You might also like
- Millionaire Next Door QuestionsDocument7 pagesMillionaire Next Door Questionsapi-360370073No ratings yet
- Grooming: Concept: The Evolution of and TermDocument12 pagesGrooming: Concept: The Evolution of and TermCamila PinzonNo ratings yet
- EW160 AlarmsDocument12 pagesEW160 AlarmsIgor MaricNo ratings yet
- QCM Part 145 en Rev17 310818 PDFDocument164 pagesQCM Part 145 en Rev17 310818 PDFsotiris100% (1)
- Gravity Based Foundations For Offshore Wind FarmsDocument121 pagesGravity Based Foundations For Offshore Wind FarmsBent1988No ratings yet
- Emergency and Safety ProceduresDocument22 pagesEmergency and Safety Procedurespaupastrana94% (17)
- Awais Inspector-PaintingDocument6 pagesAwais Inspector-PaintingMohammed GaniNo ratings yet
- Canopy CountersuitDocument12 pagesCanopy CountersuitJohn ArchibaldNo ratings yet
- We Move You. With Passion.: YachtDocument27 pagesWe Move You. With Passion.: YachthatelNo ratings yet
- Acute Myeloid Leukemia With Myelodysplasia RelatedDocument6 pagesAcute Myeloid Leukemia With Myelodysplasia RelatedAgus WiniNo ratings yet
- Week 7 Apple Case Study FinalDocument18 pagesWeek 7 Apple Case Study Finalgopika surendranathNo ratings yet
- EIADocument268 pagesEIACamila PinzonNo ratings yet
- LICDocument82 pagesLICTinu Burmi Anand100% (2)
- FLT3 Mutations in Acute Myeloid Leukemia: Key Concepts and Emerging ControversiesDocument20 pagesFLT3 Mutations in Acute Myeloid Leukemia: Key Concepts and Emerging Controversieseti apriyantiNo ratings yet
- FCVM 10 1090103Document9 pagesFCVM 10 1090103lipu1982No ratings yet
- 3Document10 pages3zahidNo ratings yet
- Trombocitemia EsentialaDocument22 pagesTrombocitemia EsentialalittlestressNo ratings yet
- Clinicopathological and Prognostic Significance of Programmed Death Ligand 1 Expression in Korean Melanoma PatientsDocument9 pagesClinicopathological and Prognostic Significance of Programmed Death Ligand 1 Expression in Korean Melanoma Patientsfebri susantoNo ratings yet
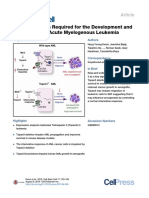
- Tetraspanin 3 Is Required For The Development and Propagation - 2015 - Cell StemDocument14 pagesTetraspanin 3 Is Required For The Development and Propagation - 2015 - Cell StemFrankenstein MelancholyNo ratings yet
- Article 5 POCDocument16 pagesArticle 5 POCmariimaria670No ratings yet
- The Role of Inflammation in Leukaemia: Janusz Krawczyk, Michael O'Dwyer, Ronan Swords, Ciara Freeman and Francis J GilesDocument26 pagesThe Role of Inflammation in Leukaemia: Janusz Krawczyk, Michael O'Dwyer, Ronan Swords, Ciara Freeman and Francis J GilesCandle Jo'inNo ratings yet
- Detection of Minimal Residual Disease in AcuteLeukemia by Flow CytometryDocument15 pagesDetection of Minimal Residual Disease in AcuteLeukemia by Flow Cytometrymilica cucuzNo ratings yet
- When To Obtain Genomic Data in Acute Myeloid Leukemia (AML) and Which Mutations MatterDocument11 pagesWhen To Obtain Genomic Data in Acute Myeloid Leukemia (AML) and Which Mutations MatterEnrique GuerreroNo ratings yet
- Aggressive T - Cell Lymphomas 2021 UpdatesDocument41 pagesAggressive T - Cell Lymphomas 2021 UpdatesAnnaNo ratings yet
- Leuemia MarkerDocument14 pagesLeuemia MarkerAdna SantanaNo ratings yet
- Update On Fundamental Mechanisms of Thyroid CancerDocument10 pagesUpdate On Fundamental Mechanisms of Thyroid Canceritang itangNo ratings yet
- Tumor Immune Microenvironment Characteristics and Their Prognostic Value in Non-Small-Cell Lung CancerDocument9 pagesTumor Immune Microenvironment Characteristics and Their Prognostic Value in Non-Small-Cell Lung CancerWilliamRayCassidyNo ratings yet
- Constitutive Transduction of Peptide Transporter and HLA Genes Restores Antigen ProcessingDocument6 pagesConstitutive Transduction of Peptide Transporter and HLA Genes Restores Antigen Processingroyhiranmay94No ratings yet
