Abdominal X-Rays Guide Diagnosis in ChildrenDocument7 pagesPlain Abdominal X-Rays Guide Diagnosis in ChildrenkishanNo ratings yet
- Minilaparoscopic Left Paraduodenal Hernia Repair-A CaseDocument4 pagesMinilaparoscopic Left Paraduodenal Hernia Repair-A CaseAritra PaulNo ratings yet
- 6255 24879 1 PBDocument2 pages6255 24879 1 PBSyafatesia nicky pratiwiNo ratings yet
- Insignis Surgery 2 Gallbladder and Extrahepatic Biliary SystemDocument7 pagesInsignis Surgery 2 Gallbladder and Extrahepatic Biliary SystemPARADISE JanoNo ratings yet
- A Left-Sided Periappendiceal Abscess in An Adult With Intestinal MalrotationDocument2 pagesA Left-Sided Periappendiceal Abscess in An Adult With Intestinal MalrotationRalynnRae MaeMyownnee HangadNo ratings yet
- Late Third Trimester Prenatal Ultrasound Diagnosis of Duodenal AtresiaDocument4 pagesLate Third Trimester Prenatal Ultrasound Diagnosis of Duodenal AtresiaIful SaifullahNo ratings yet
- UNCDCYSTDocument5 pagesUNCDCYSTeviltohuntNo ratings yet
- Acquired Colonic Atresia in A 4-Month Old Term Male Infant: A Rare Case ReportDocument3 pagesAcquired Colonic Atresia in A 4-Month Old Term Male Infant: A Rare Case ReportDenise CssNo ratings yet
- Medicine: A Newborn Patient With Both Annular Pancreas and Meckel 'S DiverticulumDocument5 pagesMedicine: A Newborn Patient With Both Annular Pancreas and Meckel 'S DiverticulumAdrian UmbriaNo ratings yet
- Diagnosing Ileal Atresia The Role of Clinical CorrDocument4 pagesDiagnosing Ileal Atresia The Role of Clinical CorrMohammad Hamim SultoniNo ratings yet
- Rare Combination of Chilaiditi and Fitz-Hugh Curtis Syndrome Causes Small-Bowel ObstructionDocument5 pagesRare Combination of Chilaiditi and Fitz-Hugh Curtis Syndrome Causes Small-Bowel ObstructionRengganis PutriNo ratings yet
- David J Ott - 1988 - Current Problems in Diagnostic RadiologyDocument28 pagesDavid J Ott - 1988 - Current Problems in Diagnostic RadiologysharfinaNo ratings yet
- Trilogy of Foregut Midgut and Hindgut Atresias PreDocument5 pagesTrilogy of Foregut Midgut and Hindgut Atresias PreEriekafebriayana RNo ratings yet
- Gastric Volvulus Through Morgagni Hernia and Intestinal Diverticulosis in An Adult Patient: A Case ReportDocument5 pagesGastric Volvulus Through Morgagni Hernia and Intestinal Diverticulosis in An Adult Patient: A Case ReportVirginia JawaNo ratings yet
- Annular PankreasDocument3 pagesAnnular PankreasAnonymous ocfZSRrrONo ratings yet
- Peritoneal Encapsulation: A Rare Cause of Small Bowel ObstructionDocument3 pagesPeritoneal Encapsulation: A Rare Cause of Small Bowel ObstructionNatalindah Jokiem Woecandra T. D.No ratings yet
- Appendix DuplicationDocument3 pagesAppendix DuplicationMario TrejoNo ratings yet
- Wandering Spleen, Gastric and Pancreatic Volvulus and Right-Sided Descending and Sigmoid ColonDocument8 pagesWandering Spleen, Gastric and Pancreatic Volvulus and Right-Sided Descending and Sigmoid ColonChristabella Natalia WijayaNo ratings yet
- MRI Findings in Fetuses with Abdominal Wall DefectsDocument7 pagesMRI Findings in Fetuses with Abdominal Wall DefectsIngrid TanasaNo ratings yet
