You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
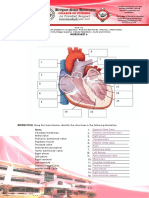
- Cardiovascular WorksheetDocument9 pagesCardiovascular WorksheetPANGPANGDEO Shanne Delle B.No ratings yet
- What Are Ketones, and Why Are They Dangerous?Document4 pagesWhat Are Ketones, and Why Are They Dangerous?john mendozaNo ratings yet
- The Use of Hematocrit Centrifuge by Using A Blood Sample of S.TR Medical Laboratory Technology StudentsDocument12 pagesThe Use of Hematocrit Centrifuge by Using A Blood Sample of S.TR Medical Laboratory Technology StudentsAnisa IstiqomahNo ratings yet
- L11 - Practice Q - HBDocument4 pagesL11 - Practice Q - HBEvan YEUNG [09N12]No ratings yet
- The Triglyceride-to-HDL Cholesterol RatioDocument6 pagesThe Triglyceride-to-HDL Cholesterol RatioArthurNo ratings yet
- Angioprimhandout 1Document2 pagesAngioprimhandout 1Pieter SteenkampNo ratings yet
- Identifying MacromoleculesDocument21 pagesIdentifying MacromoleculesMarkJasperCalabanoNo ratings yet
- Welcome To Big-City Lab Services Right in Your NeighborhoodDocument2 pagesWelcome To Big-City Lab Services Right in Your NeighborhoodstndNo ratings yet
- Lab HandbookDocument122 pagesLab Handbookbiotech department100% (1)
- Physiology of Body FluidsDocument23 pagesPhysiology of Body FluidsRamadan Physiology100% (1)
- Bempedoic Acid For Treating Hypercholesterolemia: Samar Al-Omair, B.SCDocument20 pagesBempedoic Acid For Treating Hypercholesterolemia: Samar Al-Omair, B.SCsamar alomair100% (2)
- Nutripal Cholesterol Control Plan: "Nutripal - Personal Online Diet Consultation"Document2 pagesNutripal Cholesterol Control Plan: "Nutripal - Personal Online Diet Consultation"Ashok Raj GuptaNo ratings yet
- 4-Bioavailability of Fat-Soluble Vitamins 2018Document30 pages4-Bioavailability of Fat-Soluble Vitamins 2018Juliet LópezNo ratings yet
- Exampro GCSE Biology: B2.3 EnzymesDocument33 pagesExampro GCSE Biology: B2.3 EnzymesMeera ParaNo ratings yet
- TELOSMA PROCUMBENS DraftDocument3 pagesTELOSMA PROCUMBENS DraftKaren CasaulNo ratings yet
- Kti D3 Analis Kesehatan LRDocument60 pagesKti D3 Analis Kesehatan LRMinayatul FatimahNo ratings yet
- PMLS 2 Handling and Processing of Blood Specimens For LaboratoryDocument5 pagesPMLS 2 Handling and Processing of Blood Specimens For LaboratoryXyrelle NavarroNo ratings yet
- 26430Document2 pages26430Amandeep KaurNo ratings yet
- QuestionsDocument8 pagesQuestionsshamNo ratings yet
- 08 - Allowable Error Table 2014-FinalDocument14 pages08 - Allowable Error Table 2014-FinalFe Rackle Pisco JamerNo ratings yet
- Biology Investigatory ProjectDocument16 pagesBiology Investigatory ProjectMohammed Kabir K. GNo ratings yet
- Cramsheet (Exam Cram Nclex PN)Document2 pagesCramsheet (Exam Cram Nclex PN)Katrina Reyes94% (32)
- Definition of Terms: Herbaceous Plant Costaceae Brazil Bahia Espirito SantoDocument1 pageDefinition of Terms: Herbaceous Plant Costaceae Brazil Bahia Espirito SantoAshly Jamiah DelRosario ManatoNo ratings yet
- Book Lab Tests in India - Find Diagnostic Centers Near Your Place - MedlifeDocument1 pageBook Lab Tests in India - Find Diagnostic Centers Near Your Place - Medlifegunjali daveNo ratings yet
- LIPIGET 10 MG TABLETDocument2 pagesLIPIGET 10 MG TABLETHuzaifaNo ratings yet
- 1393un 2023-03Document95 pages1393un 2023-03Mohammed TahounNo ratings yet
- Test Bank For Personal Nutrition 9th EditionDocument32 pagesTest Bank For Personal Nutrition 9th Editionthomasburgessptrsoigxdk100% (21)
- Mohammed S. Razzaque, Takashi Taguchi - Cardiovascular Disorders in Hemodialysis - 14th International Course On Hemodialysis, Vicenza, May 2005 (Contributions To Nephrology) (2005)Document377 pagesMohammed S. Razzaque, Takashi Taguchi - Cardiovascular Disorders in Hemodialysis - 14th International Course On Hemodialysis, Vicenza, May 2005 (Contributions To Nephrology) (2005)AshNo ratings yet
- Uk125 2324 001046Document10 pagesUk125 2324 001046shekharkumarkashyap8126No ratings yet
- Roche Cobas E411 Tests MenuDocument4 pagesRoche Cobas E411 Tests Menuمصطفى علي0% (1)