You might also like
- Metabolic Disease Case Study Learning ActivityDocument8 pagesMetabolic Disease Case Study Learning ActivityKhali Sciola0% (1)
- Reviewing the psychological thriller "Shutter IslandDocument4 pagesReviewing the psychological thriller "Shutter IslandDimple Castañeto CalloNo ratings yet
- Problem-based Approach to Gastroenterology and HepatologyFrom EverandProblem-based Approach to Gastroenterology and HepatologyJohn N. PlevrisNo ratings yet
- Case Study: Chapter 10 Pediatric DisordersDocument6 pagesCase Study: Chapter 10 Pediatric DisordersRica AvendañoNo ratings yet
- PCAP-C Endorsement NotesDocument2 pagesPCAP-C Endorsement NotesLorraine GambitoNo ratings yet
- Case Presentations and Patient Check-insDocument3 pagesCase Presentations and Patient Check-insJam Knows RightNo ratings yet
- The Hydrocephalus Foundation of The Philippines, Inc.: Save A Life, I PledgeDocument4 pagesThe Hydrocephalus Foundation of The Philippines, Inc.: Save A Life, I PledgejomitraNo ratings yet
- Neonatal Jaundice Case Study: Early Diagnosis and Treatment Prevents Brain DamageDocument6 pagesNeonatal Jaundice Case Study: Early Diagnosis and Treatment Prevents Brain DamagemuzamirNo ratings yet
- Covid Pathogenesis TutorialDocument29 pagesCovid Pathogenesis TutorialfelixNo ratings yet
- Covid19 - Pathophysiology and ManagementDocument51 pagesCovid19 - Pathophysiology and ManagementMyraflor CaroNo ratings yet
- Adolescents With Tuberculosis-A Review of 145 Cases, 2016Document5 pagesAdolescents With Tuberculosis-A Review of 145 Cases, 2016Yoseph Arif Putra100% (1)
- EM Practice 2018 InfluenzaDocument20 pagesEM Practice 2018 InfluenzaBarbara Yoon100% (1)
- CnsDocument15 pagesCnsArun GeorgeNo ratings yet
- Aspirin ASA BayerDocument2 pagesAspirin ASA BayerKristi WrayNo ratings yet
- HyperbilirubinemiaDocument52 pagesHyperbilirubinemiaNheljane DelacruzNo ratings yet
- Pediatric Diabetic Ketoacidosis (DKA) Algorithm (Page 1-ED) : DKA Diagnosed DKA Not DiagnosedDocument2 pagesPediatric Diabetic Ketoacidosis (DKA) Algorithm (Page 1-ED) : DKA Diagnosed DKA Not Diagnosedrolland_arrizaNo ratings yet
- Acute AbdomenDocument9 pagesAcute AbdomenHany Aboelhamd AbdelgafarNo ratings yet
- Nicu Discharge GuidelinesDocument8 pagesNicu Discharge Guidelinessophia mendiolaNo ratings yet
- Childhood Asthma Etiology and EpidemiologyDocument24 pagesChildhood Asthma Etiology and EpidemiologyEstella100% (1)
- Neonatal PneumoniaDocument2 pagesNeonatal PneumoniaJustin EduardoNo ratings yet
- Nursing Care Plans for Aspiration, Skin Integrity, and Fall RiskDocument4 pagesNursing Care Plans for Aspiration, Skin Integrity, and Fall RiskJill MurdockNo ratings yet
- Iligan City Hospital 1Document3 pagesIligan City Hospital 1danny17phNo ratings yet
- TB CPG (PPS)Document28 pagesTB CPG (PPS)Chandice CuaNo ratings yet
- Neonatal SepsisDocument39 pagesNeonatal SepsisBryan KernsNo ratings yet
- CPG Childhood ImmunizationDocument25 pagesCPG Childhood ImmunizationLady Nur StarkNo ratings yet
- Bacterial and Viral MeningitisDocument12 pagesBacterial and Viral Meningitisapi-3704562No ratings yet
- Picu Case StudyDocument3 pagesPicu Case Studyapi-455545776No ratings yet
- Case Presentation: Cagayan Valley Medical CenterDocument57 pagesCase Presentation: Cagayan Valley Medical CenterGian PagadduNo ratings yet
- Meconium Aspiration Syndrome: Walter Otieno Consultant PaediatricianDocument27 pagesMeconium Aspiration Syndrome: Walter Otieno Consultant PaediatricianMalueth AnguiNo ratings yet
- Omphalocele and GastroschisisDocument12 pagesOmphalocele and Gastroschisisluisisea100% (1)
- Abdominal Pain During PregnancyDocument58 pagesAbdominal Pain During PregnancyLuminita OpranNo ratings yet
- Mosquito Borne DiseasesDocument31 pagesMosquito Borne DiseasesRizna SaidNo ratings yet