- 1-5 BedahDocument9 pages1-5 BedahHalwia SiruaNo ratings yet
- Walker - Explorarea Radiologica A Tubului DigestivDocument11 pagesWalker - Explorarea Radiologica A Tubului DigestivDiana AndriucNo ratings yet
- Crigm2019 8907068Document4 pagesCrigm2019 8907068AlixNo ratings yet
- Wa0002Document14 pagesWa0002Katya RizqitaNo ratings yet
- Article Hernie InterneDocument4 pagesArticle Hernie Interneabdourahmane ndongNo ratings yet
- Ishii2020 Article CongenitalMultipleColonicAtresDocument5 pagesIshii2020 Article CongenitalMultipleColonicAtresAnisa GayatriNo ratings yet
- Delayed Diagnosis of Duodenal Atresia in An 11 Year Old: Case ReportDocument6 pagesDelayed Diagnosis of Duodenal Atresia in An 11 Year Old: Case ReportAnisa GayatriNo ratings yet
- Ladd's Band in The Adult, An Unusual Case of Occlusion Case Report Andreview of The LiteratureDocument5 pagesLadd's Band in The Adult, An Unusual Case of Occlusion Case Report Andreview of The Literaturewaldemar russellNo ratings yet
- Rectal Computer 2Document5 pagesRectal Computer 2Su-sake KonichiwaNo ratings yet
- Rare Obturator Hernia DiagnosisDocument4 pagesRare Obturator Hernia DiagnosisRifky TaniyoNo ratings yet
- Use Only: Investigating A Rare Cause of Intestinal OcclusionDocument2 pagesUse Only: Investigating A Rare Cause of Intestinal OcclusionDannyMichelleNo ratings yet
- JCDR 9 PD26Document2 pagesJCDR 9 PD26ceciliaNo ratings yet
- Intestinal Obstruction in Neonatal/Pediatric Surgery: by C.A. HajivassiliouDocument13 pagesIntestinal Obstruction in Neonatal/Pediatric Surgery: by C.A. HajivassiliouUlfa LathifaNo ratings yet
- 171-199 Embryologic and Anatomic Basis of Duodenal Surgery PDFDocument29 pages171-199 Embryologic and Anatomic Basis of Duodenal Surgery PDFРоман МошнягаNo ratings yet
- A Rare Variant Case of Pure Esophageal Atresia With An Atretic SegmentDocument3 pagesA Rare Variant Case of Pure Esophageal Atresia With An Atretic SegmentDetry Kala'lembangNo ratings yet
- Duplication Cyst of The CecumDocument3 pagesDuplication Cyst of The CecumMostafa ZainNo ratings yet
- International Journal of Surgery Case ReportsDocument5 pagesInternational Journal of Surgery Case ReportsJuan Eduardo Rios RodriguezNo ratings yet
- Ajcr 2010 1 6Document3 pagesAjcr 2010 1 6Muhammad Bilal MirzaNo ratings yet
- Apple Peel Atresia: A Case ReportDocument3 pagesApple Peel Atresia: A Case ReportNasriNo ratings yet
- Case Series of Unusual Causes Intestinal Obstruction in Infants and ChildrenDocument9 pagesCase Series of Unusual Causes Intestinal Obstruction in Infants and ChildrenSnega KaranNo ratings yet
- Cholecystogastric Fistula Penetrating Duodenum and Caused A Duodenal Obstruction A Case ReportDocument6 pagesCholecystogastric Fistula Penetrating Duodenum and Caused A Duodenal Obstruction A Case ReportHerald Scholarly Open AccessNo ratings yet
- Noncommunicating Isolated Enteric Duplication Cyst in The Abdomen in Children: Report of One Case and Review of The LiteratureDocument3 pagesNoncommunicating Isolated Enteric Duplication Cyst in The Abdomen in Children: Report of One Case and Review of The Literatureallan felipeNo ratings yet
