You might also like
- Reclaiming Your Life From A Traumatic Experience: Workbook - Rothbaum, Edna B. Foa, HembreeDocument105 pagesReclaiming Your Life From A Traumatic Experience: Workbook - Rothbaum, Edna B. Foa, Hembreedoppler_100% (8)
- Rosanna Tan-Andal vs. Mario Victor M. AndalDocument3 pagesRosanna Tan-Andal vs. Mario Victor M. AndalFrance Sanchez100% (4)
- The Fear of Attending School: DidaskaleinophobiaDocument13 pagesThe Fear of Attending School: DidaskaleinophobiaJoe MamaNo ratings yet
- Research Paper MethDocument4 pagesResearch Paper Methapi-260602713100% (1)
- Disability CertificateDocument1 pageDisability CertificateGopi PothirajNo ratings yet
- MR JonesDocument1 pageMR JonesJap-Jap Vacalares100% (1)
- Annexure 1Document1 pageAnnexure 1VIMAL MAURYANo ratings yet
- Proforma A1: Residential/Domicile CertificateDocument5 pagesProforma A1: Residential/Domicile CertificateRahul RoyNo ratings yet
- Formno.10 IaDocument1 pageFormno.10 IajsparakhNo ratings yet
- Form No 10-IaDocument1 pageForm No 10-IaMd Waseem KNo ratings yet
- Disability CertiDocument2 pagesDisability CertiHAR NazarNo ratings yet
- 800 DDBDocument1 page800 DDBguru prasathNo ratings yet
- PWD Registration Form: Part 1.0: IdentificationDocument5 pagesPWD Registration Form: Part 1.0: IdentificationmuhammedmuseneroNo ratings yet
- Format Pre EmploymentDocument10 pagesFormat Pre EmploymentNurman HidayatNo ratings yet
- FINAL CAT-III ADVT (2022) Final - 39-42Document4 pagesFINAL CAT-III ADVT (2022) Final - 39-42jackNo ratings yet
- Medical History FormDocument5 pagesMedical History FormgaloperiscolNo ratings yet
- 1 Yes Special Educ. 3 FinalDocument4 pages1 Yes Special Educ. 3 FinalLYn LYn AriarNo ratings yet
- Deformity QuestionnaireDocument2 pagesDeformity Questionnairevikash kumarNo ratings yet
- PWD CertificateDocument1 pagePWD CertificateVikas Mani TripathiNo ratings yet
- Covid19 Melnyk - OdtDocument6 pagesCovid19 Melnyk - OdtOleksandr MelnykNo ratings yet
- Proformas PUMDET-2021Document4 pagesProformas PUMDET-2021Mayank AgarwalNo ratings yet
- Proformas 4 ANM GNM 2022Document8 pagesProformas 4 ANM GNM 2022Anuj Kumar MondalNo ratings yet
- Certificate of Disability Form-VI PDFDocument3 pagesCertificate of Disability Form-VI PDFpyro_pradeepNo ratings yet
- Form G Health Examination Report International StudentDocument6 pagesForm G Health Examination Report International StudentVictor OjukwuNo ratings yet
- Disability Certificate (PWD) Form VI 2022Document2 pagesDisability Certificate (PWD) Form VI 2022blogwriter048No ratings yet
- Second Quarterly Examination in CaregivingDocument4 pagesSecond Quarterly Examination in CaregivingJasonS.FlavianoNo ratings yet
- Form 10IADocument1 pageForm 10IAkktbrr1No ratings yet
- PART1 Exceptional-Development-Physical-Disabilities-Sensory-Impairments-Learning-Disabilities-and-Attention-Deficit-Hyperactivity-DisordersDocument5 pagesPART1 Exceptional-Development-Physical-Disabilities-Sensory-Impairments-Learning-Disabilities-and-Attention-Deficit-Hyperactivity-DisorderskaiyihNo ratings yet
