You might also like
- Pimp Questions-SmithDocument66 pagesPimp Questions-SmithJulie100% (2)
- Anesthesia Resident Requirements PDFDocument21 pagesAnesthesia Resident Requirements PDFJulieNo ratings yet
- Omsite 2004 PDFDocument196 pagesOmsite 2004 PDFJulieNo ratings yet
- PONV Prophylaxis Reference CardDocument1 pagePONV Prophylaxis Reference CardJulieNo ratings yet
- OMSITE QuestionsDocument6 pagesOMSITE QuestionsJulieNo ratings yet
- Cusick ReferenceDrugCardDocument2 pagesCusick ReferenceDrugCardJulieNo ratings yet
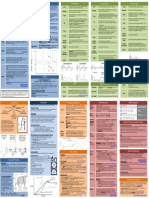
- Respiratory Therapy Pocket Reference: Ifnopt TriggerDocument2 pagesRespiratory Therapy Pocket Reference: Ifnopt TriggerJulieNo ratings yet
- 2007 Oral and Maxillofacial Surgery Self Assessment Tool (OMSSAT)Document220 pages2007 Oral and Maxillofacial Surgery Self Assessment Tool (OMSSAT)Julie100% (2)
- 2009 Oral and Maxillofacial Surgery Self Assessment Tool (OMSSAT)Document272 pages2009 Oral and Maxillofacial Surgery Self Assessment Tool (OMSSAT)Julie100% (1)
- Omfs TRST 4 PDFDocument201 pagesOmfs TRST 4 PDFgrizzlov100% (2)
- Omsite 2004 PDFDocument196 pagesOmsite 2004 PDFJulieNo ratings yet
- 2009 Oral and Maxillofacial Surgery Self Assessment Tool (OMSSAT)Document272 pages2009 Oral and Maxillofacial Surgery Self Assessment Tool (OMSSAT)Julie100% (1)
- Omsite 2005 PDFDocument180 pagesOmsite 2005 PDFJulie100% (2)
- Case Report: Hemorrhage After Dental Extractions PDFDocument9 pagesCase Report: Hemorrhage After Dental Extractions PDFJulieNo ratings yet
- Third Molar GraftingDocument8 pagesThird Molar GraftingJulieNo ratings yet
- Chlorhexidine For Prevention of Alveolar Osteitis: A Randomised Clinical TrialDocument7 pagesChlorhexidine For Prevention of Alveolar Osteitis: A Randomised Clinical TrialJulieNo ratings yet
- Parkland Trauma Soft TissueDocument14 pagesParkland Trauma Soft TissueJulieNo ratings yet
- Bedrossian Zygomatic Rescue PDFDocument33 pagesBedrossian Zygomatic Rescue PDFJulieNo ratings yet
- Parkland Trauma Upper FaceDocument14 pagesParkland Trauma Upper FaceJulieNo ratings yet
- Anticoagulants: Julene FunkDocument25 pagesAnticoagulants: Julene FunkJulieNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Arensman 2nd 9781570597510Document499 pagesArensman 2nd 9781570597510Simina SerbanNo ratings yet
- Lumbar Puncture: White SheetDocument5 pagesLumbar Puncture: White SheetcuickNo ratings yet
- Intercom March 2013Document5 pagesIntercom March 2013Lexington Medical CenterNo ratings yet
- Patient Safety, Communication and RecordkeepingDocument49 pagesPatient Safety, Communication and RecordkeepingDharlyn MungcalNo ratings yet
- Surgical Nursing Brunner 2016Document74 pagesSurgical Nursing Brunner 2016Faisol Kabir100% (1)
- Vide0 Assisted Thoracoscopic Surgery (VATS) : A Study ofDocument17 pagesVide0 Assisted Thoracoscopic Surgery (VATS) : A Study ofVibha KarmarkarNo ratings yet
- Traditional AbdominoplastyDocument23 pagesTraditional AbdominoplastyNguyen DuongNo ratings yet
- Breast Cancer - Catching Them EarlyDocument11 pagesBreast Cancer - Catching Them EarlyOgbemudia AfamNo ratings yet
- MS General Surgery Question BankDocument98 pagesMS General Surgery Question BankPrashant Singh100% (10)
- Which Activities Are The Circulating NurseDocument12 pagesWhich Activities Are The Circulating NurseDENNIS N. MUÑOZNo ratings yet
- Perioperative NursingDocument18 pagesPerioperative Nursinglagunda100% (2)
- Bariatic Surgery Guidance-2019Document22 pagesBariatic Surgery Guidance-2019ahamedsahibNo ratings yet
- ValuCare Accredited Providers v012017Document66 pagesValuCare Accredited Providers v012017aeroren40% (5)
- Intercollegiate Basic Surgical Skills (BSS) Course: Symbiosis Centre For Health Skills (SCHS)Document1 pageIntercollegiate Basic Surgical Skills (BSS) Course: Symbiosis Centre For Health Skills (SCHS)Awesoome SinceereNo ratings yet
- Final - Hospital Bill FormatDocument2 pagesFinal - Hospital Bill FormatH C50% (2)
- Benign Multinodular Goiter: A. Frilling, C. Liu, F. WeberDocument4 pagesBenign Multinodular Goiter: A. Frilling, C. Liu, F. WeberPrince AliNo ratings yet
- Managing An Outbreak of Postoperative Endophthalmitis PDFDocument12 pagesManaging An Outbreak of Postoperative Endophthalmitis PDFNawang cpsNo ratings yet
- RAMOS V CADocument4 pagesRAMOS V CARiva Rhine FernandezNo ratings yet
- Columbia Asia Referral HospitalDocument9 pagesColumbia Asia Referral HospitalNeerajNo ratings yet
- Rajiv Gandhi University of Health Sciences, KarnatakaDocument16 pagesRajiv Gandhi University of Health Sciences, KarnatakaSanthana PriyaNo ratings yet
- How Useful Is 3D Printing in Maxillofacial SurgeryDocument19 pagesHow Useful Is 3D Printing in Maxillofacial SurgeryAlex BurdeNo ratings yet
- A List of Concerns To The Mpumalanga Department of HealthDocument6 pagesA List of Concerns To The Mpumalanga Department of HealthBhekisisa HealthNo ratings yet
- New Microsoft Office Word DocumentDocument6 pagesNew Microsoft Office Word DocumentMainak MajiNo ratings yet
- Operation Theatre DisciplineDocument16 pagesOperation Theatre DisciplineDr. Ghauri100% (9)
- Milroy Lecture 2003Document28 pagesMilroy Lecture 2003Haylay GebreyohannesNo ratings yet
- Gregorio, A 54 Year Old Client Diagnosed WithDocument81 pagesGregorio, A 54 Year Old Client Diagnosed WithFreeNursingNotesNo ratings yet
- Care of The Critically Ill Surgical Patient 2010 Removed-2Document120 pagesCare of The Critically Ill Surgical Patient 2010 Removed-2lavNo ratings yet
- Bachelor in Rehabilitation Therapy CRC SyllabusDocument70 pagesBachelor in Rehabilitation Therapy CRC SyllabusHaseeb67% (3)
- MCQ Paper 2nd Class Test 2020Document11 pagesMCQ Paper 2nd Class Test 2020Super HumanNo ratings yet
- Overview of The Health System in KenyaDocument14 pagesOverview of The Health System in KenyaJohnas WanderaNo ratings yet