You might also like
- Understanding Your NeurotypeDocument18 pagesUnderstanding Your NeurotypeFabiano Lacerda100% (6)
- Psychosexual TheoryDocument27 pagesPsychosexual Theoryrejeneil100% (1)
- FILA Wrestling Science Review 2010Document53 pagesFILA Wrestling Science Review 2010mkrohlas100% (1)
- Hydro Electric Power Plant 28012019Document85 pagesHydro Electric Power Plant 28012019Rahul YadavNo ratings yet
- Effects of Different Volume-Equated Resistance Training Loading Strategies On Muscular Adaptations in Well-Trained MenDocument11 pagesEffects of Different Volume-Equated Resistance Training Loading Strategies On Muscular Adaptations in Well-Trained Menjoaoevandro100% (1)
- The Effects of Myofascial Release With Foam Rolling On Performance PDFDocument8 pagesThe Effects of Myofascial Release With Foam Rolling On Performance PDFhenriqueNo ratings yet
- HypertrophyDocument107 pagesHypertrophymehrdad_44100% (1)
- Schoenfeld 2015Document9 pagesSchoenfeld 2015GutoGonçalves100% (1)
- Progress Report - MC&T - WK - 34Document3 pagesProgress Report - MC&T - WK - 34sellitt ngNo ratings yet
- 2016 Effects of Low Versus High-Load Resistance Training On Muscle Strength and Hypertrophy in Well-Trained MenDocument32 pages2016 Effects of Low Versus High-Load Resistance Training On Muscle Strength and Hypertrophy in Well-Trained MenFrancisco Antonó Castro WeithNo ratings yet
- The Impact of Metabolic Stress On Hormonal Responses and Muscular AdaptationsDocument10 pagesThe Impact of Metabolic Stress On Hormonal Responses and Muscular AdaptationsJoão NunesNo ratings yet
- Blood Flow Restriction Resistance Training Potential Benefits of Choking The MusclesDocument2 pagesBlood Flow Restriction Resistance Training Potential Benefits of Choking The MusclesPaisan NgerndeeNo ratings yet
- 0906 0909 Lab Accreditation I II (Class Notes) (Vanessa 2022)Document82 pages0906 0909 Lab Accreditation I II (Class Notes) (Vanessa 2022)Vienne Yuen Wing YanNo ratings yet
- Increasing Lean Mass and Strength - HFT vs. LFTDocument9 pagesIncreasing Lean Mass and Strength - HFT vs. LFTKarn Mamgain100% (1)
- (Journal of Strength & Conditioning Research) Schoenfeld BJ, Peterson MD, Ogborn D, Contreras B, Sonmez GT-[Article] Effects of Low- Versus High-Load Resistance Training on Muscle Strength and HypertrDocument32 pages(Journal of Strength & Conditioning Research) Schoenfeld BJ, Peterson MD, Ogborn D, Contreras B, Sonmez GT-[Article] Effects of Low- Versus High-Load Resistance Training on Muscle Strength and Hypertrhp_blacklight7402No ratings yet
- The Effect of Training Volume and Intensity On Improvements in Muscular Strength and Size in Resistance-Trained MenDocument17 pagesThe Effect of Training Volume and Intensity On Improvements in Muscular Strength and Size in Resistance-Trained MenDenis OsmenajNo ratings yet
- The Effect of Training Volume and Intensity On ImDocument4 pagesThe Effect of Training Volume and Intensity On ImCAMPERNo ratings yet
- Muscleactivationduringlow Versushigh Loadresistancetraininginwell TrainedmenDocument7 pagesMuscleactivationduringlow Versushigh Loadresistancetraininginwell TrainedmenAgustín Adamo zarateNo ratings yet
- American College Sports Medicine Strength Training and Responses in BeginnersDocument9 pagesAmerican College Sports Medicine Strength Training and Responses in BeginnersMohd Syafiq HasriNo ratings yet
- Effects of 8 Weeks Equal-Volume Resistance TrainingDocument7 pagesEffects of 8 Weeks Equal-Volume Resistance TrainingChimpompumNo ratings yet
- Moderately Heavy Exercise Produces Lower Cardiovascular, RPE, and Discomfort Compared To Lower Load Exercise With and Without Blood Flow RestrictionDocument8 pagesModerately Heavy Exercise Produces Lower Cardiovascular, RPE, and Discomfort Compared To Lower Load Exercise With and Without Blood Flow RestrictionJuanfran Montesinos GarciaNo ratings yet