- Atresia Coli in A Japanese Black Calf Diagnosed by A Barium Sulphate Enema Contrast Radiograph in The Standing Position: A Case ReportDocument4 pagesAtresia Coli in A Japanese Black Calf Diagnosed by A Barium Sulphate Enema Contrast Radiograph in The Standing Position: A Case ReportBeratha MuktiNo ratings yet
- Imaging Patients With Acute Abdominal PainDocument16 pagesImaging Patients With Acute Abdominal PainNaelul IzahNo ratings yet
- Total Colonic Aganglionosis (Zuelzer Wilson Syndrome) An EnigmaDocument2 pagesTotal Colonic Aganglionosis (Zuelzer Wilson Syndrome) An EnigmarmysdsNo ratings yet
- Journal of Pediatric Surgery CASE REPORTS: Sonal Nagra, Jitoko K. CamaDocument3 pagesJournal of Pediatric Surgery CASE REPORTS: Sonal Nagra, Jitoko K. CamazuliaahmadNo ratings yet
- Journal of Pediatric Surgery CASE REPORTS: Sonal Nagra, Jitoko K. CamaDocument3 pagesJournal of Pediatric Surgery CASE REPORTS: Sonal Nagra, Jitoko K. CamazuliaahmadNo ratings yet
- Dokumen Tanpa Judul PDFDocument6 pagesDokumen Tanpa Judul PDFhaidar HumairNo ratings yet
- Dokumen Tanpa JudulDocument9 pagesDokumen Tanpa JudulHaidar HumairNo ratings yet
- Dokumen Tanpa Judul PDFDocument1 pageDokumen Tanpa Judul PDFhaidar HumairNo ratings yet
- Salinan Terjemahan Dokumen Tanpa JudulDocument1 pageSalinan Terjemahan Dokumen Tanpa JudulHaidar HumairNo ratings yet
- Dokumen Tanpa JudulDocument1 pageDokumen Tanpa Judulhaidar HumairNo ratings yet
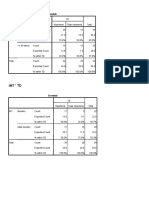
- Crosstab Analysis of Hypertension and IMT RiskDocument1 pageCrosstab Analysis of Hypertension and IMT Riskhaidar HumairNo ratings yet
- Salinan Terjemahan Dokumen Tanpa JudulDocument1 pageSalinan Terjemahan Dokumen Tanpa JudulHaidar HumairNo ratings yet
- Salinan Terjemahan Dokumen Tanpa JudulDocument1 pageSalinan Terjemahan Dokumen Tanpa JudulHaidar HumairNo ratings yet
- Local wisdom and traditional fishing of the Bajo communityDocument1 pageLocal wisdom and traditional fishing of the Bajo communityhaidar HumairNo ratings yet
- Sumber RefaratDocument55 pagesSumber Refarathaidar HumairNo ratings yet
- Salinan Terjemahan Dokumen Tanpa Judul PDFDocument1 pageSalinan Terjemahan Dokumen Tanpa Judul PDFhaidar HumairNo ratings yet
- Dapus Refarat RDN HaidarDocument2 pagesDapus Refarat RDN Haidarhaidar HumairNo ratings yet
- Sumber RefaratDocument55 pagesSumber Refarathaidar HumairNo ratings yet
- FINAL Exam - Answer SheetDocument1 pageFINAL Exam - Answer SheetViggo VillanuevaNo ratings yet
- Indian Standard: Specification For Reels and Drums For Bare ConductorsDocument13 pagesIndian Standard: Specification For Reels and Drums For Bare ConductorsUppala Krishna ChaitanyaNo ratings yet
- (GUIDE) Advanced Interactive Governor Tweaks Buttery Smooth and Insane Battery Life! - Page 519 - Xda-DevelopersDocument3 pages(GUIDE) Advanced Interactive Governor Tweaks Buttery Smooth and Insane Battery Life! - Page 519 - Xda-Developersdadme010% (2)
