You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Blood BankDocument92 pagesBlood BankDoc PreetiNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Bacterial VaginosisDocument20 pagesBacterial VaginosisTum M. TansakulNo ratings yet
- Clinical LaboratoriesDocument24 pagesClinical Laboratoriespdamodar200788% (8)
- Equipment Devices and Procedures in The Intensive Care Unit PDFDocument16 pagesEquipment Devices and Procedures in The Intensive Care Unit PDFJena Rose ReyesNo ratings yet
- Case Pres-Banag Laum SuperfinaleDocument46 pagesCase Pres-Banag Laum SuperfinaleAyen FornollesNo ratings yet
- Vital Signs LectureDocument67 pagesVital Signs LectureJayrelle D. SafranNo ratings yet
- Trauma Ginjal: Sub Bagian Urologi Bagian/Smf Bedah FK Uns/Rsud Dr. MoewardiDocument39 pagesTrauma Ginjal: Sub Bagian Urologi Bagian/Smf Bedah FK Uns/Rsud Dr. MoewardiAtika SugiartoNo ratings yet
- Drug Study HypertensionDocument2 pagesDrug Study HypertensionFryd Ryxx GarciaNo ratings yet
- Milking Procedure Pro PDFDocument2 pagesMilking Procedure Pro PDFIznulHaq ChughtaiNo ratings yet
- Rationale Inserting NGTDocument5 pagesRationale Inserting NGTHoney VargasNo ratings yet
- Respiratory Complications of SDDocument18 pagesRespiratory Complications of SDMónica ReisNo ratings yet
- Pelvic Floor Physical Therapy and Women's Health Promotion: ReviewDocument8 pagesPelvic Floor Physical Therapy and Women's Health Promotion: ReviewMónica ReisNo ratings yet
- Effects of A Balloon-Blowing Exercise On Lung Function of SmokersDocument4 pagesEffects of A Balloon-Blowing Exercise On Lung Function of SmokersMónica ReisNo ratings yet
- Cancer, Physical Activity, and ExerciseDocument71 pagesCancer, Physical Activity, and ExerciseMónica ReisNo ratings yet
- How To Systematically Assess Serious Games Applied To Health CareDocument8 pagesHow To Systematically Assess Serious Games Applied To Health CareMónica ReisNo ratings yet
- Dementia and Parkinson's Disease: Similar and Divergent Challenges in Providing Palliative CareDocument13 pagesDementia and Parkinson's Disease: Similar and Divergent Challenges in Providing Palliative CareMónica ReisNo ratings yet
- Dementia Associated With Parkinson's Disease: ReviewDocument9 pagesDementia Associated With Parkinson's Disease: ReviewMónica ReisNo ratings yet
- Non-Motor Symptoms in Parkinsonõs Disease: W. PoeweDocument7 pagesNon-Motor Symptoms in Parkinsonõs Disease: W. PoeweMónica ReisNo ratings yet
- Multidimensional Care Burden in Parkinson-Related DementiaDocument10 pagesMultidimensional Care Burden in Parkinson-Related DementiaMónica ReisNo ratings yet
- Parkinsonism and Related Disorders: Joseph H. Friedman, MDDocument4 pagesParkinsonism and Related Disorders: Joseph H. Friedman, MDMónica ReisNo ratings yet
- Games For Health 2014: Ben Schouten Stephen Fedtke Marlies Schijven Mirjam Vosmeer Alex Gekker EditorsDocument161 pagesGames For Health 2014: Ben Schouten Stephen Fedtke Marlies Schijven Mirjam Vosmeer Alex Gekker EditorsMónica ReisNo ratings yet
- ERICDocument3 pagesERICVivienne IrvingNo ratings yet
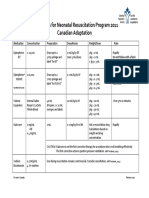
- Medications For Neonatal Resuscitation Program 2011 Canadian AdaptationDocument1 pageMedications For Neonatal Resuscitation Program 2011 Canadian AdaptationrubymayNo ratings yet
- Lithotripsy Salivary Stones OhpDocument5 pagesLithotripsy Salivary Stones Ohpaysha mksNo ratings yet
- Blood Vessels QuestionsDocument7 pagesBlood Vessels QuestionsT-Jay Ellis-DaleNo ratings yet
- Care For Client With Oxygenation Problem: OutcomesDocument19 pagesCare For Client With Oxygenation Problem: OutcomesPaul JacksonNo ratings yet
- Cisplatin As An Anti Cancer DrugDocument10 pagesCisplatin As An Anti Cancer DrugMahima KamraNo ratings yet
- Gingival Diseases in Childhood - A Review: Abst TDocument4 pagesGingival Diseases in Childhood - A Review: Abst TMagfhiro Rangga AndalasNo ratings yet
- Microneedling & Nanopore PresentationDocument58 pagesMicroneedling & Nanopore PresentationkatherineNo ratings yet
- US BTC FAQ 2015 Updated 1-5-16Document21 pagesUS BTC FAQ 2015 Updated 1-5-16Seau Vin NeeNo ratings yet
- Dexmedetomidine FAQDocument16 pagesDexmedetomidine FAQRoxana SurliuNo ratings yet
- Gavin, Nicole - Final Thesis - RedactedDocument245 pagesGavin, Nicole - Final Thesis - RedactedKarlo MedeirosNo ratings yet
- Healthy AgingDocument13 pagesHealthy AgingCarissa Mae Tapec EstradaNo ratings yet
- SGL 3 (Haematinics)Document32 pagesSGL 3 (Haematinics)raman mahmudNo ratings yet
- Virome Characterization and Identification of A Putative Parvovirus and Poxvirus in Bat Ectoparasites of Yunnan ProvinceDocument38 pagesVirome Characterization and Identification of A Putative Parvovirus and Poxvirus in Bat Ectoparasites of Yunnan ProvinceemilioNo ratings yet
- Womens Self-Management of AsthmaDocument24 pagesWomens Self-Management of AsthmaCenter for Managing Chronic DiseaseNo ratings yet
- Alcohol Withdrawal - StatPearls - NCBI BookshelfDocument7 pagesAlcohol Withdrawal - StatPearls - NCBI BookshelfDAFNE FRANÇA SANTANANo ratings yet
- BSCPT DU Syllabus-NITOR 4th BatchDocument23 pagesBSCPT DU Syllabus-NITOR 4th BatchHasan Rahman100% (2)
- Burn GuidelineDocument7 pagesBurn GuidelinegreenNo ratings yet
- Guide To Good Prescribing A Practical Manual: WHO/DAP/94.11 Distr: General Original: EnglishDocument20 pagesGuide To Good Prescribing A Practical Manual: WHO/DAP/94.11 Distr: General Original: EnglishAci LusianaNo ratings yet
- Herbalage Products KnowledgeDocument25 pagesHerbalage Products Knowledgemail9246No ratings yet