You might also like
- 51895-Case CX160 Crawler ExcavatorDocument634 pages51895-Case CX160 Crawler ExcavatorHarold McNabb100% (5)
- Al Dhahiyah - DC Short Circuit Study-Rev ADocument4 pagesAl Dhahiyah - DC Short Circuit Study-Rev ASomnath DasNo ratings yet
- The Ultimate Guide On How To Boost Your Immune SystemDocument29 pagesThe Ultimate Guide On How To Boost Your Immune SystemALMusriALSudaniNo ratings yet
- The Rough Guide to Beijing (Travel Guide eBook)From EverandThe Rough Guide to Beijing (Travel Guide eBook)Rating: 2 out of 5 stars2/5 (1)
- Certified Pastry Culinarian: Candidate HandbookDocument26 pagesCertified Pastry Culinarian: Candidate HandbookALMusriALSudaniNo ratings yet
- Technical Drawing 7 Module 1Document44 pagesTechnical Drawing 7 Module 1Zhac Domingo Ancheta83% (12)
- Terlaris Shopee Desember 2021Document1,084 pagesTerlaris Shopee Desember 2021Soni ChanNo ratings yet
- ASCO NEC Requirements For SPDDocument7 pagesASCO NEC Requirements For SPDJOSE LUIS FALCON CHAVEZNo ratings yet
- Step 1: Initial CC Pre-Approval Application: Personal InformationDocument2 pagesStep 1: Initial CC Pre-Approval Application: Personal InformationALMusriALSudaniNo ratings yet
- Certified Culinary Competition ApplicationDocument3 pagesCertified Culinary Competition ApplicationShahzad SheziiNo ratings yet
- Veteran Population by State: Fiscal Year 2015Document1 pageVeteran Population by State: Fiscal Year 2015AlexandruBroNo ratings yet
- Employment Documentation Form: American Culinary FederationDocument1 pageEmployment Documentation Form: American Culinary FederationALMusriALSudaniNo ratings yet
- 2013 02 Frames Rev 10 06 12Document125 pages2013 02 Frames Rev 10 06 12mert çelikNo ratings yet
- Case Studies of Design-Build Project Delivery For Highway PavementsDocument36 pagesCase Studies of Design-Build Project Delivery For Highway PavementsAna Paula De BaccoNo ratings yet
- Northeast South North Central West: FL TXDocument1 pageNortheast South North Central West: FL TXPetrutNo ratings yet
- Longitudinal Joint Workshop Slides 3 2017 1Document214 pagesLongitudinal Joint Workshop Slides 3 2017 1m.basim.technitalNo ratings yet
- 2018 Carter's RealEstate Brochure v5 PDFDocument2 pages2018 Carter's RealEstate Brochure v5 PDFAmanda Logan100% (1)
- Technical News: Adoption of The 2017 National Electric CodeDocument3 pagesTechnical News: Adoption of The 2017 National Electric CodeFelipe GustavoNo ratings yet
- OG at Glance CP 7844Document1 pageOG at Glance CP 7844mybooks1401No ratings yet
- Numeric Change Resident Population All Stateapport2010 Map2Document1 pageNumeric Change Resident Population All Stateapport2010 Map2Helen BennettNo ratings yet
- NPMS HeatMap GTIncidents WPointsDocument1 pageNPMS HeatMap GTIncidents WPoints01CaUKM Zhaffran AsyrafNo ratings yet
- 50-State Analysis: School Attendance Age LimitsDocument5 pages50-State Analysis: School Attendance Age LimitsshahNo ratings yet
- All About Misty Copeland: Name DateDocument2 pagesAll About Misty Copeland: Name DateY Rachel KöybaşıNo ratings yet
- States in The USADocument1 pageStates in The USAVeronicaGelfgren100% (2)
- Intermediate Directions: U. S. CitiesDocument2 pagesIntermediate Directions: U. S. CitiesNouvel Malin BashaNo ratings yet
- ED508343Document52 pagesED508343Noura AdhamNo ratings yet
- Natural Gas PricesDocument3 pagesNatural Gas PricesdownbuliaoNo ratings yet
- 9.28 SHAP WebinarDocument65 pages9.28 SHAP Webinarcmiller5143No ratings yet
