You might also like
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5813)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Ethics For Life PDF DownloadDocument2 pagesEthics For Life PDF DownloadDennis0% (3)
- Difference Between Industrial Wastewater and Municipal WastewaterDocument11 pagesDifference Between Industrial Wastewater and Municipal Wastewatertawsifamin19896% (25)
- Consent Form For Parents and Children: Associate Professor Grace Oakley Graduate School of EducationDocument1 pageConsent Form For Parents and Children: Associate Professor Grace Oakley Graduate School of EducationAnnaJones11No ratings yet
- BrackDocument4 pagesBrackkoebra211No ratings yet
- Mental Fitness: Kristina Coakley HW420-02 Unit 5 ProjectDocument11 pagesMental Fitness: Kristina Coakley HW420-02 Unit 5 ProjectKris CoakleyNo ratings yet
- 260 1086 1 PBDocument9 pages260 1086 1 PBDeva DarshiniNo ratings yet
- AfYWP Small Grants July 2015Document2 pagesAfYWP Small Grants July 2015John BandaNo ratings yet
- Diabetes Home Health RubricDocument13 pagesDiabetes Home Health Rubricapi-372924050No ratings yet
- Efektifitas Media Audio-Visual Pada Kelas Ibu Hamil Terhadap Pengetahuan Dan Sikap Ibu Dalam Pencegahan Komplikasi Kehamilan Dan PersalinanDocument11 pagesEfektifitas Media Audio-Visual Pada Kelas Ibu Hamil Terhadap Pengetahuan Dan Sikap Ibu Dalam Pencegahan Komplikasi Kehamilan Dan PersalinanMitha FebriantiNo ratings yet
- Manual de Servicio XPPDocument38 pagesManual de Servicio XPPCarlos LopezNo ratings yet
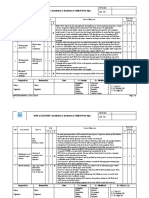
- RA For Installation & Insulation of CHW Pipe SystemDocument4 pagesRA For Installation & Insulation of CHW Pipe SystemDong VanraNo ratings yet
- 10 Surefire Solutions To End The Bedtime BattleDocument3 pages10 Surefire Solutions To End The Bedtime BattleropesNo ratings yet
- Aubert Et Al. 2018Document3 pagesAubert Et Al. 2018LhuissetNo ratings yet
- ZZ ZZZZZZZZ ZZZZZZZZDocument2 pagesZZ ZZZZZZZZ ZZZZZZZZJanderick S EsguerraNo ratings yet
- Mapeh 6 Qi Week8Document23 pagesMapeh 6 Qi Week8Denielle AmomaNo ratings yet
- Pe Health 3 Module q1 Module 1 Claire L. Vince CruzDocument6 pagesPe Health 3 Module q1 Module 1 Claire L. Vince CruzperldeveraNo ratings yet
- Stress Echo Quick ManualDocument3 pagesStress Echo Quick ManualMayrina NDNo ratings yet
- Mcmaster Students Union Dental Claim FormDocument1 pageMcmaster Students Union Dental Claim Form765489No ratings yet
- American Libraries - Design Issue PDFDocument68 pagesAmerican Libraries - Design Issue PDFHayri YildirimNo ratings yet
- Official Control of Food Safety in Lithuania: Import and ExportDocument33 pagesOfficial Control of Food Safety in Lithuania: Import and ExportAbdi HajiNo ratings yet
- Alzheimer and MusicDocument18 pagesAlzheimer and MusicAby RaicouNo ratings yet
- Small Group Anger ManagementDocument4 pagesSmall Group Anger ManagementPaul SarsfieldNo ratings yet
- Abnormalities of TeethDocument24 pagesAbnormalities of TeethRoshni ButalaNo ratings yet
- MAPC 2nd Year Assignments 2019-20Document13 pagesMAPC 2nd Year Assignments 2019-20Jayee's GalleryNo ratings yet
- Stool AssessmentDocument2 pagesStool AssessmentAlex MendozaNo ratings yet
- ECG-Based Biometric Schemes For Healthcare: A Systematic ReviewDocument23 pagesECG-Based Biometric Schemes For Healthcare: A Systematic ReviewInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- IPG Spring 2014 Vegetarian/Vegan TitlesDocument23 pagesIPG Spring 2014 Vegetarian/Vegan TitlesIndependent Publishers GroupNo ratings yet
- List of RefrigerantsDocument16 pagesList of RefrigerantsYasir ButtNo ratings yet
- Jack NewsDocument33 pagesJack NewskndaruNo ratings yet
- Journal EntryDocument4 pagesJournal Entryapi-294972271No ratings yet