You might also like
- Medical-Surgical Nursing ReviewDocument90 pagesMedical-Surgical Nursing Reviewɹǝʍdןnos99% (312)
- Neurology Multiple Choice Questions With Explanations: Volume IFrom EverandNeurology Multiple Choice Questions With Explanations: Volume IRating: 4 out of 5 stars4/5 (7)
- Notes-RJ Speed Seduction Gold WalkupsDocument7 pagesNotes-RJ Speed Seduction Gold Walkupsdulixuexi100% (1)
- Cerebral Herniation Syndromes and Intracranial HypertensionFrom EverandCerebral Herniation Syndromes and Intracranial HypertensionMatthew KoenigNo ratings yet
- How Do You Feel?: An Interoceptive Moment with Your Neurobiological SelfFrom EverandHow Do You Feel?: An Interoceptive Moment with Your Neurobiological SelfRating: 4.5 out of 5 stars4.5/5 (3)
- Polyvagal Theory: A Self-Help Polyvagal Theory Guide to Reduce with Self Help Exercises Anxiety, Depression, Autism, Trauma and Improve Your Life.From EverandPolyvagal Theory: A Self-Help Polyvagal Theory Guide to Reduce with Self Help Exercises Anxiety, Depression, Autism, Trauma and Improve Your Life.Rating: 1 out of 5 stars1/5 (1)
- Banas Bio-Gas PlantDocument30 pagesBanas Bio-Gas Plantjugal rana100% (1)
- Intro To Psychology Crash Course Psychology 1Document3 pagesIntro To Psychology Crash Course Psychology 1Hahaha YeahNo ratings yet
- SS - 578 - 2012 - Use and Maintenance of Fire ExtinguishersDocument24 pagesSS - 578 - 2012 - Use and Maintenance of Fire Extinguishersrasanavaneethan100% (4)
- MS Nursing ReviewerDocument16 pagesMS Nursing ReviewerSunshine SiopaoNo ratings yet
- Medical Surgical Nursing ReviewDocument97 pagesMedical Surgical Nursing ReviewBernadeth Josefa BorelaNo ratings yet
- MS Notes 1Document75 pagesMS Notes 1Marygrace Gan SabanalNo ratings yet
- Perception and CoordinationDocument32 pagesPerception and CoordinationFerdie Marcial B. AureaNo ratings yet
- Medsurg PrintDocument82 pagesMedsurg PrintjennywatsurproblemNo ratings yet
- Medical Surgical: Nervous SystemDocument94 pagesMedical Surgical: Nervous SystemAngelika DomondonNo ratings yet
- Nervous SystemDocument6 pagesNervous Systembritney sookdeoNo ratings yet
- Ms Penta NotesDocument84 pagesMs Penta Notesshenric16No ratings yet
- NeurologyDocument118 pagesNeurologykep1313No ratings yet
- Neuro Study GuideDocument7 pagesNeuro Study GuideNursingSchoolNotes100% (2)
- Nervous System: Effects ofDocument18 pagesNervous System: Effects ofClark LlameraNo ratings yet
- Medical Surgical: SNS (Anti-Cholinergic/adrenergic)Document12 pagesMedical Surgical: SNS (Anti-Cholinergic/adrenergic)Pedro SorianoNo ratings yet
- Physiological Aspects of DeceptionDocument4 pagesPhysiological Aspects of DeceptionALJHON SABINONo ratings yet
- MEdical Surgical REVEWERDocument86 pagesMEdical Surgical REVEWERennaedNo ratings yet
- Medical Surgical: Nervous SystemDocument90 pagesMedical Surgical: Nervous SystemCatherine G. Borras100% (1)
- NS Review: Brain, Spinal Cord, Peripheral NervesDocument12 pagesNS Review: Brain, Spinal Cord, Peripheral Nervesitsme_rizaNo ratings yet
- NervousSystem (6) &Document67 pagesNervousSystem (6) &Irfan Nur Fathur Rahman100% (1)
- International Post-Baccalaureate Pharmd. Program (Ipbp) Internal Assessment (Ia) Exam Study GuideDocument19 pagesInternational Post-Baccalaureate Pharmd. Program (Ipbp) Internal Assessment (Ia) Exam Study Guideapi-3752144No ratings yet