- Total Fertility Rates by State and Race and Hispanic Origin: United States, 2017Document11 pagesTotal Fertility Rates by State and Race and Hispanic Origin: United States, 2017WXYZ-TV Channel 7 DetroitNo ratings yet
- What Your Council Should Be Doing Right Now!: Tom Mccaffrey VP, Fraternal OperationsDocument70 pagesWhat Your Council Should Be Doing Right Now!: Tom Mccaffrey VP, Fraternal OperationsRamon BrionesNo ratings yet
- Alphas Are No OmegasDocument5 pagesAlphas Are No OmegascontentionNo ratings yet
- Is This A Kind of FutureDocument3 pagesIs This A Kind of FuturecontentionNo ratings yet
- Opening HorizonsDocument5 pagesOpening HorizonsSuperfonfyNo ratings yet
- Beauty Is LonesomeDocument2 pagesBeauty Is LonesomecontentionNo ratings yet
- Field of DreamsDocument6 pagesField of DreamscontentionNo ratings yet
- Skies of A Deep PurpleDocument4 pagesSkies of A Deep PurplecontentionNo ratings yet
- Maths For Student With DisabilitiesDocument183 pagesMaths For Student With DisabilitiesYing Thong ChinNo ratings yet
- Map 5 Fine Scale WildlifeDocument1 pageMap 5 Fine Scale WildlifeapakuniNo ratings yet
- EQEQEDocument1 pageEQEQESHIELAMAE GREGORIONo ratings yet
- Census Block GRP 7Document1 pageCensus Block GRP 7bfloblockclubsNo ratings yet
- Description: Tags: REL 2007017Document35 pagesDescription: Tags: REL 2007017anon-376992No ratings yet
- Plumbing 3Document1 pagePlumbing 3Shia CastañedaNo ratings yet
- Price Data Quality Report: Chart Displaying Price Data Quality Per Issue Type For The Month ofDocument2 pagesPrice Data Quality Report: Chart Displaying Price Data Quality Per Issue Type For The Month ofShivangi TanejaNo ratings yet
- Cancer Prevention and Early DetectonDocument64 pagesCancer Prevention and Early DetectonRicho WijayaNo ratings yet
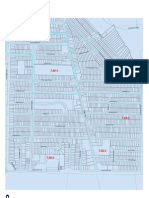
- Central Business DistrictDocument1 pageCentral Business DistrictjasonswallaceNo ratings yet
- Paxtang Zoning MapDocument1 pagePaxtang Zoning MapPennLiveNo ratings yet
- State Puppy Mill LawsDocument1 pageState Puppy Mill LawsFOX 17 NewsNo ratings yet
- Regional Briefing Central U.S.: Dave Zwicke, Sr. Director & Regional EconomistDocument25 pagesRegional Briefing Central U.S.: Dave Zwicke, Sr. Director & Regional EconomistStanislav ZemskovNo ratings yet
- Elysia-2 Brochure PDFDocument8 pagesElysia-2 Brochure PDFAniruddha JaydeokarNo ratings yet
- Cartographywk 1 No 2Document1 pageCartographywk 1 No 2api-534097793No ratings yet
- Lilydale Warburton Rail Trail Pocket Guide 2017Document2 pagesLilydale Warburton Rail Trail Pocket Guide 2017ALNo ratings yet
- DT One Coverage MapDocument18 pagesDT One Coverage Mapamrozaki.aauNo ratings yet
- Planning A Special EventDocument8 pagesPlanning A Special EventctyvteNo ratings yet
- Michigan MileDocument1 pageMichigan MileNBC 25 / FOX 66 NewsNo ratings yet
- UST MUNIF IbadahDocument3 pagesUST MUNIF IbadahFaiz MaulanaNo ratings yet
- Instalasi MainLine Air PPR PN 10 - 22 - 1 .24Document1 pageInstalasi MainLine Air PPR PN 10 - 22 - 1 .24edy.sustiyono0408No ratings yet
- Gig Car Share Home Zone 2017-3-16 PDFDocument1 pageGig Car Share Home Zone 2017-3-16 PDFRecordTrac - City of OaklandNo ratings yet
- 026 Abd BasementDocument1 page026 Abd BasementdikkiNo ratings yet
- UCC1 - Fact Sheet - 2022 - ADADocument1 pageUCC1 - Fact Sheet - 2022 - ADAmadamed4uNo ratings yet
- In Action: Wipe Out Vandalism and GraffitiDocument8 pagesIn Action: Wipe Out Vandalism and Graffitiapi-686827362No ratings yet
