You might also like
- PrescriptionChart - Used in OSCEsDocument4 pagesPrescriptionChart - Used in OSCEsAmisha Vastani100% (1)
- Preop ChecklistDocument2 pagesPreop ChecklistJan Federick BantayNo ratings yet
- This Study Resource Was: Silvestri: Saunders Comprehensive Review For The NCLEX-PN Examination, 7th EditionDocument4 pagesThis Study Resource Was: Silvestri: Saunders Comprehensive Review For The NCLEX-PN Examination, 7th EditionNeoGellinNo ratings yet
- Date Progress Notes Doctor's Order C AR E DDocument4 pagesDate Progress Notes Doctor's Order C AR E DRenea Joy ArruejoNo ratings yet
- 4a JKP 2 - 7Document2 pages4a JKP 2 - 7Ala'a Emerald AguamNo ratings yet
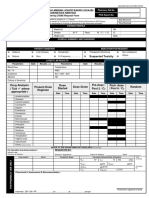
- MED-F-015 Pre - Anesthesia Record FormDocument2 pagesMED-F-015 Pre - Anesthesia Record Formdrakmalik71No ratings yet
- Pressure Injury Report For MayDocument1 pagePressure Injury Report For MayHannah LinasNo ratings yet
- Backup of DKT Anestesi OkeyDocument1 pageBackup of DKT Anestesi OkeyLinaNo ratings yet
- OR Sched 12 20Document7 pagesOR Sched 12 20Faye TuscanoNo ratings yet
- Surname AGE Hospital CODE:0000585 HOSPITAL NO.9013115 Given Name SEX Ward / Room Fmw3Document2 pagesSurname AGE Hospital CODE:0000585 HOSPITAL NO.9013115 Given Name SEX Ward / Room Fmw3Gerald AndersonNo ratings yet
- Doctor'S Order Sheet: Time Posted AND SignatureDocument3 pagesDoctor'S Order Sheet: Time Posted AND SignatureRenea Joy ArruejoNo ratings yet
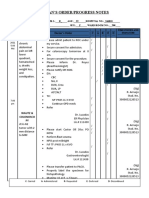
- Physician'S Order/Progress Notes: 23 S. Avila Male JhonDocument2 pagesPhysician'S Order/Progress Notes: 23 S. Avila Male JhonKrizha Angela Nicolas100% (1)
- College of Nursing: Treatment Standing Ordered MedicationDocument3 pagesCollege of Nursing: Treatment Standing Ordered MedicationPrince Rupee GonzalesNo ratings yet
- Aiims PDFDocument1 pageAiims PDFRahul RaiNo ratings yet
- Laboratory Report Sheet: Dr. Nicanor Reyes Medical Foundation Medical CenterDocument8 pagesLaboratory Report Sheet: Dr. Nicanor Reyes Medical Foundation Medical CenterJusmine Rose MundaNo ratings yet
- JP Covid ReprotDocument1 pageJP Covid ReprotYashNo ratings yet
- IVT FORM 09 S 09Document1 pageIVT FORM 09 S 09lamuraoNo ratings yet
- Bahan Bahan Dan Obat-Obatan Habis Pakai Di Kamar Operasi: RM - RI/PO/BEDAH/11Document2 pagesBahan Bahan Dan Obat-Obatan Habis Pakai Di Kamar Operasi: RM - RI/PO/BEDAH/11luh kadekNo ratings yet
- Case Sheet NGDocument10 pagesCase Sheet NGAniruddha ChatterjeeNo ratings yet
- AZ ACOG Antepartum RecordDocument6 pagesAZ ACOG Antepartum RecordAvilla Ane LukitoNo ratings yet
- Nursing NotesDocument2 pagesNursing NotesSfa ShahNo ratings yet
- TDM Monitoring Sampling Guideline Form 2022 Iso CodeDocument2 pagesTDM Monitoring Sampling Guideline Form 2022 Iso Codenur nadirahNo ratings yet
- Bahan Bahan Dan Obat-Obatan Habis Pakai Di Kamar Operasi: RM - RI/PO/RV.I/BEDAH/11Document2 pagesBahan Bahan Dan Obat-Obatan Habis Pakai Di Kamar Operasi: RM - RI/PO/RV.I/BEDAH/11Made HappyNo ratings yet
- Pathology: MicrobiologyDocument1 pagePathology: MicrobiologyAJMAL HASSANNo ratings yet
- Access To Important E-BooksDocument6 pagesAccess To Important E-Booksshashvatmarrow123No ratings yet
- College of Health Sciences: Nursing KardexDocument1 pageCollege of Health Sciences: Nursing KardexNajla Kaye PerezNo ratings yet