- Peripheral Electrical and Magnetic Stimulation To Augment Resistance TrainingDocument15 pagesPeripheral Electrical and Magnetic Stimulation To Augment Resistance TrainingFilipe FariaNo ratings yet
- Acute Skeletal Muscle Responses To Very Low-Load Resistance Exercise With and Without The Application of Blood Flow Restriction in The Upper BodyDocument8 pagesAcute Skeletal Muscle Responses To Very Low-Load Resistance Exercise With and Without The Application of Blood Flow Restriction in The Upper BodyFabiano LacerdaNo ratings yet
- Balance Improvements in Older Women Effects ofDocument12 pagesBalance Improvements in Older Women Effects ofRENATO_VEZETIVNo ratings yet
- 2JSCR 23 3 962 71 09Document10 pages2JSCR 23 3 962 71 09RosaneLacerdaNo ratings yet
- Effect of Isometric Quadriceps Exercise On Muscle StrengthDocument7 pagesEffect of Isometric Quadriceps Exercise On Muscle StrengthAyu RoseNo ratings yet
- 28 - Jpts 2016 190Document6 pages28 - Jpts 2016 190alsyafarinoorNo ratings yet
- Effects of Low-Intensity Resistance Exercise With Vascular Occlusion On Physical Function in Healthy Elderly People.-2Document7 pagesEffects of Low-Intensity Resistance Exercise With Vascular Occlusion On Physical Function in Healthy Elderly People.-2Ingrid Ramirez PNo ratings yet
- The Acute Muscular Response To Blood Flow-Restricted Exercise With Very Low Relative PressureDocument9 pagesThe Acute Muscular Response To Blood Flow-Restricted Exercise With Very Low Relative PressureFabiano LacerdaNo ratings yet
- Accepted: Eccentric Overload Training: A Viable Strategy To Enhance Muscle Hypertrophy?Document10 pagesAccepted: Eccentric Overload Training: A Viable Strategy To Enhance Muscle Hypertrophy?Alexandre FerreiraNo ratings yet
- Effect of Muscle Oxygenation During Resistance Exercise On Anabolic Hormone ResponseDocument6 pagesEffect of Muscle Oxygenation During Resistance Exercise On Anabolic Hormone ResponseAle CostaNo ratings yet
- Carga HipertrofiaDocument34 pagesCarga HipertrofiaCristina VicenteNo ratings yet
- 10.1007@s40279 020 01331 7Document17 pages10.1007@s40279 020 01331 7Jonathan BaldeonNo ratings yet
- Is Resistance Training To Muscular Failure Necessary?: Sanmy R. Nóbrega and Cleiton A. LibardiDocument4 pagesIs Resistance Training To Muscular Failure Necessary?: Sanmy R. Nóbrega and Cleiton A. LibardijoaoevandroNo ratings yet
- ElsangedyDocument6 pagesElsangedyPaulo Emilio Marchete RohorNo ratings yet
- Effects of Horizontal and Incline Bench Press On Neuromuscular Adaptations in Untrained Young MenDocument14 pagesEffects of Horizontal and Incline Bench Press On Neuromuscular Adaptations in Untrained Young MenAndré Evandro MartinsNo ratings yet
- The Influence of Exercise Load With and Without Different Levels of Blood Flow Restriction On Acute Changes in Muscle Thickness and LactateDocument7 pagesThe Influence of Exercise Load With and Without Different Levels of Blood Flow Restriction On Acute Changes in Muscle Thickness and LactateFabiano LacerdaNo ratings yet
- Calatayud Et Al.,2014 (Bench Press and Push-Ups at Comparable EMG Levels Strength Gains)Document8 pagesCalatayud Et Al.,2014 (Bench Press and Push-Ups at Comparable EMG Levels Strength Gains)AnaNo ratings yet
- Evidence BasedGuidelinesforResistanceTrainingVolumetoMaximizeMuscleHypertrophy PDFDocument14 pagesEvidence BasedGuidelinesforResistanceTrainingVolumetoMaximizeMuscleHypertrophy PDFjuan091184No ratings yet
- Adaptations Slow-Velocity VS Traditional Resistance Training - Schuenke Et Al. 2012 PDFDocument11 pagesAdaptations Slow-Velocity VS Traditional Resistance Training - Schuenke Et Al. 2012 PDFPablo FitNo ratings yet
