You might also like
- The Big Book of Infectious Disease Trivia: Everything You Ever Wanted to Know about the World's Worst Pandemics, Epidemics and DiseasesFrom EverandThe Big Book of Infectious Disease Trivia: Everything You Ever Wanted to Know about the World's Worst Pandemics, Epidemics and DiseasesNo ratings yet
- Viral Vistas: Insights into Infectious Diseases: The Invisible War: Decoding the Game of Hide and Seek with PathogensFrom EverandViral Vistas: Insights into Infectious Diseases: The Invisible War: Decoding the Game of Hide and Seek with PathogensNo ratings yet
- Human Common DiseasesDocument11 pagesHuman Common Diseasessadia khan SultaniNo ratings yet
- CH 14 EpidemiologyDocument33 pagesCH 14 EpidemiologyCangelkween Krixen BautistaNo ratings yet
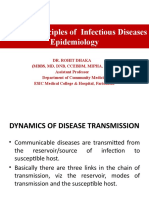
- Introduction To Infectious Diseases Lec1 2024Document30 pagesIntroduction To Infectious Diseases Lec1 2024Dictor Omar Botan kheyreNo ratings yet
- Peter John P. Gono, RN, ManDocument22 pagesPeter John P. Gono, RN, ManGardoke Jr. M. LansonNo ratings yet
- Disease Principles and EpidemiologyDocument33 pagesDisease Principles and EpidemiologyLiezel CauilanNo ratings yet
- Communicable vs Non-Communicable DiseasesDocument147 pagesCommunicable vs Non-Communicable Diseaseschristine gisembaNo ratings yet
- Systemic Infections From GiDocument10 pagesSystemic Infections From GiJake MillerNo ratings yet
- Nam chp24 PDFDocument17 pagesNam chp24 PDFJannatur RahmahNo ratings yet
- Bacterial InfectionsDocument20 pagesBacterial InfectionsFahad RasheedNo ratings yet
- 2 GIT, GUT AND STDs (INFECTIOUS DISEASES)Document30 pages2 GIT, GUT AND STDs (INFECTIOUS DISEASES)TumabangNo ratings yet
- Communicable-D FINAL 2021-1-9Document16 pagesCommunicable-D FINAL 2021-1-9Shimaa KashefNo ratings yet
- Swine Influenza: Nature of The DiseaseDocument8 pagesSwine Influenza: Nature of The Diseasejawairia_mmgNo ratings yet
- What is a communicable disease? Types and how they spreadDocument3 pagesWhat is a communicable disease? Types and how they spreadSantos JewelNo ratings yet
- CD Concept Lecture NotesDocument9 pagesCD Concept Lecture NotesJenny Rose GriñoNo ratings yet
- Preventing Healthcare-Associated InfectionsDocument16 pagesPreventing Healthcare-Associated InfectionsRDi JNo ratings yet
- Infectious Disease Causes, Transmission, and PreventionDocument15 pagesInfectious Disease Causes, Transmission, and Preventioncylon3No ratings yet
- Communicable DiseasesDocument22 pagesCommunicable DiseaseskaramnNo ratings yet
- CDC 1 IntroDocument174 pagesCDC 1 Introdemessie diriba100% (1)
- Bacterial Disease 1. Pulmonary TuberculosisDocument7 pagesBacterial Disease 1. Pulmonary TuberculosiskanishqcNo ratings yet
- CH 5 Infectious DiseaseDocument40 pagesCH 5 Infectious Diseaser55fsf75hpNo ratings yet
- Bio InvestigatoryDocument15 pagesBio InvestigatoryShrilata EruguralaNo ratings yet
- What is a communicable diseaseDocument2 pagesWhat is a communicable diseaseChristian AlejoNo ratings yet
- Infectious DiseasesDocument10 pagesInfectious DiseasesAgnes Marie RendonNo ratings yet
- Classification of Communicable DiseasesDocument40 pagesClassification of Communicable Diseasesvarshasharma0575% (8)
- Introduction To Tropical MedicineDocument5 pagesIntroduction To Tropical MedicineisaacturyabikirizaNo ratings yet
- Typhoid FeverDocument14 pagesTyphoid FeverJames Cojab SacalNo ratings yet
- CURS ENGLEZA Boli InfectioaseDocument246 pagesCURS ENGLEZA Boli InfectioaseKiran LetrangeNo ratings yet
- Topic 3 Chain of Infection, Disease Transamission, Control and PreventionDocument38 pagesTopic 3 Chain of Infection, Disease Transamission, Control and PreventionF2056 SITI AISYAH BINTI MOHAMMED NOORNo ratings yet