- Tramadol - DSDocument2 pagesTramadol - DSThrinNo ratings yet
- Health Data Profile Per Brgy.Document15 pagesHealth Data Profile Per Brgy.Jerald CruzNo ratings yet
- Case FormatDocument5 pagesCase FormatduypalaNo ratings yet
- PortfolioDocument3 pagesPortfoliobryanNo ratings yet
- Medical CertificateDocument1 pageMedical CertificateTimo EpsiNo ratings yet
- OB Requirements 2020-2021Document6 pagesOB Requirements 2020-2021KIM LORIE YAP PASCUALNo ratings yet
- PRC Form GuideDocument1 pagePRC Form GuideJohn MarkNo ratings yet
- Doctor'S Order: Case-Based ScenarioDocument8 pagesDoctor'S Order: Case-Based Scenariospain michaelisNo ratings yet
- Sample Information Form: Formular Informații ProbăDocument3 pagesSample Information Form: Formular Informații ProbăCristea InaNo ratings yet
- PRC FormDocument5 pagesPRC FormFlor Anne De JesusNo ratings yet
- Clinical Duty Forms Guide 1Document12 pagesClinical Duty Forms Guide 1Joy SaavedraNo ratings yet
- Ob Ward Dec 4-5Document18 pagesOb Ward Dec 4-5Gio PinedaNo ratings yet
- CASE 7: Cerebrovascular Accident, Bleed vs. Infarct: JMJ Marist BrothersDocument9 pagesCASE 7: Cerebrovascular Accident, Bleed vs. Infarct: JMJ Marist Brothersspain michaelisNo ratings yet
- Dysphagia HPWDocument1 pageDysphagia HPWfredericktingsyNo ratings yet
- Confidential Laboratory Report: Normal Range ResultDocument1 pageConfidential Laboratory Report: Normal Range ResultranmaltharinduNo ratings yet
- JADWAL PREOP VISITE JUMAT 22 SEPTEMBER 2023 AsaDocument3 pagesJADWAL PREOP VISITE JUMAT 22 SEPTEMBER 2023 AsaZatin ZatinNo ratings yet
- Drug Study (Ranitidine, Citicoline, Enalapril, Aspilet, Cefuroxime Etc)Document9 pagesDrug Study (Ranitidine, Citicoline, Enalapril, Aspilet, Cefuroxime Etc)gino_23_28No ratings yet
- Dispensing Report 2018 (ComPack)Document2 pagesDispensing Report 2018 (ComPack)NanRe Gacus Yan-OneNo ratings yet
- DSDSSDDocument10 pagesDSDSSDkrischaniNo ratings yet
- HIV Medication Chart - Jan 2019Document2 pagesHIV Medication Chart - Jan 2019Stephany SoutoNo ratings yet
- GS1 OCT 23 Version 2Document45 pagesGS1 OCT 23 Version 2Donzzkie DonNo ratings yet
- 02 Pre Anaesthesia Format UroDocument2 pages02 Pre Anaesthesia Format UroVHealthcare SolutionNo ratings yet
- Referensi Komite Medis PDFDocument9 pagesReferensi Komite Medis PDFreza susantoNo ratings yet
- MARIELLE CHUA - NDH KardexDocument5 pagesMARIELLE CHUA - NDH KardexMarielle ChuaNo ratings yet
- Pharmacology - Day 2 AssignmentDocument2 pagesPharmacology - Day 2 AssignmentStacey GwenNo ratings yet
- Medication OrderDocument2 pagesMedication OrderXXX YYY100% (1)
- Sampletype:Plasma: Test NameDocument2 pagesSampletype:Plasma: Test NameG.T. aquariumNo ratings yet
- Bhs Rama Non Com MasterlistDocument4 pagesBhs Rama Non Com MasterlistAnne Sherly OdevilasNo ratings yet
- Kardex: Mental Status: Activities: Diet: Tubes: Special InfoDocument3 pagesKardex: Mental Status: Activities: Diet: Tubes: Special InfoJanelle Cabida SupnadNo ratings yet
- As Required and Anticipatory Medication KardexDocument2 pagesAs Required and Anticipatory Medication KardexMichel TameleNo ratings yet
- Medication Booklet and TicketDocument3 pagesMedication Booklet and TicketCayanne ChuaNo ratings yet
- City College of San Francisco Vocational Nursing Program: Medical Surgical Care Plan Date DateDocument4 pagesCity College of San Francisco Vocational Nursing Program: Medical Surgical Care Plan Date DateShanice CapiliNo ratings yet
