You might also like
- Covid 19 Patients' Clinical Characteristics, Discharge Rate, and Fatality Rate of Meta AnalysisDocument7 pagesCovid 19 Patients' Clinical Characteristics, Discharge Rate, and Fatality Rate of Meta AnalysisDelfina RubioNo ratings yet
- JMV 26509Document12 pagesJMV 26509a27091No ratings yet
- Efficacy of Various Treatment Modalities For nCOV-2019: A Systematic Review and Meta-AnalysisDocument21 pagesEfficacy of Various Treatment Modalities For nCOV-2019: A Systematic Review and Meta-AnalysisJuan José Cardona GiraldoNo ratings yet
- Efficacy of Various Treatment Modalities For nCOV-2019: A Systematic Review and Meta-AnalysisDocument5 pagesEfficacy of Various Treatment Modalities For nCOV-2019: A Systematic Review and Meta-AnalysisJuan José Cardona GiraldoNo ratings yet
- Dysregulation of Immune Response in Patients With Coronavirus 2019 (COVID-19) in Wuhan, ChinaDocument7 pagesDysregulation of Immune Response in Patients With Coronavirus 2019 (COVID-19) in Wuhan, Chinacika daraNo ratings yet
- The Influence of Comorbidity On The Severity of CODocument13 pagesThe Influence of Comorbidity On The Severity of COBurhan AquariusNo ratings yet
- Risk Factors of Healthcare Workers With Corona Virus Disease 2019: A Retrospective Cohort Study in A Designated Hospital of Wuhan in ChinaDocument18 pagesRisk Factors of Healthcare Workers With Corona Virus Disease 2019: A Retrospective Cohort Study in A Designated Hospital of Wuhan in ChinakazifsalahinNo ratings yet
- DDR 21762Document20 pagesDDR 21762mohammad kazem HajianiNo ratings yet
- A Systematic Meta Analysis of Immune Signatures in Patients With Covid-19Document40 pagesA Systematic Meta Analysis of Immune Signatures in Patients With Covid-19reginabrizolaraNo ratings yet
- Journal of Infection and Public Health: Qianqian Cui, Zengyun Hu, Yingke Li, Junmei Han, Zhidong Teng, Jing QianDocument7 pagesJournal of Infection and Public Health: Qianqian Cui, Zengyun Hu, Yingke Li, Junmei Han, Zhidong Teng, Jing Qianشبلي غرايبهNo ratings yet
- The Incubation Period Distribution of Coronavirus Disease 2019: A Systematic Review and Meta-AnalysisDocument9 pagesThe Incubation Period Distribution of Coronavirus Disease 2019: A Systematic Review and Meta-AnalysiseswaynedNo ratings yet
- Diabetes & Metabolic Syndrome: Clinical Research & ReviewsDocument5 pagesDiabetes & Metabolic Syndrome: Clinical Research & ReviewsRea AuliaNo ratings yet
- Diabetes & Metabolic Syndrome: Clinical Research & ReviewsDocument8 pagesDiabetes & Metabolic Syndrome: Clinical Research & Reviewslama rashedNo ratings yet
- Journal Pone 0250602Document21 pagesJournal Pone 0250602Syed Rehan AghaNo ratings yet
- Clinical Microbiology and InfectionDocument6 pagesClinical Microbiology and InfectionMiguel AngelNo ratings yet
- Benefit of Fasting 30 DaysDocument3 pagesBenefit of Fasting 30 DayshvtdNo ratings yet
- Prevalence of Comorbidities in COVID-19 Patients: A Systematic Review and Meta-AnalysisDocument13 pagesPrevalence of Comorbidities in COVID-19 Patients: A Systematic Review and Meta-AnalysisMas WiNo ratings yet
- Sars-Cov-2 Vaccine Effectiveness Against Infection, Symptomatic and Severe Covid-19: A Systematic Review and Meta-AnalysisDocument12 pagesSars-Cov-2 Vaccine Effectiveness Against Infection, Symptomatic and Severe Covid-19: A Systematic Review and Meta-AnalysisChengwustZhangNo ratings yet
- Sequelae of COVID-19 Among Previously Hospitalized Patients Up To 1 Year After Discharge - A Systematic Review and Meta-AnalysisDocument43 pagesSequelae of COVID-19 Among Previously Hospitalized Patients Up To 1 Year After Discharge - A Systematic Review and Meta-AnalysisRicardo Pariona LlanosNo ratings yet
- Impact of COVID-19 Pandemic On Mental Health in The General Population - A Systematic ReviewDocument36 pagesImpact of COVID-19 Pandemic On Mental Health in The General Population - A Systematic ReviewCharlesNo ratings yet