- 10.1 Infectious DiseasesDocument80 pages10.1 Infectious Diseasesnie20060301No ratings yet
- Microorganism Classification GuideDocument26 pagesMicroorganism Classification GuidehangoverNo ratings yet
- Presented by Riya XFDocument19 pagesPresented by Riya XFdikpalakNo ratings yet
- CHAPTER 6 Infection and DiseasesDocument17 pagesCHAPTER 6 Infection and DiseasesDanica DaniotNo ratings yet
- Chapter-8 Human Health and Diseases ContinuationDocument9 pagesChapter-8 Human Health and Diseases ContinuationKeerthana D SNo ratings yet
- Introduction To CDC Pathogens - 2019 - 2020Document48 pagesIntroduction To CDC Pathogens - 2019 - 2020McLord SelasiNo ratings yet
- Nosocomial InfectionDocument30 pagesNosocomial InfectionDivyeshkumar GanvitNo ratings yet
- Infectious or Communicable DiseasesDocument2 pagesInfectious or Communicable DiseasesДария КоваленкоNo ratings yet
- Afolabi Omowunmi IretigoDocument17 pagesAfolabi Omowunmi IretigomikealsonjuwonNo ratings yet
- Introduction To Microbiology - CHDDocument52 pagesIntroduction To Microbiology - CHDFrancis muhia KaranjaNo ratings yet
- 2020 Epidermic and Endermic DiseasesDocument5 pages2020 Epidermic and Endermic DiseasesOluwakemi OLATUNJI-ADEWUNMINo ratings yet
- PAEDS 3 - 15.10.19 PneumoniaDocument10 pagesPAEDS 3 - 15.10.19 Pneumonialotp12No ratings yet
- Introduction of MicroparasitoryDocument36 pagesIntroduction of MicroparasitoryEben Alameda-PalapuzNo ratings yet
- Diphtheria: About The DiseaseDocument18 pagesDiphtheria: About The DiseaseJesse EstradaNo ratings yet
- Primary Tuberculosis (Lecture)Document24 pagesPrimary Tuberculosis (Lecture)slyfoxkitty100% (2)
- FCH, Communicable Diseases Syllabus (2020)Document277 pagesFCH, Communicable Diseases Syllabus (2020)jean uwakijijweNo ratings yet
- Foundation in Science: Biology IiiDocument63 pagesFoundation in Science: Biology IiiLeong Sze XieNo ratings yet
- Gastrointestinal Infections CommunicatedDocument63 pagesGastrointestinal Infections CommunicatedReyadh JassemNo ratings yet
- BiologyDocument17 pagesBiologyKrish VermaNo ratings yet
- INFECTION AND INFECTIOUS PROCESS Lecture 3Document28 pagesINFECTION AND INFECTIOUS PROCESS Lecture 3Hassan Kafi AliNo ratings yet
- Chapter 7 Assignment Group 3Document40 pagesChapter 7 Assignment Group 3anas cabdisalaam NuurNo ratings yet
- Case Study For PneumoniaDocument11 pagesCase Study For PneumoniaGabbii Cinco100% (1)
- Bilogy Class 12 Practical ProjectDocument21 pagesBilogy Class 12 Practical Projectjoelpaul devrajNo ratings yet
- Principles of Infectious DiseaseDocument11 pagesPrinciples of Infectious Diseasenida intongNo ratings yet
- PowerPoint on Infectious DiseasesDocument24 pagesPowerPoint on Infectious DiseasesgabmusaNo ratings yet
- Communicable & Non-Communicable DiseaseDocument59 pagesCommunicable & Non-Communicable DiseaseMuskanNo ratings yet
- Typhoid DiseaseDocument28 pagesTyphoid DiseaseSaba Parvin Haque100% (1)
- Communicale Chaper OneDocument26 pagesCommunicale Chaper OneAyro Business CenterNo ratings yet
- Lecture 56 Public Health and Preventive Medicine Spring 2022-2023Document17 pagesLecture 56 Public Health and Preventive Medicine Spring 2022-2023stpaulafamilyNo ratings yet
- Contagious Diseases: The Science, History, and Future of Epidemics. From Ancient Plagues to Modern Pandemics, How to Stay Ahead of a Global Health CrisisFrom EverandContagious Diseases: The Science, History, and Future of Epidemics. From Ancient Plagues to Modern Pandemics, How to Stay Ahead of a Global Health CrisisNo ratings yet
