You might also like
- Tlac 3.0 PDFDocument26 pagesTlac 3.0 PDFFook Ngo83% (6)
- Xerox Case StudyDocument10 pagesXerox Case StudyMojiNo ratings yet
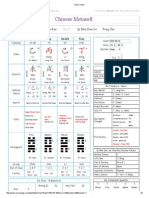
- Ba Zi Chart1Document2 pagesBa Zi Chart1adisebe100% (1)
- IB Biology Lab Report GuideDocument16 pagesIB Biology Lab Report Guideaufafua100% (1)
- Year 5 Maths Revision BookletDocument31 pagesYear 5 Maths Revision BookletCamille100% (2)
- Ecdis PresentationDocument62 pagesEcdis PresentationDiana Morales100% (10)
- Cognitive Deficits Induced in Young Rats by Long-Term Corticosterone AdministrationDocument7 pagesCognitive Deficits Induced in Young Rats by Long-Term Corticosterone AdministrationJean Pierre Chastre LuzaNo ratings yet
- J of Comparative Neurology - 25 November 1996 - AlonsoDocument25 pagesJ of Comparative Neurology - 25 November 1996 - AlonsoEccoNo ratings yet
- Physio in AnimalsDocument6 pagesPhysio in AnimalsCornerstone OrganizationNo ratings yet
- A Classical Case of Duchenne Muscular Dystrophy 2161 1041 4 1000139Document2 pagesA Classical Case of Duchenne Muscular Dystrophy 2161 1041 4 1000139Yasif AbbasNo ratings yet
- 2897 FullDocument6 pages2897 FullJean Pierre Chastre LuzaNo ratings yet
- Neuro 2Document5 pagesNeuro 2Ivan RisnaNo ratings yet
- Reimers 2007Document8 pagesReimers 2007Joanna Riera MNo ratings yet
- Nervous Disease Associated With Coccdiosis in Young CattleDocument2 pagesNervous Disease Associated With Coccdiosis in Young CattleRaul alejandro Kim gomezNo ratings yet
- Fractured in AnimalDocument6 pagesFractured in AnimalIvan RisnaNo ratings yet
- Management of Oesophageal Obstruction in A DogDocument2 pagesManagement of Oesophageal Obstruction in A DogHari Krishna Nunna V VNo ratings yet
- Broom 1993Document4 pagesBroom 1993maria vitoria saldanhaNo ratings yet
- A Case of Choke in A She BuffaloDocument2 pagesA Case of Choke in A She BuffaloHari Krishna Nunna V VNo ratings yet
- Surgical Correction of Idiopathic Megacolon in Cats: Feline Practice January 1992Document7 pagesSurgical Correction of Idiopathic Megacolon in Cats: Feline Practice January 1992Ayu DinaNo ratings yet
- Acute and Chronic Responses To The Convulsant Pilocarpine in DBA2J and AJ Mice (2007)Document11 pagesAcute and Chronic Responses To The Convulsant Pilocarpine in DBA2J and AJ Mice (2007)Apróné Török IbolyaNo ratings yet
- Neuro 1Document5 pagesNeuro 1Ivan RisnaNo ratings yet
- Marchioro Et Al. - 2005 - Postnatal Neurogenesis in The Medial Cortex of The Tropical Lizard Tropidurus HispidusDocument7 pagesMarchioro Et Al. - 2005 - Postnatal Neurogenesis in The Medial Cortex of The Tropical Lizard Tropidurus HispidusOsny SillasNo ratings yet
- Treatment of The Lateral Patellar Luxation in Toy PoodlesDocument5 pagesTreatment of The Lateral Patellar Luxation in Toy PoodlesNucleoNo ratings yet
- Pandi Culat I OnDocument7 pagesPandi Culat I OnOscar RamirezNo ratings yet
- Bilateral TemporoDocument4 pagesBilateral TemporoHusna UnanaNo ratings yet
- Clinicopathologic Features of Brain Herniation in AnimalsDocument7 pagesClinicopathologic Features of Brain Herniation in AnimalsDesNo ratings yet
- Tutorial 3. Oct 23 - Barbeau&Rossignol1987-1Document12 pagesTutorial 3. Oct 23 - Barbeau&Rossignol1987-1jaxter2002No ratings yet