- Dong J - Prediction For Progression Risk in Patients With COVID - 19 Pneumonia The CALL ScoreDocument7 pagesDong J - Prediction For Progression Risk in Patients With COVID - 19 Pneumonia The CALL ScoreMercedes Ah CardenasNo ratings yet
- 1 s2.0 S1063458421009341 MainDocument11 pages1 s2.0 S1063458421009341 MainDhev GianfrancoNo ratings yet
- Association of The Insulin Resistance Marker Tyg Index With The Severity and Mortality of Covid-19Document8 pagesAssociation of The Insulin Resistance Marker Tyg Index With The Severity and Mortality of Covid-19LolaNo ratings yet
- JMV 25961Document9 pagesJMV 25961damar soebandNo ratings yet
- Obesity Aggravates COVID-19: A Systematic Review and Meta-AnalysisDocument20 pagesObesity Aggravates COVID-19: A Systematic Review and Meta-AnalysisLuis C Ribon VNo ratings yet
- COVID-19 ICU and Mechanical Ventilation Patient Characteristics and Outcomes-A Systematic Review and Meta-AnalysisDocument16 pagesCOVID-19 ICU and Mechanical Ventilation Patient Characteristics and Outcomes-A Systematic Review and Meta-AnalysisTai rascunhos TaiNo ratings yet
- Identification of COVID-19 Clinical Phenotypes by Principal Component Analysis-Based Cluster AnalysisDocument7 pagesIdentification of COVID-19 Clinical Phenotypes by Principal Component Analysis-Based Cluster Analysisnoor khairaniNo ratings yet
- Correlation of Demographic Profile With Laboratory Parameters and Clinical Factors As Predictors of Covid-19 Severity: A Comprehensive AnalysisDocument7 pagesCorrelation of Demographic Profile With Laboratory Parameters and Clinical Factors As Predictors of Covid-19 Severity: A Comprehensive Analysisindex PubNo ratings yet
- Systemic Immune-In Ammatory Index Predicts Prognosis of Patients With COVID-19: A Retrospective StudyDocument37 pagesSystemic Immune-In Ammatory Index Predicts Prognosis of Patients With COVID-19: A Retrospective StudyJuliana SanjayaNo ratings yet
- Guo-Li2021 Article ModelingAndDynamicAnalysisOfNoDocument26 pagesGuo-Li2021 Article ModelingAndDynamicAnalysisOfNoAmido MussaNo ratings yet
- Scab 066Document12 pagesScab 066Djfiory YonutzNo ratings yet
- ArticleText 82443 1 10 20200404Document8 pagesArticleText 82443 1 10 20200404Avi KhannaNo ratings yet
- Clinical Characteristics and Durations of Hospitalized Patients With COVID-19 in BeijingDocument18 pagesClinical Characteristics and Durations of Hospitalized Patients With COVID-19 in BeijingTOMMYNo ratings yet
- Sarah GorstDocument19 pagesSarah GorstDaniel J Alejos CNo ratings yet
- Ongoing Living Update of Potential COVID-19 Therapeutics: Summary of Rapid Systematic ReviewsDocument25 pagesOngoing Living Update of Potential COVID-19 Therapeutics: Summary of Rapid Systematic ReviewsjessicaNo ratings yet
- 1 s2.0 S2213219821012022 MainDocument10 pages1 s2.0 S2213219821012022 Main茹光毅No ratings yet
- The Impact of COVID-19 On College Students' Physical Activity - A Protocol For Systematic Review and Meta-AnalysisDocument4 pagesThe Impact of COVID-19 On College Students' Physical Activity - A Protocol For Systematic Review and Meta-AnalysisSujit reddyNo ratings yet
- Diagnostic Utility of Clinical Laboratory Data Determinationsfor Patients With The Severe COVID 19Document6 pagesDiagnostic Utility of Clinical Laboratory Data Determinationsfor Patients With The Severe COVID 19junior rodriguesNo ratings yet
- MainDocument19 pagesMainnisalazarvNo ratings yet
- Antibiotico CovidDocument12 pagesAntibiotico CovidPaul ArtigasNo ratings yet
- Chloroquine and Hydroxychloroquine For The TreatmentDocument7 pagesChloroquine and Hydroxychloroquine For The TreatmentbcmariaNo ratings yet
- Covid 19 TreatmentDocument18 pagesCovid 19 TreatmentwiwiNo ratings yet