- US Heat MapDocument9 pagesUS Heat MapApril Ubay AlibayanNo ratings yet
- Site Comparison 2023Document1 pageSite Comparison 2023HarryNo ratings yet
- Me 3344Document1 pageMe 3344Jithin P KNo ratings yet
- Invertor Samsung IP BOARD IP INVERTER PDFDocument1 pageInvertor Samsung IP BOARD IP INVERTER PDFseggurNo ratings yet
- Directions: North, South, East or West? PDFDocument1 pageDirections: North, South, East or West? PDFNini CarrilloNo ratings yet
- Good Refurbishment Practice: Global Medical Imaging IndustryDocument20 pagesGood Refurbishment Practice: Global Medical Imaging IndustryALMusriALSudaniNo ratings yet
- Remanufacturing and Product DesignDocument77 pagesRemanufacturing and Product DesignALMusriALSudaniNo ratings yet
- Federation of Engine Re-Manufacturers LTD: This Copy Dated January 2017 Supercedes All Previous VersionsDocument8 pagesFederation of Engine Re-Manufacturers LTD: This Copy Dated January 2017 Supercedes All Previous VersionsALMusriALSudaniNo ratings yet
- Candidate Handbook American Culinary Federation PDFDocument32 pagesCandidate Handbook American Culinary Federation PDFALMusriALSudaniNo ratings yet
- Certification Cost Estimates: Member Estimated CostsDocument1 pageCertification Cost Estimates: Member Estimated CostsALMusriALSudaniNo ratings yet
- Shelf Life, Storage, and Reconditioning of ESAB Welding Filler MetalsDocument3 pagesShelf Life, Storage, and Reconditioning of ESAB Welding Filler MetalsALMusriALSudaniNo ratings yet
- Personal Certified Chef & Personal Certified Executive Chef: Candidate HandbookDocument25 pagesPersonal Certified Chef & Personal Certified Executive Chef: Candidate HandbookALMusriALSudaniNo ratings yet
- Candidate Handbook CcaDocument16 pagesCandidate Handbook CcaALMusriALSudaniNo ratings yet
- Certification Education 30 Hour Course Requirements Experience Additional RequirementsDocument1 pageCertification Education 30 Hour Course Requirements Experience Additional RequirementsALMusriALSudaniNo ratings yet
- 2018 CEC® Certificant Bulletin: Statistics For The ACF Certified Executive Chef® (CEC®) Credential Are Issued AnnuallyDocument1 page2018 CEC® Certificant Bulletin: Statistics For The ACF Certified Executive Chef® (CEC®) Credential Are Issued AnnuallyALMusriALSudaniNo ratings yet
- Certified Working Pastry Chef: Candidate HandbookDocument25 pagesCertified Working Pastry Chef: Candidate HandbookALMusriALSudaniNo ratings yet
- Certified Sous Chef: Candidate HandbookDocument24 pagesCertified Sous Chef: Candidate HandbookALMusriALSudaniNo ratings yet
- Electrhaz Handouts PDFDocument9 pagesElectrhaz Handouts PDFALMusriALSudaniNo ratings yet
- Certified Master Chef: Candidate Handbook Segment 2Document22 pagesCertified Master Chef: Candidate Handbook Segment 2ALMusriALSudaniNo ratings yet
- Activity Option A Student Copy Wet Conditions / Ground Fault Circuit InterruptersDocument7 pagesActivity Option A Student Copy Wet Conditions / Ground Fault Circuit InterruptersALMusriALSudaniNo ratings yet
- Solar Photovoltaic:: Fundamentals, Technologies and ApplicationsDocument45 pagesSolar Photovoltaic:: Fundamentals, Technologies and ApplicationsALMusriALSudaniNo ratings yet
- Accident Summary No. 11: Brief Description of AccidentDocument8 pagesAccident Summary No. 11: Brief Description of AccidentALMusriALSudaniNo ratings yet
- 12DEC Eat These Foods To Boost Your Immune SystemDocument2 pages12DEC Eat These Foods To Boost Your Immune SystemALMusriALSudaniNo ratings yet