- Accepted Manuscript: Medical HypothesesDocument23 pagesAccepted Manuscript: Medical HypothesesFabiano LacerdaNo ratings yet
- Series para MMII e MMSS PDFDocument6 pagesSeries para MMII e MMSS PDFJúnior Alvacir CamargoNo ratings yet
- 14 CPFI Tri-SetDocument6 pages14 CPFI Tri-SetjoaoevandroNo ratings yet
- 2018 Article 1051Document10 pages2018 Article 1051Vukašin Schooly StojanovićNo ratings yet
- Acute Effect of Two Aerobic Exercise ModesDocument5 pagesAcute Effect of Two Aerobic Exercise Modeswander_dukaNo ratings yet
- Progressive Resistive Exercise: Erbil Polytechnic UniversityDocument10 pagesProgressive Resistive Exercise: Erbil Polytechnic UniversityNur DilshadNo ratings yet
- Lasevicius2018 PDFDocument10 pagesLasevicius2018 PDFAgustinaNo ratings yet
- Effects of Resistance Exercise and Creatine Supplementation On Myasthenia Gravis - A Case StudyDocument4 pagesEffects of Resistance Exercise and Creatine Supplementation On Myasthenia Gravis - A Case StudyMiguel KennedyNo ratings yet
- Estudio Sobre La Restricción Del Flujo Sanguíneo en El EntrenamientoDocument11 pagesEstudio Sobre La Restricción Del Flujo Sanguíneo en El EntrenamientoEnrique Manuel CerettiNo ratings yet
- Comparison of The Effects of A Single Bout of Resistance Exercises With Different Intensities On Oxidative Stress in Untrained Male StudentsDocument5 pagesComparison of The Effects of A Single Bout of Resistance Exercises With Different Intensities On Oxidative Stress in Untrained Male StudentsRoy WilsonNo ratings yet
- Buttner - JAP 07 - MicroarrayDocument12 pagesButtner - JAP 07 - Microarrayf1r3br4nd9427No ratings yet
- Artigo 10Document9 pagesArtigo 10Átrio Reabilitação CardiopulmonarNo ratings yet
- Short-Term High-Vs. Low-Velocity Isokinetic Lengthening Training Results in Greater Hypertrophy of The Elbow Exors in Young MenDocument11 pagesShort-Term High-Vs. Low-Velocity Isokinetic Lengthening Training Results in Greater Hypertrophy of The Elbow Exors in Young MenAlejandro Albert RequesNo ratings yet
- Running Head: Neither Load Nor Hormones Determine HypertrophyDocument32 pagesRunning Head: Neither Load Nor Hormones Determine HypertrophyMarcelo NorisNo ratings yet
- Repeated Plyometric Exercise Attenuates Blood Glucose in Healthy AdultsDocument9 pagesRepeated Plyometric Exercise Attenuates Blood Glucose in Healthy AdultsBlake d souzaNo ratings yet
- Jenkins Et Al (2015) EJAP - Muscle Activation During Three Sets To Failure at 80 vs. 30% 1RM Resistance ExerciseDocument16 pagesJenkins Et Al (2015) EJAP - Muscle Activation During Three Sets To Failure at 80 vs. 30% 1RM Resistance ExerciseFabiano LacerdaNo ratings yet
- Absctrac Congreso NSCADocument144 pagesAbsctrac Congreso NSCAMelina LabroneNo ratings yet
- Efectos Del Ejercicio en Pacientes Mayores Con Diabetes ECADocument13 pagesEfectos Del Ejercicio en Pacientes Mayores Con Diabetes ECAAndrés Araneda VásquezNo ratings yet
- Differential Effects of Strength Training Leading To Failure Versus Not To Failure On Hormonal Responses, Strength, and Muscle Power Gains CHAOS PAINDocument11 pagesDifferential Effects of Strength Training Leading To Failure Versus Not To Failure On Hormonal Responses, Strength, and Muscle Power Gains CHAOS PAINDenilson CostaNo ratings yet
- Strength Training Basics LEERDocument8 pagesStrength Training Basics LEERbichofoodNo ratings yet
- Mechanisms of Blood Flow Restriction: The New Testament: YmposiumDocument8 pagesMechanisms of Blood Flow Restriction: The New Testament: YmposiumRosaneLacerdaNo ratings yet
- Resistance Training Is An Effective Tool Against Metabolic and Frailty SyndromesDocument7 pagesResistance Training Is An Effective Tool Against Metabolic and Frailty SyndromesgiannidietNo ratings yet
- Thematic Poster Bioenergetics and Training: (No Relationships Reported)Document2 pagesThematic Poster Bioenergetics and Training: (No Relationships Reported)pantufoNo ratings yet