- The Clinical Impact of The Molecular Landscape of Acute Myeloid LeukemiaDocument13 pagesThe Clinical Impact of The Molecular Landscape of Acute Myeloid LeukemiaCT DAMNo ratings yet
- 2014 - MesenchymalDocument18 pages2014 - MesenchymalMiguel ÁngelNo ratings yet
- Mutaz Et Al Cancers 2022Document21 pagesMutaz Et Al Cancers 2022Farid JohanNo ratings yet
- Cancers 12 01746Document18 pagesCancers 12 01746LauraQuinteroNo ratings yet
- Cancers 12 01746 v2Document18 pagesCancers 12 01746 v2Ulicer CruzNo ratings yet
- Paper Comparativa Sobrevida de PV, TE y MFPDocument7 pagesPaper Comparativa Sobrevida de PV, TE y MFPDani HaindlNo ratings yet
- Kaito Et Al. - 2021 - CD155 and CD112 As Possible Therapeutic Targets ofDocument12 pagesKaito Et Al. - 2021 - CD155 and CD112 As Possible Therapeutic Targets ofpablopac2021No ratings yet
- Pantel EA - 2012 - Circulating Cancer Cells and DNA - V2Document20 pagesPantel EA - 2012 - Circulating Cancer Cells and DNA - V2Clark Xingzhi ZhangNo ratings yet
- ANG2 - Angiopoietin-2-Dependent Spatial Vascular Destabilization Promotes T Cell Exclusion and Limits Immunotherapy in MelanomaDocument51 pagesANG2 - Angiopoietin-2-Dependent Spatial Vascular Destabilization Promotes T Cell Exclusion and Limits Immunotherapy in MelanomaCher IshNo ratings yet
- Molecular Biomarkers in Acute Myeloid Leukemia PDFDocument45 pagesMolecular Biomarkers in Acute Myeloid Leukemia PDFHasiadin LaodeNo ratings yet
- Specific Targetin of CD163 + TAM in Tumor JEM 2019Document18 pagesSpecific Targetin of CD163 + TAM in Tumor JEM 2019Kudelko MatNo ratings yet
- European Journal of PharmacologyDocument13 pagesEuropean Journal of Pharmacologykamal.nayanNo ratings yet
- Oncogenesis of Thyroid Cancer: ReviewDocument9 pagesOncogenesis of Thyroid Cancer: ReviewRum Afida RasfaNo ratings yet
- Immune Cell Promotion of MetastasisDocument14 pagesImmune Cell Promotion of MetastasisCristian Gutiérrez VeraNo ratings yet
- Cancer Immunosurveillance: AngiogenesisDocument2 pagesCancer Immunosurveillance: AngiogenesisBrenda Bastos LevanoNo ratings yet
- Tumour Grade Significantly Correlates With Total Dysfunction of Tumour Tissue-Infiltrating Lymphocytes in Renal Cell CarcinomaDocument13 pagesTumour Grade Significantly Correlates With Total Dysfunction of Tumour Tissue-Infiltrating Lymphocytes in Renal Cell Carcinomasara.madkour99No ratings yet
- Deros A 2015Document10 pagesDeros A 2015rakaNo ratings yet
- Cancer Immunology and ImmunotherapyDocument15 pagesCancer Immunology and ImmunotherapyRamona PalalogosNo ratings yet
- Ajtr 0151665Document12 pagesAjtr 0151665Muhammad ImranNo ratings yet
- Clinics in Oncology: Flowcytometry in Acute LeukemiaDocument5 pagesClinics in Oncology: Flowcytometry in Acute LeukemiaSp PpvNo ratings yet
- Jones PA Et Al. 2019 Epigetnic Therapy in Immune-OncologyDocument11 pagesJones PA Et Al. 2019 Epigetnic Therapy in Immune-OncologyJasmyn KimNo ratings yet
- Tumor Microenvironment and Immune-Related Therapies of Head and Neck Squamous Cell CarcinomaDocument10 pagesTumor Microenvironment and Immune-Related Therapies of Head and Neck Squamous Cell CarcinomaSpore FluxNo ratings yet
- Biologia Molecular CA TiroidesDocument33 pagesBiologia Molecular CA TiroidesOskar MartinezNo ratings yet
- Li Et Al. 2022 - Untangling The Web of Intratumour HeterogeneityDocument10 pagesLi Et Al. 2022 - Untangling The Web of Intratumour HeterogeneitysodiogoesNo ratings yet
- Molecular Cell BiologyDocument36 pagesMolecular Cell BiologyEda BasarirNo ratings yet
- CX3CR1 Acts As A Protective Biomarker in The Tumor Microenvironment of Colorectal CancerDocument16 pagesCX3CR1 Acts As A Protective Biomarker in The Tumor Microenvironment of Colorectal CancerIsmaNo ratings yet
- Resolving The Paradox of Colon CancerDocument25 pagesResolving The Paradox of Colon CancerFranciscoGarciaNo ratings yet