- COVID GuidelinesDocument13 pagesCOVID GuidelinesAlexandra StuparuNo ratings yet
- Henry2020Document8 pagesHenry2020TisaNo ratings yet
- Aberrant Hyperactivation of Cytotoxic T Cell As - 2020 - International JournalDocument9 pagesAberrant Hyperactivation of Cytotoxic T Cell As - 2020 - International Journalmohd mizam saidi aliNo ratings yet
- Bacterial Co-Infection and Secondary Infection in Patients With COVID19 A Living Rapid Review and Meta-AnalysisDocument8 pagesBacterial Co-Infection and Secondary Infection in Patients With COVID19 A Living Rapid Review and Meta-AnalysisSundas EjazNo ratings yet
- Ijbsv 17 P 1581Document7 pagesIjbsv 17 P 1581sarahulfaaNo ratings yet
- Indian Clinical Trials On COVID-19: A Review of Clinical Trials Registry of India (CTRI)Document21 pagesIndian Clinical Trials On COVID-19: A Review of Clinical Trials Registry of India (CTRI)Haryadi WidodoNo ratings yet
- Association of Procalcitonin Levels With The Progression and Prognosis of Hospitalized Patients With COVID-19Document9 pagesAssociation of Procalcitonin Levels With The Progression and Prognosis of Hospitalized Patients With COVID-19Dian Putri NingsihNo ratings yet
- The Impact of Dementia On The Clinical Outcome of COVID-19 - A Systematic Review and Meta-Analysis - IOS PressDocument16 pagesThe Impact of Dementia On The Clinical Outcome of COVID-19 - A Systematic Review and Meta-Analysis - IOS PressDino AdijayaNo ratings yet
- New Insights of Emerging Sars-Cov-2: Epidemiology, Etiology, Clinical Features, Clinical Treatment, and PreventionDocument22 pagesNew Insights of Emerging Sars-Cov-2: Epidemiology, Etiology, Clinical Features, Clinical Treatment, and PreventionWendi IochNo ratings yet
- Impact of Corticosteroid Therapy On Outcomes of Persons With Sars-Cov-2, Sars-Cov, or Mers-Cov Infection: A Systematic Review and Meta-AnalysisDocument9 pagesImpact of Corticosteroid Therapy On Outcomes of Persons With Sars-Cov-2, Sars-Cov, or Mers-Cov Infection: A Systematic Review and Meta-AnalysisMax CamargoNo ratings yet
- Best Practice & Research: Clinical RheumatologyDocument18 pagesBest Practice & Research: Clinical Rheumatologyclaude fernaNo ratings yet
- Ireland LongCovDocument19 pagesIreland LongCovTochukwu IgboanugoNo ratings yet
- Severe Covid and Autoimmune DiseaseDocument4 pagesSevere Covid and Autoimmune DiseaseYudha SatriaNo ratings yet
- Nindi Arnanda Model Research Proposal 14 Oct 2021Document9 pagesNindi Arnanda Model Research Proposal 14 Oct 2021nindi arnandaNo ratings yet
- Liver Injury Is Associated With Severe Coronavirus Disease 2019 (COVID-19) Infection: A Systematic Review and Meta-Analysis of Retrospective StudiesDocument12 pagesLiver Injury Is Associated With Severe Coronavirus Disease 2019 (COVID-19) Infection: A Systematic Review and Meta-Analysis of Retrospective StudiesBremel Gallegos SegundoNo ratings yet
- Risk Factors For Mortality in Patients With Coronavirus Disease 2019 COVID 19 Infection A Systematic Review and Meta Analysis of Observational StudiesDocument10 pagesRisk Factors For Mortality in Patients With Coronavirus Disease 2019 COVID 19 Infection A Systematic Review and Meta Analysis of Observational StudiesAnak MuadzNo ratings yet
- Contoh Jurnal PromkesDocument15 pagesContoh Jurnal Promkeshusna arwaNo ratings yet
- COVID-19 Mortality Review in Malaysia & Updates on Clinical Management of COVID-19From EverandCOVID-19 Mortality Review in Malaysia & Updates on Clinical Management of COVID-19No ratings yet
- Black People Covid DeathDocument10 pagesBlack People Covid DeathJuan c ANo ratings yet
- 2020 Prevalence, Severity and Mortality Associated With COPD and Smoking in Patients With COVID-19 A Rapid Systematic Review and Meta AnalysisDocument13 pages2020 Prevalence, Severity and Mortality Associated With COPD and Smoking in Patients With COVID-19 A Rapid Systematic Review and Meta AnalysisNataliaPalacínBernalNo ratings yet