- Information Systems Evolution and ModellingDocument35 pagesInformation Systems Evolution and ModellingRuchi SharmaNo ratings yet
- Rivulis Day 2Document4 pagesRivulis Day 2Ruchi SharmaNo ratings yet
- Add On IrrigationDocument5 pagesAdd On IrrigationRuchi SharmaNo ratings yet
- Village household data by month and yearDocument745 pagesVillage household data by month and yearRuchi SharmaNo ratings yet
- Final WRDDocument2 pagesFinal WRDRuchi SharmaNo ratings yet
- Agenda: We Shall Discuss The Case On DairyDocument10 pagesAgenda: We Shall Discuss The Case On DairyRuchi SharmaNo ratings yet
- Final DangsDocument2 pagesFinal DangsRuchi SharmaNo ratings yet
- Final WRDDocument2 pagesFinal WRDRuchi SharmaNo ratings yet
- Team Eco-LutionDocument2 pagesTeam Eco-LutionRuchi SharmaNo ratings yet
- Global Synfuels Case StudyDocument26 pagesGlobal Synfuels Case StudyRuchi SharmaNo ratings yet
- Information Systems Quality: Chapter-8 PRM-41Document7 pagesInformation Systems Quality: Chapter-8 PRM-41Ruchi SharmaNo ratings yet
- Case of Nestle: Chapter - 10Document7 pagesCase of Nestle: Chapter - 10Ruchi SharmaNo ratings yet
- HRM Co - PRM41Document5 pagesHRM Co - PRM41Ruchi SharmaNo ratings yet
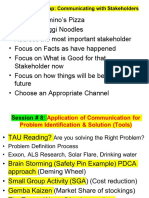
- S#8 Communication in Problem Identification & SolvingDocument8 pagesS#8 Communication in Problem Identification & SolvingRuchi SharmaNo ratings yet
- Roll No. Back Ground Background Code Grade Grade CodeDocument2 pagesRoll No. Back Ground Background Code Grade Grade CodeRuchi SharmaNo ratings yet
- Imports 2665 Income Payments 518 Net Transfers 135: Current Account $BN Exports 2105 Income Receipts 739Document3 pagesImports 2665 Income Payments 518 Net Transfers 135: Current Account $BN Exports 2105 Income Receipts 739Ruchi SharmaNo ratings yet
- Working BDocument4 pagesWorking BRuchi SharmaNo ratings yet
- Chapter 1: IntroductionDocument1 pageChapter 1: IntroductionRuchi SharmaNo ratings yet
- FoodDocument2 pagesFoodRuchi SharmaNo ratings yet
- 3Document2 pages3Ruchi SharmaNo ratings yet
- Market of Edible Oil in IndiaDocument1 pageMarket of Edible Oil in IndiaRuchi SharmaNo ratings yet
- Data For Kaps CaseDocument2 pagesData For Kaps CaseRuchi SharmaNo ratings yet
- Madhuca Indica Is A Plant of Indian Origin and Has Remarkable Pharmacological ActivityDocument1 pageMadhuca Indica Is A Plant of Indian Origin and Has Remarkable Pharmacological ActivityRuchi SharmaNo ratings yet
- Relations Among Different FactorsDocument2 pagesRelations Among Different FactorsRuchi SharmaNo ratings yet
- Molecules from Madhuca indica Interact with RA ProteinsDocument1 pageMolecules from Madhuca indica Interact with RA ProteinsRuchi SharmaNo ratings yet
- Contents:: S.NO. Page NoDocument1 pageContents:: S.NO. Page NoRuchi SharmaNo ratings yet
- Impacts of COVID-19 On Livelihoods and Coping StrategiesDocument2 pagesImpacts of COVID-19 On Livelihoods and Coping StrategiesRuchi SharmaNo ratings yet
- Madhuca Indica Was Done and Comparison Was Made With Already Reported Ligands OnDocument1 pageMadhuca Indica Was Done and Comparison Was Made With Already Reported Ligands OnRuchi SharmaNo ratings yet
- 5Document1 page5Ruchi SharmaNo ratings yet
- Madhuca Indica (Local Names: (Hindi) Mahua, Mohwa, Mauwa)Document1 pageMadhuca Indica (Local Names: (Hindi) Mahua, Mohwa, Mauwa)Ruchi SharmaNo ratings yet
- My Future Goals EssayDocument6 pagesMy Future Goals Essayfesehos0tej2100% (2)
- Protein Structure FunctionDocument57 pagesProtein Structure FunctionRaghunandan SinghNo ratings yet