- American J Hematol - 2022 - Patnaik - Chronic Myelomonocytic Leukemia 2022 Update On Diagnosis Risk Stratification andDocument21 pagesAmerican J Hematol - 2022 - Patnaik - Chronic Myelomonocytic Leukemia 2022 Update On Diagnosis Risk Stratification andamysweet.everNo ratings yet
- Acc 59 s1 66Document7 pagesAcc 59 s1 66luzvi1708No ratings yet
- Genetic-Guidedrisk Assessmentand Managementofthyroidcancer: Mingzhao XingDocument16 pagesGenetic-Guidedrisk Assessmentand Managementofthyroidcancer: Mingzhao XingPedro Gómez RNo ratings yet
- Anaplastic Thyroid Cancer Diagnosis and ManagementDocument16 pagesAnaplastic Thyroid Cancer Diagnosis and ManagementKimberly Andrea Gramajo OrozcoNo ratings yet
- Reviews: Neutrophil Diversity and Plasticity in Tumour Progression and TherapyDocument19 pagesReviews: Neutrophil Diversity and Plasticity in Tumour Progression and TherapySobek1789No ratings yet
- Nri 1936 ArtigoDocument13 pagesNri 1936 ArtigoGlauce L TrevisanNo ratings yet
- 24-Journal of Cancer Research and Clinical Oncology - 2020 - PaccosiDocument11 pages24-Journal of Cancer Research and Clinical Oncology - 2020 - PaccosiSara PaccosiNo ratings yet
- Colorectal Cancer Immune Infiltrates - Significance in Patient Prognosis andDocument13 pagesColorectal Cancer Immune Infiltrates - Significance in Patient Prognosis andOvamelia JulioNo ratings yet
- Characterization of Immunophenotypic Aberrancies in Adult and Childhood Acute Lymphoblastic Leukemia Lessons From Regional VariationDocument7 pagesCharacterization of Immunophenotypic Aberrancies in Adult and Childhood Acute Lymphoblastic Leukemia Lessons From Regional VariationAzucena BCNo ratings yet
- Halloran 2004Document15 pagesHalloran 2004Agustina ParnisariNo ratings yet
- Blood 1997 Jennings 2863 92Document31 pagesBlood 1997 Jennings 2863 92Neo Mervyn MonahengNo ratings yet
- 18 JL 7Document15 pages18 JL 7Irma SihotangNo ratings yet
- Boll Et Al-2023-Scientific ReportsDocument14 pagesBoll Et Al-2023-Scientific ReportsJoy IsmailNo ratings yet
- Myeloid Malignancies: Mutations, Models and Management: Review Open AccessDocument15 pagesMyeloid Malignancies: Mutations, Models and Management: Review Open AccessZikry Aulia100% (1)
- Frequent TERT Promoter Mutations in Ocular Surface Squamous NeoplasiaDocument8 pagesFrequent TERT Promoter Mutations in Ocular Surface Squamous NeoplasiaGlauce L TrevisanNo ratings yet
- A Randomized Trial Evaluating The Association Between Related Gene Polymorphism and Nausea and Vomiting Induced by Cisplatin Multi-Day ChemotherapyDocument10 pagesA Randomized Trial Evaluating The Association Between Related Gene Polymorphism and Nausea and Vomiting Induced by Cisplatin Multi-Day ChemotherapyGABRIELANo ratings yet
- Tumor Immune Microenvironment in Cancer Progression and Cancer TherapyFrom EverandTumor Immune Microenvironment in Cancer Progression and Cancer TherapyPawel KalinskiNo ratings yet
- Jmbfs 0738 KonfoDocument7 pagesJmbfs 0738 KonfoCamila PinzonNo ratings yet
- Hierarchically Defining Internet of Things Security: From CIA To CACADocument13 pagesHierarchically Defining Internet of Things Security: From CIA To CACACamila PinzonNo ratings yet
- SAGER: A Database of Symbiodiniaceae and Algal Genomic ResourceDocument8 pagesSAGER: A Database of Symbiodiniaceae and Algal Genomic ResourceCamila PinzonNo ratings yet
- Atvbaha 119 313399Document15 pagesAtvbaha 119 313399Camila PinzonNo ratings yet
- Japanese Language and Literature: Journal of The American Association of Teachers of JapaneseDocument35 pagesJapanese Language and Literature: Journal of The American Association of Teachers of JapaneseCamila PinzonNo ratings yet
- Culture VietnamDocument16 pagesCulture VietnamCamila PinzonNo ratings yet
- Value Relevance of Accounting Information in The Botswana Listed CompaniesDocument15 pagesValue Relevance of Accounting Information in The Botswana Listed CompaniesCamila PinzonNo ratings yet