- Strengthen Your Immune System: Exercise ConsistentlyDocument2 pagesStrengthen Your Immune System: Exercise ConsistentlyALMusriALSudaniNo ratings yet
- Fall Hazards Student Copy LADDER SAFETY: What's Wrong With This Picture?Document5 pagesFall Hazards Student Copy LADDER SAFETY: What's Wrong With This Picture?ALMusriALSudaniNo ratings yet
- Natural Ways To Boost Your Immune Health: Green TeaDocument5 pagesNatural Ways To Boost Your Immune Health: Green TeaALMusriALSudaniNo ratings yet
- Build Your Immune System With Good NutritionDocument2 pagesBuild Your Immune System With Good NutritionALMusriALSudaniNo ratings yet
- Feeding The Immune SystemDocument12 pagesFeeding The Immune SystemALMusriALSudaniNo ratings yet
- Students' Point of View On The Use of Whatsapp Group To Elevate Writing AbilityDocument7 pagesStudents' Point of View On The Use of Whatsapp Group To Elevate Writing AbilityAl HakimNo ratings yet
- Wienold MFC Brochure 2018Document4 pagesWienold MFC Brochure 2018sebastianavinaNo ratings yet
- Towards Establishing A Framework For Managing Trusted Records in The Electronic EnvironmentDocument12 pagesTowards Establishing A Framework For Managing Trusted Records in The Electronic EnvironmentRina RakhmawatiNo ratings yet
- New Lucena National Comprehensive High: SchoolDocument8 pagesNew Lucena National Comprehensive High: Schoolriverastudy01No ratings yet
- Digital MarketingDocument8 pagesDigital MarketingYounus ahmedNo ratings yet
- InfertilityDocument29 pagesInfertilityCristina StanleeNo ratings yet
- Material Downloaded From - 1 / 4Document4 pagesMaterial Downloaded From - 1 / 4NihalSoniNo ratings yet
- 01 PHP Part - 07Document18 pages01 PHP Part - 07Fans DodNo ratings yet
- Lifting Operations Onboard ShipDocument3 pagesLifting Operations Onboard ShipGiorgi KandelakiNo ratings yet
- 32LD867HTDocument47 pages32LD867HTlaboratorio fercorNo ratings yet
- WorkApps ChatDocument18 pagesWorkApps ChatRuletaNo ratings yet
- Service Support Catalog 2020Document178 pagesService Support Catalog 2020Xin GaoNo ratings yet
- Yb21 10 WNF 210613Document80 pagesYb21 10 WNF 210613era wahyu santosoNo ratings yet
- GeotecniaDocument35 pagesGeotecniaRaquel OliveiraNo ratings yet
- 1 2 Performing Mensuration and CalculationDocument4 pages1 2 Performing Mensuration and CalculationRonaldo CruzNo ratings yet
- Brentwood STAR ReportDocument2 pagesBrentwood STAR ReportShahab Z AhmedNo ratings yet
- Practical 10 - Shear CentreDocument4 pagesPractical 10 - Shear CentreTbyTanNo ratings yet
- Annex A - Grant Application FormDocument46 pagesAnnex A - Grant Application FormtijanagruNo ratings yet
- AS - CBSE - X - Math - Practise - Standard 2Document11 pagesAS - CBSE - X - Math - Practise - Standard 2Kattirsitti Jeet Govind100% (1)
- Syllabus of 2nd Year LMD English at ENS Algeria Semster 4Document363 pagesSyllabus of 2nd Year LMD English at ENS Algeria Semster 4belbachir100% (1)
- KK CoffeeStout TentCardsDocument4 pagesKK CoffeeStout TentCardsHeris padilahNo ratings yet
- JHS LCP English Grade 7 10Document25 pagesJHS LCP English Grade 7 10Daryl RiveraNo ratings yet
- 5 GDocument9 pages5 GsanchitNo ratings yet
- Maxxxxxx App FormDocument4 pagesMaxxxxxx App Formanorue maxwellNo ratings yet
- Project Guidelines - MGA 708Document14 pagesProject Guidelines - MGA 708AnushkaNo ratings yet
- ASHRAE Journal - VAV Box Duct Design - TaylorDocument8 pagesASHRAE Journal - VAV Box Duct Design - TaylorsajuhereNo ratings yet
- Keys Test 2 - Lis Batch 2Document8 pagesKeys Test 2 - Lis Batch 2Đoàn MiNo ratings yet