- Black People Covid DeathDocument10 pagesBlack People Covid DeathJuan c ANo ratings yet
- Jurnal 2 TridaraDocument12 pagesJurnal 2 TridaraLuckyNawaNo ratings yet
- Jurnal 1 TridaraDocument8 pagesJurnal 1 TridaraLuckyNawaNo ratings yet
- Jurnal 5 TridaraDocument5 pagesJurnal 5 TridaraLuckyNawaNo ratings yet
- Tridara Februaluki 09180000069 KMBDocument11 pagesTridara Februaluki 09180000069 KMBTri DarafebrualukiNo ratings yet
- Jurnal 6 TridaraDocument9 pagesJurnal 6 TridaraLuckyNawaNo ratings yet
- Harper's Illustrated Biochemistry - Hormonal Control in Signal TransductionDocument18 pagesHarper's Illustrated Biochemistry - Hormonal Control in Signal TransductionDr Sanjeeb Kumar Dey BaidyaNo ratings yet
- Case Study-Cereal PartnersDocument5 pagesCase Study-Cereal PartnersTariq MehmoodNo ratings yet
- Bba-Mq Tias 2023-24Document2 pagesBba-Mq Tias 2023-24Chris PresleyNo ratings yet
- Deguzman Vs ComelecDocument3 pagesDeguzman Vs ComelecEsnani MaiNo ratings yet
- XDocument2 pagesXSophiaFrancescaEspinosaNo ratings yet
- Filcro - LabrevDocument19 pagesFilcro - LabrevKim ArniñoNo ratings yet
- M.S Engineering (Aerospace) Application Form: For Office UseDocument4 pagesM.S Engineering (Aerospace) Application Form: For Office Useshashasha123No ratings yet
- CRC Ace Far 1ST PBDocument9 pagesCRC Ace Far 1ST PBJohn Philip Castro100% (1)
- Making Friends British English StudentDocument8 pagesMaking Friends British English StudentMily ArrayaNo ratings yet
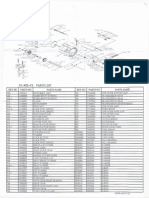
- Okuma CL302L Parts List & ManualDocument3 pagesOkuma CL302L Parts List & Manualcoolestkiwi100% (1)
- Pre-Int Unit 3aDocument2 pagesPre-Int Unit 3aKarla Chong Bejarano0% (1)
- Package Suppdists': R Topics DocumentedDocument26 pagesPackage Suppdists': R Topics DocumentedHector Alejandro Cabezas CasanuevaNo ratings yet
- Executive MBA Project - Self Help Allowance - FinalDocument55 pagesExecutive MBA Project - Self Help Allowance - FinalKumar SourabhNo ratings yet
- Kraft Foods Inc. in FranceDocument25 pagesKraft Foods Inc. in Francevishal211086No ratings yet
- Fleet Management 101 Training Part 1:: Presenters Gary Hatfield, Mercury Associates William Gookin, Mercury AssociatesDocument22 pagesFleet Management 101 Training Part 1:: Presenters Gary Hatfield, Mercury Associates William Gookin, Mercury AssociatesAdolphe Hotereshi100% (1)
- FSED 1F Application Form FSEC For Building Permit Rev02Document2 pagesFSED 1F Application Form FSEC For Building Permit Rev02Angelito RegulacionNo ratings yet
- Gerry Mulligan DiscographyDocument491 pagesGerry Mulligan DiscographyIan SinclairNo ratings yet
- Gibbs VerBeek CorrespondenceDocument3 pagesGibbs VerBeek CorrespondenceWXMINo ratings yet
- RAB PLTS Hybrid 1kWp-ScheneiderDocument4 pagesRAB PLTS Hybrid 1kWp-ScheneiderilhamNo ratings yet
- Mcmurdo S4 SART User GuideDocument20 pagesMcmurdo S4 SART User Guidesathish kumar100% (2)
- Literatur Riview Tentang Faktor Penyebab Klaim Tidak Layak Bayar BPJS Kesehatan Di Rumah Sakit Tahun 2020Document8 pagesLiteratur Riview Tentang Faktor Penyebab Klaim Tidak Layak Bayar BPJS Kesehatan Di Rumah Sakit Tahun 2020Maulida LutfiaNo ratings yet
- Laboratory Activity 1CDocument4 pagesLaboratory Activity 1CAini HasshimNo ratings yet
- Procreate GuideDocument283 pagesProcreate GuideDiego D'Andrea100% (2)
- Ac-Ppt On Crystal OscillatorDocument10 pagesAc-Ppt On Crystal OscillatorRitika SahuNo ratings yet
- QQQQ PDFDocument484 pagesQQQQ PDFSagor Saha100% (1)
- 50 Studies Every Anesthesiologist Shoud Know 2019Document305 pages50 Studies Every Anesthesiologist Shoud Know 2019pcut100% (2)
- Forcep DeliveryDocument11 pagesForcep DeliveryNishaThakuriNo ratings yet
- PHY130 Lab Report 2Document7 pagesPHY130 Lab Report 2Declan Gale Anak DellyNo ratings yet