- Prepared By: Anne Jillian T. Singson, RN MNDocument17 pagesPrepared By: Anne Jillian T. Singson, RN MNJan Federick BantayNo ratings yet
- Care of Client With Immobilization DevicesDocument8 pagesCare of Client With Immobilization DevicesJan Federick BantayNo ratings yet
- Prepared By: Anne Jillian T. Singson, RN, MN: (Assisting Clients in The Use of Assistive Ambulatory Devices)Document22 pagesPrepared By: Anne Jillian T. Singson, RN, MN: (Assisting Clients in The Use of Assistive Ambulatory Devices)Jan Federick Bantay100% (1)
- Application of Patch, Shield, and Pressure Dressing: Eye EyeDocument10 pagesApplication of Patch, Shield, and Pressure Dressing: Eye EyeJan Federick BantayNo ratings yet
- Introduction To Logic As A Branch of Philosophy - PDFDocument18 pagesIntroduction To Logic As A Branch of Philosophy - PDFJan Federick Bantay100% (1)
- Clinical Duty FormsDocument20 pagesClinical Duty FormsJan Federick BantayNo ratings yet
- College of Nursing: Standing Ordered MedicationsDocument2 pagesCollege of Nursing: Standing Ordered MedicationsJan Federick BantayNo ratings yet
- Assisting in Application Ofcast (Plaster of Paris & Fiberglass CastDocument9 pagesAssisting in Application Ofcast (Plaster of Paris & Fiberglass CastJan Federick BantayNo ratings yet
- Administering Irrigation Eye Ear and NoseDocument11 pagesAdministering Irrigation Eye Ear and NoseJan Federick BantayNo ratings yet
- Measures in Meeting The Needs of Clients With Alteration in Visual and AuditoryDocument13 pagesMeasures in Meeting The Needs of Clients With Alteration in Visual and AuditoryJan Federick BantayNo ratings yet
- Learning Task 1: Discovering The Renaissance and William ShakespeareDocument7 pagesLearning Task 1: Discovering The Renaissance and William ShakespeareJan Federick BantayNo ratings yet
- Infusing Total Parenteral Nutrition (TPN) - 1Document16 pagesInfusing Total Parenteral Nutrition (TPN) - 1Jan Federick BantayNo ratings yet
- Nurses-Notes-BANTAY BSN3D MW WIIIDocument1 pageNurses-Notes-BANTAY BSN3D MW WIIIJan Federick BantayNo ratings yet
- Performing Colostomy Irrigation: by O-Jay Jimenez, RN, MNDocument24 pagesPerforming Colostomy Irrigation: by O-Jay Jimenez, RN, MNJan Federick Bantay100% (1)
- Administering Tube FeedingsDocument48 pagesAdministering Tube FeedingsJan Federick BantayNo ratings yet
- Assisting in Nasogastric Tube InsertionDocument11 pagesAssisting in Nasogastric Tube InsertionJan Federick BantayNo ratings yet
- BARRIER and Cannot Reach The CNSDocument4 pagesBARRIER and Cannot Reach The CNSJan Federick BantayNo ratings yet
- Book of JobDocument1 pageBook of JobJan Federick BantayNo ratings yet
- Budget PlanDocument1 pageBudget PlanJan Federick BantayNo ratings yet
- Name of Patient: Age: Sex: Ward/room: Diagnosis: Proposed Operation: Anesthesia: Anesthesiologist: SurgeonDocument2 pagesName of Patient: Age: Sex: Ward/room: Diagnosis: Proposed Operation: Anesthesia: Anesthesiologist: SurgeonJan Federick Bantay100% (3)
- V. Complications of CVDDocument26 pagesV. Complications of CVDJan Federick BantayNo ratings yet
- TPR Graphic Sheet: Tico Ronee P. 43 M M 432100 DRDocument10 pagesTPR Graphic Sheet: Tico Ronee P. 43 M M 432100 DRJan Federick BantayNo ratings yet