- Farup Et Al-2015-Scandinavian Journal of Medicine & Science in SportsDocument10 pagesFarup Et Al-2015-Scandinavian Journal of Medicine & Science in SportsR.No ratings yet
- Pagé-Descarreaux2019 Article EffectsOfSpinalMDocument14 pagesPagé-Descarreaux2019 Article EffectsOfSpinalMdavid ioanaNo ratings yet
- Basic Exercise Physiology: Clinical and Laboratory PerspectivesFrom EverandBasic Exercise Physiology: Clinical and Laboratory PerspectivesNo ratings yet
- How To Carve A Gymnasts Ripped Back With Pull Ups by Anthony Arvanitakis 2016Document1 pageHow To Carve A Gymnasts Ripped Back With Pull Ups by Anthony Arvanitakis 2016Fabiano LacerdaNo ratings yet
- The Importance of Muscular Strength: Training ConsiderationsDocument38 pagesThe Importance of Muscular Strength: Training ConsiderationsFabiano LacerdaNo ratings yet
- Ozaki 2013 e JapDocument9 pagesOzaki 2013 e JapFabiano LacerdaNo ratings yet
- The Influence of Biological Sex and Cuff Width On Muscle Swelling, Echo Intensity, and The Fatigue Response To Blood Flow Restricted ExerciseDocument10 pagesThe Influence of Biological Sex and Cuff Width On Muscle Swelling, Echo Intensity, and The Fatigue Response To Blood Flow Restricted ExerciseFabiano LacerdaNo ratings yet
- Caffeine Supplementation For Powerlifting Competitions: An Evidence-Based ApproachDocument13 pagesCaffeine Supplementation For Powerlifting Competitions: An Evidence-Based ApproachFabiano LacerdaNo ratings yet
- Lower Load Is More Effective Than Higher Load.17Document7 pagesLower Load Is More Effective Than Higher Load.17Fabiano LacerdaNo ratings yet
- Dynamic Joint and Muscle Forces During Knee Isokinetic ExerciseDocument8 pagesDynamic Joint and Muscle Forces During Knee Isokinetic ExerciseFabiano LacerdaNo ratings yet
- Exercise Modification Strategies To Prevent and Train Around Shoulder PainDocument14 pagesExercise Modification Strategies To Prevent and Train Around Shoulder PainFabiano LacerdaNo ratings yet
- Frequencia Na MusculaçãoDocument13 pagesFrequencia Na MusculaçãoFabiano LacerdaNo ratings yet
- The Acute Muscle Swelling Effects of Blood Flow RestrictionDocument11 pagesThe Acute Muscle Swelling Effects of Blood Flow RestrictionFabiano LacerdaNo ratings yet
- Activation of Human Quadriceps Femoris During Isometric, Concentric, and Eccentric ContractionsDocument8 pagesActivation of Human Quadriceps Femoris During Isometric, Concentric, and Eccentric ContractionsFabiano LacerdaNo ratings yet
- The Influence of Exercise Load With and Without Different Levels of Blood Flow Restriction On Acute Changes in Muscle Thickness and LactateDocument7 pagesThe Influence of Exercise Load With and Without Different Levels of Blood Flow Restriction On Acute Changes in Muscle Thickness and LactateFabiano LacerdaNo ratings yet
- Apha 13302 PDFDocument127 pagesApha 13302 PDFFabiano LacerdaNo ratings yet
- Acute Effects of Blood Flow Restriction On Muscle Activity and Endurance During Fatiguing Dynamic Knee Extensions at Low LoadDocument8 pagesAcute Effects of Blood Flow Restriction On Muscle Activity and Endurance During Fatiguing Dynamic Knee Extensions at Low LoadFabiano LacerdaNo ratings yet
- Rapid Increase in Plasma Growth Hormone After Low-Intensity Resistace Exercise With Vascular OcclusionDocument7 pagesRapid Increase in Plasma Growth Hormone After Low-Intensity Resistace Exercise With Vascular OcclusionFabiano LacerdaNo ratings yet
- Acute Skeletal Muscle Responses To Very Low-Load Resistance Exercise With and Without The Application of Blood Flow Restriction in The Upper BodyDocument8 pagesAcute Skeletal Muscle Responses To Very Low-Load Resistance Exercise With and Without The Application of Blood Flow Restriction in The Upper BodyFabiano LacerdaNo ratings yet