- Proceedings of The National Academy of Sciences Sackler NAS Colloquium Self-Perpetuating Structural States in Biology, Disease, and GenetDocument141 pagesProceedings of The National Academy of Sciences Sackler NAS Colloquium Self-Perpetuating Structural States in Biology, Disease, and GenetAndrei CorneaNo ratings yet
- Chapter 4Document66 pagesChapter 4Monika AfableNo ratings yet
- WRL0005Document36 pagesWRL0005NewdeersciNo ratings yet
- Moreno Mallucci Et Al. (2012) Presentation Luke Daly-RonayneDocument11 pagesMoreno Mallucci Et Al. (2012) Presentation Luke Daly-RonayneLuke Daly-RonayneNo ratings yet
- 3 - Microbiology and Parasitology Main Handout Oct 2023 Ver2 Jamaiyah H. Serad - Hadji OsopDocument77 pages3 - Microbiology and Parasitology Main Handout Oct 2023 Ver2 Jamaiyah H. Serad - Hadji OsopmikzhiNo ratings yet
- Basics of Medical Microbiology & ParasitologyDocument25 pagesBasics of Medical Microbiology & ParasitologyJustine Val RevalidaNo ratings yet
- Virus General AllDocument41 pagesVirus General AllAaQib BhatNo ratings yet
- L8 VirusDocument26 pagesL8 VirusMasar Elf100% (1)
- The Protein: Presented by Dr. Shazzad Hosain Asst. Prof. EECS, NSUDocument157 pagesThe Protein: Presented by Dr. Shazzad Hosain Asst. Prof. EECS, NSUAlimushwan AdnanNo ratings yet
- TSE/BSE Risks and Regulations in PharmaceuticalsDocument28 pagesTSE/BSE Risks and Regulations in PharmaceuticalsSin PoulNo ratings yet
- Multiple Choice Questions: Q.1. Plant Virus ContainsDocument25 pagesMultiple Choice Questions: Q.1. Plant Virus ContainsS. Ramgopal RaoNo ratings yet
- Tonometer Sterilisation SurveyDocument4 pagesTonometer Sterilisation SurveyPhilip McNelsonNo ratings yet
- PRIONS THE INFECTIOUS PROTEINSDocument36 pagesPRIONS THE INFECTIOUS PROTEINSMohammed Abdul JabbarNo ratings yet
- Fundamentals of Prions and Their Inactivation (Review)Document7 pagesFundamentals of Prions and Their Inactivation (Review)ManuelNo ratings yet
- General Principles of Microbial PathogenesisDocument22 pagesGeneral Principles of Microbial PathogenesisMARTINEZ JUSTINENo ratings yet
- Comprehensive Neurology Board Review Flash CardsDocument202 pagesComprehensive Neurology Board Review Flash CardsDr. Chaim B. Colen78% (9)
- DementiaDocument40 pagesDementiacvmqx7yppdNo ratings yet
- Parkinsons Disease in Adults PDF 1837629189061Document37 pagesParkinsons Disease in Adults PDF 1837629189061Rizqan Fahlevvi AkbarNo ratings yet
- Introduction To MicrobiologyDocument24 pagesIntroduction To MicrobiologyNguyễn Ngọc NguyênNo ratings yet
- Protein Structure and Folding in 4 ChaptersDocument28 pagesProtein Structure and Folding in 4 Chapterscatalina esanuNo ratings yet
- Infectious Disease Study NotesDocument56 pagesInfectious Disease Study NotesPierre BenardNo ratings yet
- Yale University Press Spring & Summer 2013 Catalog PDFDocument164 pagesYale University Press Spring & Summer 2013 Catalog PDFYale University PressNo ratings yet
- Jim Stone Freelance 4-13-2021Document96 pagesJim Stone Freelance 4-13-2021Brian CharlesNo ratings yet
- Amino Acids, Peptides & Proteins Structures and FunctionsDocument117 pagesAmino Acids, Peptides & Proteins Structures and FunctionsdharshiiniNo ratings yet
- Protein Structure and FunctionDocument35 pagesProtein Structure and FunctionPRAJWAL SHYAM BHOSALENo ratings yet
- Std11 Bot EM 1Document236 pagesStd11 Bot EM 1Irshad Ali100% (1)
- (Advances in Virus Research 86) Said A. Ghabrial (Eds.) - Mycoviruses-Academic Press, Elsevier (2013) PDFDocument366 pages(Advances in Virus Research 86) Said A. Ghabrial (Eds.) - Mycoviruses-Academic Press, Elsevier (2013) PDFAlfredoAmadorGarcíaNo ratings yet
- Miscellaneous VirusesDocument36 pagesMiscellaneous VirusesNamdev Suryawanshi50% (2)