- A Teacher Education ModelDocument128 pagesA Teacher Education ModelMelinda LabianoNo ratings yet
- Decolonising The FutureDocument20 pagesDecolonising The Futurebybee7207No ratings yet
- MB1 - The Australian Economy PA 7092016Document8 pagesMB1 - The Australian Economy PA 7092016ninja980117No ratings yet
- Odoo JS Framework Rewrite Brings New Views and TestingDocument68 pagesOdoo JS Framework Rewrite Brings New Views and TestingglobalknowledgeNo ratings yet
- Communicate With S7-1200 Via EhernetDocument6 pagesCommunicate With S7-1200 Via EhernetRegisNo ratings yet
- OCS Study Analyzes Instrument Performance for NC Oceanography ProgramDocument127 pagesOCS Study Analyzes Instrument Performance for NC Oceanography ProgramAniruddhNo ratings yet
- Plan & Elevation of Dog-Legged StaircaseDocument1 pagePlan & Elevation of Dog-Legged Staircasesagnik bhattacharjeeNo ratings yet
- 1081 Camid Vs Op DigestDocument2 pages1081 Camid Vs Op DigestLennart Reyes67% (3)
- Tax2win's Growth Strategy Through Comprehensive Tax SolutionsDocument6 pagesTax2win's Growth Strategy Through Comprehensive Tax SolutionsAhmar AyubNo ratings yet
- Bus Crash LawsuitDocument7 pagesBus Crash LawsuitNewsTeam20No ratings yet
- Haukongo Nursing 2020Document86 pagesHaukongo Nursing 2020Vicky Torina ShilohNo ratings yet
- Altracs: A Superior Thread-Former For Light AlloysDocument8 pagesAltracs: A Superior Thread-Former For Light AlloysSquidwardNo ratings yet
- GUEST REGISTRATION CARDDocument1 pageGUEST REGISTRATION CARDRasmi Ranjan Kar100% (1)
- The Role of Business in Social and Economic Development Chapter 1Document18 pagesThe Role of Business in Social and Economic Development Chapter 1Emil EscasinasNo ratings yet
- The Future of Retail in Asia-Pacific: How To Thrive at High SpeedDocument12 pagesThe Future of Retail in Asia-Pacific: How To Thrive at High SpeedPhạm Thanh HuyềnNo ratings yet
- Kneehab XP Instructions and UsageDocument16 pagesKneehab XP Instructions and UsageMVP Marketing and DesignNo ratings yet
- Dialogic DSI Signaling Servers: SIU Mode User ManualDocument304 pagesDialogic DSI Signaling Servers: SIU Mode User ManualAdiansyah Rama67% (3)
- Robotic Surgery History and SystemsDocument28 pagesRobotic Surgery History and SystemsLidhi DileepNo ratings yet
- Diesel Injector FailureDocument19 pagesDiesel Injector FailureWayne Mcmeekan100% (2)
- Penetron Admix FlyerDocument2 pagesPenetron Admix Flyernght7942No ratings yet
- MCP Lab Manual C-16Document62 pagesMCP Lab Manual C-16siri.pogula67% (6)
- Social and cultural geographies of Southeast Asia exploredDocument18 pagesSocial and cultural geographies of Southeast Asia exploredJohn Lemuel MagnayeNo ratings yet
- L4 Examples - Exact Differential Equations PDFDocument16 pagesL4 Examples - Exact Differential Equations PDFCarlo EdolmoNo ratings yet
- Bangladesh Premier League 2024 Schedule, Live Scores and ResultsDocument5 pagesBangladesh Premier League 2024 Schedule, Live Scores and Resultsmoslahuddin2022No ratings yet
- MObile InvoiceDocument1 pageMObile Invoicechandra kiran KodavatiNo ratings yet