- Low Intensity Blood Flow Restriction Training: A Meta-AnalysisDocument12 pagesLow Intensity Blood Flow Restriction Training: A Meta-AnalysisFabiano LacerdaNo ratings yet
- The History, Theory and Practice of Restricted Blood Flow Resistance Training (Rbfrt/Kaatsu)Document10 pagesThe History, Theory and Practice of Restricted Blood Flow Resistance Training (Rbfrt/Kaatsu)Fabiano LacerdaNo ratings yet
- Iso Astm 52701-13 PDFDocument10 pagesIso Astm 52701-13 PDFAhmed LabibNo ratings yet
- Gray Hat Hacking The Ethical Hackers Handbook Sixth Edition Daniel Regalado Full ChapterDocument51 pagesGray Hat Hacking The Ethical Hackers Handbook Sixth Edition Daniel Regalado Full Chaptereugene.poremski145100% (5)
- Going Concern ChecklistDocument1 pageGoing Concern Checklisttunlinoo.067433No ratings yet
- Suicidal Ideation and Behavior in Adults - UpToDate PDFDocument36 pagesSuicidal Ideation and Behavior in Adults - UpToDate PDFLemuel ReyesNo ratings yet
- Phosphorus IndustryDocument38 pagesPhosphorus IndustryS S S REDDY100% (1)
- Cul5a - Lecture - Week 9 - Singaporean Cuisine PDFDocument14 pagesCul5a - Lecture - Week 9 - Singaporean Cuisine PDFJJ GRNo ratings yet
- Company Industry Employee Count Country: Plastic OmniumDocument4 pagesCompany Industry Employee Count Country: Plastic OmniumA AlamNo ratings yet
- WOODRUFF v. UNITED STATES OF AMERICA - Document No. 7Document2 pagesWOODRUFF v. UNITED STATES OF AMERICA - Document No. 7Justia.comNo ratings yet
- CHAPTER LLDocument11 pagesCHAPTER LLDeege BaeNo ratings yet
- T or 1155 Year 1 The Zoo Vet Differentiated Reading Comprehension Activity Ver 8Document9 pagesT or 1155 Year 1 The Zoo Vet Differentiated Reading Comprehension Activity Ver 8Dla SemecoNo ratings yet
- Ztipc 2019Document86 pagesZtipc 2019Journal of Pharmacy & Pharmacognosy ResearchNo ratings yet
- Electrodeposited Coatings of Rhodium For Engineering UseDocument5 pagesElectrodeposited Coatings of Rhodium For Engineering UsesamehNo ratings yet
- The Final Research PaperDocument47 pagesThe Final Research Paperapi-402790311No ratings yet
- Research-2 SynthesisDocument11 pagesResearch-2 SynthesisJesusValenciaNo ratings yet
- Vacuum Circuit Breaker CatalogueDocument11 pagesVacuum Circuit Breaker Cataloguedabs_orangejuice0% (1)
- Physical Evidence in Service MarketingDocument43 pagesPhysical Evidence in Service MarketingXie Qiquan0% (1)
- Wastewater TreatmentDocument60 pagesWastewater TreatmentPC YeapNo ratings yet
- Livro - Egg Parasitoids in Agroecosystems With Emphasis On TrichogrammaDocument481 pagesLivro - Egg Parasitoids in Agroecosystems With Emphasis On TrichogrammaRuan Carlos Mesquita0% (2)
- HU038 - Humes Oasis 2000 Series Owners Manual v6 WEBDocument22 pagesHU038 - Humes Oasis 2000 Series Owners Manual v6 WEBCodrut DavidNo ratings yet
- Visio SM12, RTC048200405UDocument1 pageVisio SM12, RTC048200405UMN Titas TitasNo ratings yet
- CytoskeletonDocument4 pagesCytoskeletonharshika tembhurneNo ratings yet
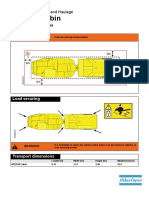
- 9852 2654 01 Transport Instructions MT2010 CabinDocument2 pages9852 2654 01 Transport Instructions MT2010 CabinIH Medrano100% (1)
- 2011UCMC Trauma Care Q&ADocument2 pages2011UCMC Trauma Care Q&ASam CholkeNo ratings yet
- Separation Agreement Template 04Document5 pagesSeparation Agreement Template 04rob De MayoNo ratings yet
- Resources-Pressure Ulcers PresentationDocument10 pagesResources-Pressure Ulcers PresentationVicKy AmaliaNo ratings yet














![(Journal of Strength & Conditioning Research) Schoenfeld BJ, Peterson MD, Ogborn D, Contreras B, Sonmez GT-[Article] Effects of Low- Versus High-Load Resistance Training on Muscle Strength and Hypertr](https://imgv2-2-f.scribdassets.com/img/document/297172026/149x198/5d558be804/1454119074?v=1)