- Oligospermia,: Which, NormalDocument4 pagesOligospermia,: Which, NormalJohn DoeNo ratings yet
- Familial Chondrodysplasia in Holstein CalvesDocument6 pagesFamilial Chondrodysplasia in Holstein Calvesana lauraNo ratings yet
- Bio350 6thabd ProtocolDocument19 pagesBio350 6thabd ProtocolRobin Lewis CooperNo ratings yet
- Prenatal Growth Retardation, Pelvic Hypoplasia, and Arthrogrypotic Changes of Lower LimbsDocument8 pagesPrenatal Growth Retardation, Pelvic Hypoplasia, and Arthrogrypotic Changes of Lower LimbsPaul AsturbiarisNo ratings yet
- Masticator Muscle Myositis in A Dog - A Case: P.V. Tresamol, K. Vinodkumar, S. Anoop, K.M. Lucy and S. AjithkumarDocument3 pagesMasticator Muscle Myositis in A Dog - A Case: P.V. Tresamol, K. Vinodkumar, S. Anoop, K.M. Lucy and S. Ajithkumarcicelynara94No ratings yet
- Correlates of in Rats: Physiological Prolonged Sleep DeprivationDocument3 pagesCorrelates of in Rats: Physiological Prolonged Sleep DeprivationJuan Vale TrujilloNo ratings yet
- Slavo Tine K 1996Document6 pagesSlavo Tine K 1996jahfdfgsdjad asdhsajhajdkNo ratings yet
- Case Report Wobbler Syndrome (CVSM)Document9 pagesCase Report Wobbler Syndrome (CVSM)YraNo ratings yet
- Historical Note: Marie Jean Pierre Flourens (1794-1867) : An Extraordinary Scientist of His TimeDocument1 pageHistorical Note: Marie Jean Pierre Flourens (1794-1867) : An Extraordinary Scientist of His TimeElelmoduNo ratings yet
- DiafragmaDocument8 pagesDiafragmaRodrigo Diaz VqzNo ratings yet
- Ditunno 2014 PDFDocument13 pagesDitunno 2014 PDFkeith andriesNo ratings yet
- 5498 FullDocument10 pages5498 FullOlga Peña HernandezNo ratings yet
- Avascular Necrosis of The Femoral Head in Dogs - RDocument5 pagesAvascular Necrosis of The Femoral Head in Dogs - RninagonzalezmedelNo ratings yet
- Necrotizing Cerebellitis Neospora JVIM 2010Document8 pagesNecrotizing Cerebellitis Neospora JVIM 2010Rafael Porto GoncalvesNo ratings yet
- Displasia de Cadera CaninaDocument9 pagesDisplasia de Cadera CaninaPam LinkoNo ratings yet
- Heng 2017Document6 pagesHeng 2017CLINICA VETERINARIA DE MEDELLINNo ratings yet
- Evidence For Autosomal Cerebral Gigantism: Recessive InheritanceDocument8 pagesEvidence For Autosomal Cerebral Gigantism: Recessive InheritanceBlhackNo ratings yet
- External HydrocephalusDocument6 pagesExternal HydrocephalusJorge VergaraNo ratings yet
- Hypertrophic Osteodystrophy Great Dane: PuppyDocument4 pagesHypertrophic Osteodystrophy Great Dane: PuppyGavrilo Janja VlajinacNo ratings yet
- tmp8804 TMPDocument21 pagestmp8804 TMPFrontiersNo ratings yet
- Third Ventricular Cavernous Haemangioma - Darwish2005Document3 pagesThird Ventricular Cavernous Haemangioma - Darwish2005Bruno Diaz LlanesNo ratings yet
- Animals 13 01233Document11 pagesAnimals 13 01233dpcamposhNo ratings yet
- Equine Neural Angiostrongylosis: Aust Vet J 68Document3 pagesEquine Neural Angiostrongylosis: Aust Vet J 68Angeles GonzalezNo ratings yet
- Hypervitaminosis A in The Cat A Case Report and Review of The LiteratureDocument6 pagesHypervitaminosis A in The Cat A Case Report and Review of The LiteratureCarlos Alberto AmorimNo ratings yet