- Medical-Surgical Nursing Lecture NotesDocument90 pagesMedical-Surgical Nursing Lecture NotesJessica AnisNo ratings yet
- Medical and Surgical Nursing Notes For NLEDocument63 pagesMedical and Surgical Nursing Notes For NLEBel Zeta DonaireNo ratings yet
- Medical SurgicalDocument180 pagesMedical SurgicalCorinne Adriano100% (2)
- How The Brain Works: Understanding Brain Function, Thought and PersonalityFrom EverandHow The Brain Works: Understanding Brain Function, Thought and PersonalityNo ratings yet
- Current Concepts in Cardiovascular PhysiologyFrom EverandCurrent Concepts in Cardiovascular PhysiologyOscar GarfeinNo ratings yet
- Electromyography in CNS Disorders: Central EMGFrom EverandElectromyography in CNS Disorders: Central EMGBhagwan T. ShahaniNo ratings yet
- Periphery: How Your Nervous System Predicts and Protects against DiseaseFrom EverandPeriphery: How Your Nervous System Predicts and Protects against DiseaseNo ratings yet
- The Dislocated Brain: Innovation in Traumatic Brain Injury and IrrigationFrom EverandThe Dislocated Brain: Innovation in Traumatic Brain Injury and IrrigationRating: 5 out of 5 stars5/5 (2)
- Somatosensory Teachers Manual: for Somatosensory Science FactsFrom EverandSomatosensory Teachers Manual: for Somatosensory Science FactsNo ratings yet
- Clinical Autonomic and Mitochondrial Disorders: Diagnosis, Prevention, and Treatment for Mind-Body WellnessFrom EverandClinical Autonomic and Mitochondrial Disorders: Diagnosis, Prevention, and Treatment for Mind-Body WellnessNo ratings yet
- Understanding Brain Aging and Dementia: A Life Course ApproachFrom EverandUnderstanding Brain Aging and Dementia: A Life Course ApproachNo ratings yet
- Applied Neurophysiology: With Particular Reference to AnaesthesiaFrom EverandApplied Neurophysiology: With Particular Reference to AnaesthesiaNo ratings yet
- The Brain-Body Connection: Understanding the Impact of Physical Health on Mental HealthFrom EverandThe Brain-Body Connection: Understanding the Impact of Physical Health on Mental HealthNo ratings yet
- The Secret Life of the Brain: Exploring the Mysteries and Wonders of Our Most Vital OrganFrom EverandThe Secret Life of the Brain: Exploring the Mysteries and Wonders of Our Most Vital OrganNo ratings yet
- Neuropathology Simplified: A Guide for Clinicians and NeuroscientistsFrom EverandNeuropathology Simplified: A Guide for Clinicians and NeuroscientistsNo ratings yet
- Neurobiology of Ischemic Brain DamageFrom EverandNeurobiology of Ischemic Brain DamageK. KogureNo ratings yet
- Summary of Herbert Benson, M.D. & Miriam Z. Klipper's The Relaxation ResponseFrom EverandSummary of Herbert Benson, M.D. & Miriam Z. Klipper's The Relaxation ResponseNo ratings yet
- Musculoskeletal Disorders: PhysiologyDocument24 pagesMusculoskeletal Disorders: PhysiologyTanwir HoussaynNo ratings yet
- Cardiovascular DisordersDocument16 pagesCardiovascular DisordersTanwir HoussaynNo ratings yet
- Terms and Conditions for Use of Cim Finance's Electronic PlatformsDocument3 pagesTerms and Conditions for Use of Cim Finance's Electronic PlatformsTanwir HoussaynNo ratings yet
- Diploma in General Nursing PDFDocument7 pagesDiploma in General Nursing PDFTanwir HoussaynNo ratings yet