- Pediatric Imperforate Anus - Background, Pathophysiology, EpidemiologyDocument4 pagesPediatric Imperforate Anus - Background, Pathophysiology, EpidemiologyYehuda Agus SantosoNo ratings yet
- Drug Study Pyrantel & CefuroximeDocument2 pagesDrug Study Pyrantel & CefuroximeMikhael Briones ApasNo ratings yet
- Pulmonary Atresia With Ventricular Septal Defect: Systematic ReviewDocument10 pagesPulmonary Atresia With Ventricular Septal Defect: Systematic ReviewIvan VeriswanNo ratings yet
- MeaslesDocument32 pagesMeaslesYum C100% (2)
- PPS Orals List of Topics Case StudiesDocument3 pagesPPS Orals List of Topics Case StudiesEdna M. AtanganNo ratings yet
- NICU EndorsementDocument9 pagesNICU EndorsementAileen JaymeNo ratings yet
- Pathophysiology Ischemic Stroke - VinaDocument2 pagesPathophysiology Ischemic Stroke - VinaDevi Astri KusumawardaniNo ratings yet
- 2-Sickle Cell Anemia PDFDocument21 pages2-Sickle Cell Anemia PDFJennyu YuNo ratings yet
- Surfactant Replacement Therapy: From Biological Basis To Current Clinical PracticeDocument8 pagesSurfactant Replacement Therapy: From Biological Basis To Current Clinical PracticeBetharia TriayuNo ratings yet
- Kawasaki DiseaseDocument14 pagesKawasaki DiseaseFransiskus Beat Batmomolin100% (1)
- Taking History in PaediatricsDocument7 pagesTaking History in PaediatricsNikola IgnjatovicNo ratings yet
- Integrated Management of Childhood Illness Flip ChartDocument78 pagesIntegrated Management of Childhood Illness Flip ChartkjtomananNo ratings yet
- Bronchiolitis Clinical Practice GuidelineDocument21 pagesBronchiolitis Clinical Practice GuidelineJuwita PratiwiNo ratings yet
- Pediatric Case PresentationDocument12 pagesPediatric Case PresentationMohammed jouhra100% (1)
- CPG Managment of Neonatal Jaundice (Second Edition) NewDocument62 pagesCPG Managment of Neonatal Jaundice (Second Edition) NewHafiz HamidiNo ratings yet
- Management and Investigation of Neonatal Encephalopathy: 2017 UpdateDocument13 pagesManagement and Investigation of Neonatal Encephalopathy: 2017 Updatenuge putriNo ratings yet
- Standardized Mini-Mental State Exam GuideDocument2 pagesStandardized Mini-Mental State Exam GuideSummer WrightNo ratings yet
- Acrodermatitis EnteropathicaDocument4 pagesAcrodermatitis EnteropathicaIntan FajrinNo ratings yet
- A Case Study On Septic ShockDocument51 pagesA Case Study On Septic ShockKeThSantibanNo ratings yet
- CASE STUDY PEDIA - SaavedraDocument15 pagesCASE STUDY PEDIA - SaavedraChryst Louise SaavedraNo ratings yet
- OmphalitisDocument21 pagesOmphalitisdaisukeNo ratings yet
- Fluminant Pertussis PDFDocument11 pagesFluminant Pertussis PDFDooriitha Pérez Peralta100% (1)
- Handbook Peads SurgDocument88 pagesHandbook Peads Surgsedaka26No ratings yet
- Laws Governing Medical Technology Practice in the PhilippinesDocument1 pageLaws Governing Medical Technology Practice in the PhilippinesJessie AzarragaNo ratings yet
- 191Document12 pages191asmausman1No ratings yet
- Zocor (Simvastatin)Document3 pagesZocor (Simvastatin)E100% (1)
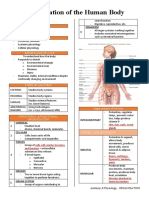
- Organization of the Human BodyDocument8 pagesOrganization of the Human BodyAly HannahNo ratings yet
- Review of Trichomonas Vaginalisinfection From (2013-2023) in Governorates of IraqDocument8 pagesReview of Trichomonas Vaginalisinfection From (2013-2023) in Governorates of IraqIJAR JOURNALNo ratings yet
- Antenatal AssessmentDocument24 pagesAntenatal AssessmentIshrat PatelNo ratings yet
- Assignment in 118 (Lecture) : C: Compressions A: Airway B: Breathing Compressions: Restore Blood FlowDocument10 pagesAssignment in 118 (Lecture) : C: Compressions A: Airway B: Breathing Compressions: Restore Blood FlowJean ReyesNo ratings yet
- Mule AaDocument37 pagesMule AaShabaka KashataNo ratings yet
