You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5811)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Handouts Renal Fabs Ucu InhouseDocument42 pagesHandouts Renal Fabs Ucu Inhousejon elleNo ratings yet
- MDCT Signs Differentiating Retroperitoneal and Intraperitoneal Lesions-Diagnostic PearlsDocument35 pagesMDCT Signs Differentiating Retroperitoneal and Intraperitoneal Lesions-Diagnostic PearlsagusNo ratings yet
- 2016 Contrast MediaDocument128 pages2016 Contrast MediabayarearadNo ratings yet
- Adult 3 FinalDocument29 pagesAdult 3 Finalأبوأحمد الحكيم100% (1)
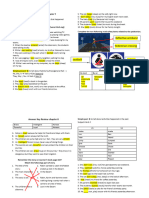
- Answer Key - Eng Worksheet Ch. 8 and 9Document2 pagesAnswer Key - Eng Worksheet Ch. 8 and 9agusNo ratings yet
- Answer Key - Eng Worksheet Ch. 8 and 9Document2 pagesAnswer Key - Eng Worksheet Ch. 8 and 9agusNo ratings yet
- 13.30 DR Arunraj Navaratnarajah - The Septic PatientDocument49 pages13.30 DR Arunraj Navaratnarajah - The Septic PatientagusNo ratings yet
- First AnnouncementDocument10 pagesFirst AnnouncementagusNo ratings yet
- A Comparative Study Between Laser Hemorrhoidoplasty Procedure and Conventional HemorrhoidectomyDocument18 pagesA Comparative Study Between Laser Hemorrhoidoplasty Procedure and Conventional HemorrhoidectomyagusNo ratings yet
- INFORMATION LETTER & SCHEDULE 4th GRADEDocument2 pagesINFORMATION LETTER & SCHEDULE 4th GRADEagusNo ratings yet
- The Significance of Neutrophil/lymphocyte Ratio As A Possible Marker of Underlying Papillary Microcarcinomas in Thyroidal Goiters: A Pilot StudyDocument6 pagesThe Significance of Neutrophil/lymphocyte Ratio As A Possible Marker of Underlying Papillary Microcarcinomas in Thyroidal Goiters: A Pilot StudyagusNo ratings yet
- Hemorrhoidal Laser Procedure - Short - and Long-Term Results From A Prospective StudyDocument5 pagesHemorrhoidal Laser Procedure - Short - and Long-Term Results From A Prospective StudyagusNo ratings yet
- 0019 2A Ful-Orr-gegeszet AngolDocument4 pages0019 2A Ful-Orr-gegeszet AngolagusNo ratings yet
- Delta Neutrophil Index and Neutrophil-to-Lymphocyte Ratio in The Differentiation of Thyroid Malignancy and Nodular GoiterDocument8 pagesDelta Neutrophil Index and Neutrophil-to-Lymphocyte Ratio in The Differentiation of Thyroid Malignancy and Nodular GoiteragusNo ratings yet
- Early Versus Delayed Dressing Removal After Primary Closure of Clean and Clean-Contaminated Surgical WoundDocument41 pagesEarly Versus Delayed Dressing Removal After Primary Closure of Clean and Clean-Contaminated Surgical WoundagusNo ratings yet
- Early Versus Delayed Post-Operative Bathing or Showering To Prevent Wound ComplicationsDocument25 pagesEarly Versus Delayed Post-Operative Bathing or Showering To Prevent Wound ComplicationsagusNo ratings yet
- Ameloblastoma 140624025211 Phpapp02Document51 pagesAmeloblastoma 140624025211 Phpapp02agusNo ratings yet
- Acute PancreatitisDocument78 pagesAcute Pancreatitisagus100% (1)
- Uettwiller 2014Document3 pagesUettwiller 2014agusNo ratings yet
- Gastric Perforation in The Neonate: Ludvig OicmianDocument6 pagesGastric Perforation in The Neonate: Ludvig OicmianagusNo ratings yet
- Neonatal Gastric Perforation : Fi) Win S. WilsonDocument3 pagesNeonatal Gastric Perforation : Fi) Win S. WilsonagusNo ratings yet
- Rasti 2007Document4 pagesRasti 2007agusNo ratings yet
- Principle of Screw and Plate Fixation & Mechanical Behavior of Implant MaterialsDocument40 pagesPrinciple of Screw and Plate Fixation & Mechanical Behavior of Implant MaterialsagusNo ratings yet