- Colloids As Big AtomsDocument3 pagesColloids As Big AtomsShashankKamdarNo ratings yet
- Neurosurgery in Feline Epilepsy Including Clinicopatholo - 2022 - The VeterinarDocument10 pagesNeurosurgery in Feline Epilepsy Including Clinicopatholo - 2022 - The VeterinarGNo ratings yet
- Ader, Cohen, 1982 - Behaviorally Conditioned Immunosuppresion and Murine Systemic Lupus ErythematosuDocument3 pagesAder, Cohen, 1982 - Behaviorally Conditioned Immunosuppresion and Murine Systemic Lupus ErythematosuDiogo Deganeli de Brito VaragoNo ratings yet
- Dis. Model. Mech. 2010 Hortopan 144 8Document5 pagesDis. Model. Mech. 2010 Hortopan 144 8Awanish MishraNo ratings yet
- Effect Ofl Dopa On Oculogyric Crises inDocument2 pagesEffect Ofl Dopa On Oculogyric Crises inJoséNo ratings yet
- gutierrez-quintana2014.MALFORMACIONES VERTEBRALES TORÁCICAS CONGÉNITAS EN RAZAS DE PERROS BRQUICÉFÁLICOS DE "COLA DE TORNILLO"Document7 pagesgutierrez-quintana2014.MALFORMACIONES VERTEBRALES TORÁCICAS CONGÉNITAS EN RAZAS DE PERROS BRQUICÉFÁLICOS DE "COLA DE TORNILLO"Joa FloresNo ratings yet
- Cmo EbookDocument5 pagesCmo EbookDiana Rahmayani PutriNo ratings yet
- Cap. 11 - HamstersDocument10 pagesCap. 11 - HamstersNailson JúniorNo ratings yet
- Behavioral and Metabolic Features of Repetitive Seizures in Immature and Mature RatsDocument13 pagesBehavioral and Metabolic Features of Repetitive Seizures in Immature and Mature RatsFrontiersNo ratings yet
- Peacock 1990Document7 pagesPeacock 1990Alvaro Perez HenriquezNo ratings yet
- TMP 6 DAEDocument16 pagesTMP 6 DAEFrontiersNo ratings yet
- Perceptual and Motor SkillsDocument11 pagesPerceptual and Motor SkillsSwathi GeethaNo ratings yet
- Alaskan 20 Husky 20 Encephalopathy 202Document13 pagesAlaskan 20 Husky 20 Encephalopathy 202Mao Tse Tung ToledoNo ratings yet
- Top 5 Consequences of BrachycephalyDocument4 pagesTop 5 Consequences of BrachycephalyCabinet VeterinarNo ratings yet
- Neurobiology and BehaviorFrom EverandNeurobiology and BehaviorA. O. Dennis WillowsRating: 5 out of 5 stars5/5 (1)
- Cornish Rex (CRX) (Standard Source: Fife 1987) : GeneralDocument2 pagesCornish Rex (CRX) (Standard Source: Fife 1987) : Generalandrostona980No ratings yet
- Cornish Rex: General StandardDocument1 pageCornish Rex: General Standardandrostona980No ratings yet
- Cornish Rex (CR) : Cornish Rex Breed Standard, 05/01/2008 Cornish Rex Breed Standard, 05/01/2008Document1 pageCornish Rex (CR) : Cornish Rex Breed Standard, 05/01/2008 Cornish Rex Breed Standard, 05/01/2008androstona980No ratings yet
- The Cornish RexDocument3 pagesThe Cornish Rexandrostona980No ratings yet
- Peterbald (PD) : Transitional State While Being ShownDocument1 pagePeterbald (PD) : Transitional State While Being Shownandrostona980No ratings yet
- Peterbald: General StandardDocument2 pagesPeterbald: General Standardandrostona980No ratings yet
- PeterbaldDocument2 pagesPeterbaldandrostona980No ratings yet
- Peterbald (PD) : R e Vise D 0 5/0 1/0 8 R e Vise D 0 5/0 1/0 8Document1 pagePeterbald (PD) : R e Vise D 0 5/0 1/0 8 R e Vise D 0 5/0 1/0 8androstona980No ratings yet
- The Scottish FoldDocument3 pagesThe Scottish Foldandrostona980No ratings yet
- The Peterbald Article PDFDocument16 pagesThe Peterbald Article PDFandrostona980No ratings yet