- Not All Grooming Is Equal: Differential Effects of Political Vs A Liative Grooming On Cytokines and Glucocorticoids in Rhesus MacaquesDocument49 pagesNot All Grooming Is Equal: Differential Effects of Political Vs A Liative Grooming On Cytokines and Glucocorticoids in Rhesus MacaquesCamila PinzonNo ratings yet
- Incorporating Animal Movement Into Distance SamplingDocument9 pagesIncorporating Animal Movement Into Distance SamplingCamila PinzonNo ratings yet
- Silence Is Golden. Six Reasons Inhibiting The Spread of Third-Party GossipDocument11 pagesSilence Is Golden. Six Reasons Inhibiting The Spread of Third-Party GossipCamila PinzonNo ratings yet
- ReputattionDocument28 pagesReputattionCamila PinzonNo ratings yet
- GenéticaDocument179 pagesGenéticaCamila PinzonNo ratings yet
- PDF 1b - Research On Gossip - Foster PDFDocument22 pagesPDF 1b - Research On Gossip - Foster PDFCamila PinzonNo ratings yet
- Formato: Poster Apresentado em ConferênciaDocument2 pagesFormato: Poster Apresentado em ConferênciaCamila PinzonNo ratings yet
- Sexting, Intimate and Sexual Media Practices, and Social JusticeDocument18 pagesSexting, Intimate and Sexual Media Practices, and Social JusticeCamila PinzonNo ratings yet
- Question Bank For Vlsi LabDocument4 pagesQuestion Bank For Vlsi LabSav ThaNo ratings yet
- Presentation - Prof. Yuan-Shing PerngDocument92 pagesPresentation - Prof. Yuan-Shing PerngPhuongLoanNo ratings yet
- Historical DocumentsDocument82 pagesHistorical Documentsmanavjha29No ratings yet
- Application of ARIMAX ModelDocument5 pagesApplication of ARIMAX ModelAgus Setiansyah Idris ShalehNo ratings yet
- PanasonicDocument35 pagesPanasonicAsif Shaikh0% (1)
- MCS Valve: Minimizes Body Washout Problems and Provides Reliable Low-Pressure SealingDocument4 pagesMCS Valve: Minimizes Body Washout Problems and Provides Reliable Low-Pressure SealingTerry SmithNo ratings yet
- Microeconomics: Production, Cost Minimisation, Profit MaximisationDocument19 pagesMicroeconomics: Production, Cost Minimisation, Profit Maximisationhishamsauk50% (2)
- A Survey On Multicarrier Communications Prototype PDFDocument28 pagesA Survey On Multicarrier Communications Prototype PDFDrAbdallah NasserNo ratings yet
- 133 The Science and Understanding of TheDocument14 pages133 The Science and Understanding of TheCarlos RieraNo ratings yet
- Customer Satisfaction-ICICI Bank-Priyanka DhamijaDocument85 pagesCustomer Satisfaction-ICICI Bank-Priyanka DhamijaVarun GuptaNo ratings yet
- ML7999A Universal Parallel-Positioning Actuator: FeaturesDocument8 pagesML7999A Universal Parallel-Positioning Actuator: Featuresfrank torresNo ratings yet
- Chapter 3 Searching and PlanningDocument104 pagesChapter 3 Searching and PlanningTemesgenNo ratings yet
- Sign Language To Speech ConversionDocument6 pagesSign Language To Speech ConversionGokul RajaNo ratings yet
- Surface CareDocument18 pagesSurface CareChristi ThomasNo ratings yet
- 87 - Case Study On Multicomponent Distillation and Distillation Column SequencingDocument15 pages87 - Case Study On Multicomponent Distillation and Distillation Column SequencingFranklin Santiago Suclla Podesta50% (2)
- tdr100 - DeviceDocument4 pagestdr100 - DeviceSrđan PavićNo ratings yet
- Introduction To Wireless and Mobile Systems 4th Edition Agrawal Solutions ManualDocument12 pagesIntroduction To Wireless and Mobile Systems 4th Edition Agrawal Solutions Manualethelbertsangffz100% (34)
- Audit Certificate: (On Chartered Accountant Firm's Letter Head)Document3 pagesAudit Certificate: (On Chartered Accountant Firm's Letter Head)manjeet mishraNo ratings yet
- 88 - 02 Exhaust Manifold Gasket Service BulletinDocument3 pages88 - 02 Exhaust Manifold Gasket Service BulletinGerrit DekkerNo ratings yet
- Belimo Fire & Smoke Damper ActuatorsDocument16 pagesBelimo Fire & Smoke Damper ActuatorsSrikanth TagoreNo ratings yet