- Neonatal Gastric Perforation: A Single Center Experience: Observational StudyDocument6 pagesNeonatal Gastric Perforation: A Single Center Experience: Observational StudyagusNo ratings yet
- A Framework For Maternal and Child Health Nursing A Framework For Maternal and Child Health NursingDocument26 pagesA Framework For Maternal and Child Health Nursing A Framework For Maternal and Child Health NursingBSN CMUNo ratings yet
- Community Capstone Health Policy PaperDocument17 pagesCommunity Capstone Health Policy Paperapi-417446716No ratings yet
- World Health Organization: Jump To Navigationjump To SearchDocument2 pagesWorld Health Organization: Jump To Navigationjump To SearchJianhengMokNo ratings yet
- Contingency Plan: Implementation of Face-to-Face ClassesDocument32 pagesContingency Plan: Implementation of Face-to-Face ClassesimpromtouNo ratings yet
- 2nd Puc Biology Reasoning Questions ZoologyDocument4 pages2nd Puc Biology Reasoning Questions ZoologynomanNo ratings yet
- Hemostasis 1Document24 pagesHemostasis 1novriadi suhendraNo ratings yet
- A Rbo VirusesDocument2 pagesA Rbo VirusesDapoy PeraltaNo ratings yet
- Drug Adherence & Self-MedicationDocument3 pagesDrug Adherence & Self-MedicationFrances Lau Yee ChinNo ratings yet
- AmraDocument6 pagesAmraSangpencinta QueenNo ratings yet
- (06012023 0719) Tai Pack l3 Int Efaw and Use of An Aed Jan 2023Document15 pages(06012023 0719) Tai Pack l3 Int Efaw and Use of An Aed Jan 2023BhargaviNo ratings yet
- Anderson 2002Document14 pagesAnderson 2002JFFNo ratings yet
- Anemia During PregnancyDocument39 pagesAnemia During PregnancyBhawna JoshiNo ratings yet
- LECTURE ON Acid-Base BalanceDocument229 pagesLECTURE ON Acid-Base BalanceNayyer Khan100% (1)
- Prakriya Hospitals Investor Brochure - 2019Document19 pagesPrakriya Hospitals Investor Brochure - 2019Abhishek S AatreyaNo ratings yet
- A. Alhasso, A. Fernando - Urinary Incontinence (2012, Intech)Document334 pagesA. Alhasso, A. Fernando - Urinary Incontinence (2012, Intech)Adnan WalidNo ratings yet
- Chapter 15 - The Aging Immune System Dysregulation, Compensatory Mechanisms, and Prospects For Intervention PDFDocument25 pagesChapter 15 - The Aging Immune System Dysregulation, Compensatory Mechanisms, and Prospects For Intervention PDFCayadi Sidarta Antonius PocipNo ratings yet
- Dental Treatment Needs in Lithuanian AdplescentsDocument5 pagesDental Treatment Needs in Lithuanian AdplescentsKhairunnisa SihotangNo ratings yet
- Prosthodontic Perspective To All On - 4 ConceptDocument33 pagesProsthodontic Perspective To All On - 4 ConceptKrupali JainNo ratings yet
- Comfort Behaviors ChecklistDocument4 pagesComfort Behaviors Checklistjennylyn guadalupeNo ratings yet
- NCP RequirementsDocument3 pagesNCP RequirementsJasmine JarapNo ratings yet
- Alan Hope - 1 - Safe SedationDocument12 pagesAlan Hope - 1 - Safe SedationAlan HopeNo ratings yet
- Stem Cell BookDocument20 pagesStem Cell Bookbabasolai83No ratings yet
- Bee Therapy X - Google SearchDocument1 pageBee Therapy X - Google SearchclausakNo ratings yet
- Fifa Pcma FormDocument15 pagesFifa Pcma Formyousra AhmedNo ratings yet
- Brain Injury Medicine, 2nd Edition: Principles and Practice: August 2012Document20 pagesBrain Injury Medicine, 2nd Edition: Principles and Practice: August 2012Dipim GautamNo ratings yet
- Medical Report FormDocument7 pagesMedical Report FormShazni Afandi RusliNo ratings yet
- Dialog of Antenatal Care ExaminationDocument7 pagesDialog of Antenatal Care Examinationvina1598No ratings yet