- Ecc Class 68 Pediatric (Newborn) Part - 4Document44 pagesEcc Class 68 Pediatric (Newborn) Part - 4Dinabandhu BaradNo ratings yet
- The Effect of Smoking OnDocument42 pagesThe Effect of Smoking OnAndreina AcevedoNo ratings yet
- Zubiaga, R-Jeane S. - BSN 3 - For PlagscanDocument41 pagesZubiaga, R-Jeane S. - BSN 3 - For PlagscanR-Jeane ZubiagaNo ratings yet
- CASE SIMUlation 112Document6 pagesCASE SIMUlation 112Princess Levie CenizaNo ratings yet
- ZOOL 143 Topic 6 Diseases Assosiated With HIV and AIDSDocument9 pagesZOOL 143 Topic 6 Diseases Assosiated With HIV and AIDSnattydreadfathelahNo ratings yet
- Septicemia PresentationDocument23 pagesSepticemia Presentationapi-548307464No ratings yet
- Lung Volumes and CapacitiesDocument16 pagesLung Volumes and CapacitiesMoses DumbuyaNo ratings yet
- Factors Affecting Stability of OrthodontDocument7 pagesFactors Affecting Stability of OrthodontSALAHEDDINE BLIZAKNo ratings yet
- BadjokoDocument4 pagesBadjokoanderson mendesNo ratings yet
- Fistula in AnoDocument12 pagesFistula in AnoWenna Grace OdtujanNo ratings yet
- A Case Study In:: Hirschsprung DiseaseDocument18 pagesA Case Study In:: Hirschsprung DiseaseJaimie La PenaNo ratings yet
- Fall Health & Wellness (October 2022)Document20 pagesFall Health & Wellness (October 2022)Watertown Daily TimesNo ratings yet
- CHCAGE002 Implement Falls Prevention Strategies: Mode OneDocument26 pagesCHCAGE002 Implement Falls Prevention Strategies: Mode OnemaxsalNo ratings yet
- Therapeutic Monoclonal Antibodies Approved by FDA in 2019 (Mini Review)Document2 pagesTherapeutic Monoclonal Antibodies Approved by FDA in 2019 (Mini Review)asclepiuspdfsNo ratings yet
- Fiji Communicable Disease Surveillance and Outbreak Response Guidelines 2016 1Document133 pagesFiji Communicable Disease Surveillance and Outbreak Response Guidelines 2016 1roddy narayanNo ratings yet
- Chapter 14Document17 pagesChapter 14Fathimath AliNo ratings yet
- Acr-Nasci-Sir-Spr Practice Parameter For The Performance and Interpretation of Body Computed Tomography Angiography (Cta)Document15 pagesAcr-Nasci-Sir-Spr Practice Parameter For The Performance and Interpretation of Body Computed Tomography Angiography (Cta)kirim mammoNo ratings yet
- Absorb Amplify Course List (Updated Monthly)Document6 pagesAbsorb Amplify Course List (Updated Monthly)Madhu KumarNo ratings yet
- © 2017 Lanternfish ESL @Document5 pages© 2017 Lanternfish ESL @DanniNo ratings yet
- Pregnancy Induced Hypertension Case StudyDocument77 pagesPregnancy Induced Hypertension Case StudyATEHAN BORDS100% (1)
- AcetazolamideDocument4 pagesAcetazolamideAnkit RuhilNo ratings yet
- On Saying PleaseDocument2 pagesOn Saying PleaseIrfan RazaNo ratings yet
- Clinical Study of Himanshwadi Churna in The Management of Vataj Grahani W.R.T. Irritable Bowel SyndromeDocument7 pagesClinical Study of Himanshwadi Churna in The Management of Vataj Grahani W.R.T. Irritable Bowel SyndromeDrHassan Ahmed ShaikhNo ratings yet
- Liver Function TestsDocument26 pagesLiver Function TestsSadeq TalibNo ratings yet
- Clinical NeurologyDocument288 pagesClinical NeurologyWeronika Tomaszczuk-KłakNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (13)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 3.5 out of 5 stars3.5/5 (2)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (41)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 5 out of 5 stars5/5 (5)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 3.5 out of 5 stars3.5/5 (33)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- The Tennis Partner: A Doctor's Story of Friendship and LossFrom EverandThe Tennis Partner: A Doctor's Story of Friendship and LossRating: 4.5 out of 5 stars4.5/5 (4)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)