- Sample ConsentDocument1 pageSample ConsentTanwir HoussaynNo ratings yet
- Assessment of The Elderly 3Document32 pagesAssessment of The Elderly 3Tanwir Houssayn100% (1)
- FAQ Multiscreen PDFDocument4 pagesFAQ Multiscreen PDFTanwir HoussaynNo ratings yet
- Assessment of The Elderly 3Document32 pagesAssessment of The Elderly 3Tanwir Houssayn100% (1)
- FAQs EnglishDocument7 pagesFAQs EnglishTanwir HoussaynNo ratings yet
- Network Marketing BusinessesDocument1 pageNetwork Marketing BusinessessukhberNo ratings yet
- Engineered Plastics GuideDocument1 pageEngineered Plastics GuideKmgsa BandaraNo ratings yet
- Dip Zinc 7-Tank ProcessDocument3 pagesDip Zinc 7-Tank ProcessAmit Chauhan100% (1)
- SCC50 ManualDocument33 pagesSCC50 ManualJesus Alejandro Cochachin VegaNo ratings yet
- Health Impact AssessmentDocument16 pagesHealth Impact AssessmentjrynNo ratings yet
- Instruction: 217 - C Fiber Optic Splice CaseDocument9 pagesInstruction: 217 - C Fiber Optic Splice CaseHữu Khánh NguyễnNo ratings yet
- Analyzing Project ViabilityDocument2 pagesAnalyzing Project ViabilityKumar VikasNo ratings yet
- Starch Industry Effluent Treatment PlantDocument30 pagesStarch Industry Effluent Treatment PlantBSridhar50% (2)
- Induction Training Program For Newly Recruited NursesDocument17 pagesInduction Training Program For Newly Recruited NursesNisha sutariyaNo ratings yet
- Easy Tom Micro and NanoDocument2 pagesEasy Tom Micro and NanoMURALINo ratings yet
- CONTENTS Final Page For IntroductionDocument78 pagesCONTENTS Final Page For Introductionvarshadh varshaNo ratings yet
- ReptileDocument4 pagesReptileDratonius 101No ratings yet
- Tempt Me, Marry MeDocument832 pagesTempt Me, Marry MeCharlotte Selin BautistaNo ratings yet
- 19 - Kyocera Milling - Endmill - Radius - Ball-Nose 2010-2011 (ENG)Document24 pages19 - Kyocera Milling - Endmill - Radius - Ball-Nose 2010-2011 (ENG)karadimasNo ratings yet
- CattabrigaF45 90 120Document21 pagesCattabrigaF45 90 120Fernando William Rivera CuadrosNo ratings yet
- The Practice of Yoga and Its Philosophy FinalDocument23 pagesThe Practice of Yoga and Its Philosophy Finalshwets91No ratings yet
- CALIMOVEDocument46 pagesCALIMOVERasheedAladdinNGuiomala0% (1)
- Pinatubo Eruption Case Study: Disaster Readiness and Risk ReductionDocument5 pagesPinatubo Eruption Case Study: Disaster Readiness and Risk ReductionAndrie PaydoenNo ratings yet
- MDocument47 pagesMKumara55No ratings yet
- LogDocument12 pagesLogrifaniagustinNo ratings yet
- Mini ProjectDocument14 pagesMini ProjectEli Body ButterNo ratings yet
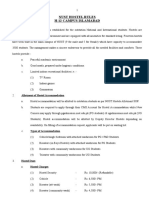
- Nust Hostel Rules H-12 Campus IslamabadDocument10 pagesNust Hostel Rules H-12 Campus IslamabadNeha KhanNo ratings yet
- Petition For Modification of Child Support Order (Administrative Hearing)Document3 pagesPetition For Modification of Child Support Order (Administrative Hearing)Shared EmailNo ratings yet
- Technical Bulletin: Ptfe, 25% Glass Filled Slide PlatesDocument5 pagesTechnical Bulletin: Ptfe, 25% Glass Filled Slide PlatesDavid Luna MolinaNo ratings yet
- IS01 Service Pension OverviewDocument12 pagesIS01 Service Pension OverviewNige McIntoshNo ratings yet
- Basic Counseling SkillsDocument58 pagesBasic Counseling SkillsAnonymous QThGsU93gNo ratings yet