- Case ReportDocument5 pagesCase Reportandrostona980No ratings yet
- Devon Rex: General StandardDocument1 pageDevon Rex: General Standardandrostona980No ratings yet
- UP Devon Rex Vet DermDocument7 pagesUP Devon Rex Vet Dermandrostona980No ratings yet
- Growth Opportunities For Brands During The Coronavirus CrisisDocument12 pagesGrowth Opportunities For Brands During The Coronavirus CrisisAleeza AnjumNo ratings yet
- Fraud Risk Management ProgramDocument68 pagesFraud Risk Management Programaa yudhoNo ratings yet
- Teacher-Made SCIENCE 4 Q1-Week 4 Activity Sheets With Answer KeyDocument15 pagesTeacher-Made SCIENCE 4 Q1-Week 4 Activity Sheets With Answer KeyCeleste Dailisan VillaranNo ratings yet
- ADMU V CapulongDocument21 pagesADMU V CapulongjunjunNo ratings yet
- Adverbs of Degree Java LauditDocument15 pagesAdverbs of Degree Java LauditPepitoNo ratings yet
- How To Pass The FSODocument5 pagesHow To Pass The FSODeutsch FrancaisNo ratings yet
- Greek Melkite Catholic Patriarchate of AntiochDocument21 pagesGreek Melkite Catholic Patriarchate of AntiochSamee HasanNo ratings yet
- SST TEMPLATES (Summarize Spoken Teswt)Document3 pagesSST TEMPLATES (Summarize Spoken Teswt)Nabin AdhikariNo ratings yet
- PCCA RobbioDocument4 pagesPCCA RobbioIsobel WhiteleggNo ratings yet
- Linear AlgebraDocument499 pagesLinear AlgebraAnsh Mittal100% (4)
- Slide Human Digestive - SCF2NUTRITIONDocument23 pagesSlide Human Digestive - SCF2NUTRITIONellayuslianaNo ratings yet
- JKF8 Intelligent Reactive Power Compensation ControllerDocument4 pagesJKF8 Intelligent Reactive Power Compensation ControllerGuillermo Morales HerreraNo ratings yet
- Models and Technique of MP Demand and Supply Forecasting... by Shahid ElimsDocument19 pagesModels and Technique of MP Demand and Supply Forecasting... by Shahid Elimsshahid veettil91% (11)
- 2019 SC CL January June HO CLCDocument31 pages2019 SC CL January June HO CLCIvan LeeNo ratings yet
- Guided Meditation - Tara Brach - AttachmentDocument1 pageGuided Meditation - Tara Brach - AttachmentSantiago Carey100% (1)
- Man Singh's Manakutuhala and The DhrupadDocument10 pagesMan Singh's Manakutuhala and The DhrupadAman ShrivastavaNo ratings yet
- Answer of Every Question !! - Uttaranchal Objective General Knowledge Solved Questions PDFDocument4 pagesAnswer of Every Question !! - Uttaranchal Objective General Knowledge Solved Questions PDFMrigendra MishraNo ratings yet
- Share Capital and Creditor Protection Efficient Rules For A Modern Company LawDocument54 pagesShare Capital and Creditor Protection Efficient Rules For A Modern Company LawMichelle T.No ratings yet
- Q3 Arts 7Document37 pagesQ3 Arts 7john robie del rosarioNo ratings yet
- Indigenous MethodlogiesDocument16 pagesIndigenous MethodlogiesMaria Paula MenesesNo ratings yet
- Drug Prescription - DR Mahmoud DorghamDocument72 pagesDrug Prescription - DR Mahmoud DorghamhaiaoNo ratings yet
- Erp Testing PDFDocument2 pagesErp Testing PDFChelseaNo ratings yet
- Verschueren Jef.-Understanding PragmaticsDocument309 pagesVerschueren Jef.-Understanding PragmaticsMahfoodh AljubouryNo ratings yet
- Time RetractionDocument4 pagesTime RetractionVIVA, Trisha Anne L.No ratings yet