- Medical FormDocument1 pageMedical Formmuhammad shahrozeNo ratings yet
- Nephrologist Physical Therapist Cardiologist Dentist DermatologistDocument2 pagesNephrologist Physical Therapist Cardiologist Dentist DermatologistMyrr Dane AliligayNo ratings yet
- NSFAS Disability Annexure A - 2022Document2 pagesNSFAS Disability Annexure A - 2022courtney lemmertNo ratings yet
- Elem Sec Health CardsDocument17 pagesElem Sec Health CardsMary Grace CalipesNo ratings yet
- 41 Fad Advts090721 12 20Document9 pages41 Fad Advts090721 12 20Manova JNo ratings yet
- Language For Understanding Covid19 Conversation Topics Dialogs Reading Comprehension 125476Document8 pagesLanguage For Understanding Covid19 Conversation Topics Dialogs Reading Comprehension 125476Deti Kurnia DewiNo ratings yet
- 2nd Long Quiz Q1 Grade 6Document2 pages2nd Long Quiz Q1 Grade 6Raynalie DispoNo ratings yet
- Guidelines To Fill in Health Examination ReportDocument6 pagesGuidelines To Fill in Health Examination ReportNurman HidayatNo ratings yet
- 1503182828PWBD Certificate - FORM VI PDFDocument2 pages1503182828PWBD Certificate - FORM VI PDFMadhu PanchadarlaNo ratings yet
- MAPEH (Health) 6 - Quarter 1 - Quiz No. 1Document1 pageMAPEH (Health) 6 - Quarter 1 - Quiz No. 1KervinNo ratings yet
- Functional Capacity Screen ManualDocument22 pagesFunctional Capacity Screen ManualRachid Boujdi -Mendeley community advisor-No ratings yet
- PWD Medical Certificate & Format For ScribeDocument2 pagesPWD Medical Certificate & Format For Scribehemantaduttaghy1No ratings yet
- Types of ImpairmentsDocument3 pagesTypes of ImpairmentsshrutiNo ratings yet
- PWD ResolutionDocument60 pagesPWD ResolutionPradiptaJenaNo ratings yet
- Republic of The Philippines Department of Education Republic of The Philippines Department of EducationDocument1 pageRepublic of The Philippines Department of Education Republic of The Philippines Department of EducationElma Joyce BatuyongNo ratings yet
- Application Form RBI Bank Medical Consultant PostsDocument2 pagesApplication Form RBI Bank Medical Consultant PostsNeha SharmaNo ratings yet
- Application Form Residency & PostRes 2022Document2 pagesApplication Form Residency & PostRes 2022Franz LibreNo ratings yet
- Form 6 Local LEAVEDocument2 pagesForm 6 Local LEAVECielito Alili Cervancia-LuceroNo ratings yet
- NSFAS Disability Annexure A - 2023Document2 pagesNSFAS Disability Annexure A - 2023karabo karaboNo ratings yet
- Unit - 3 - Various Types of DisabilitiesDocument4 pagesUnit - 3 - Various Types of DisabilitiesMeghanaagarwal9No ratings yet
- Kolej Teknologi Darulnaim: Darulnaim College of TechnologyDocument5 pagesKolej Teknologi Darulnaim: Darulnaim College of TechnologyDaryanto SutejiNo ratings yet
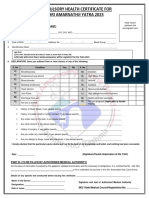
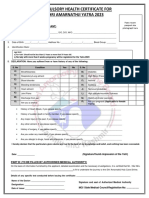
- FormatCHCYatra 2023Document1 pageFormatCHCYatra 2023Eknath KoliNo ratings yet
- CHC Updated 2023Document1 pageCHC Updated 2023maheshmonu9449No ratings yet
- CHC Updated 2023Document1 pageCHC Updated 2023Vishal Singh ShekhawatNo ratings yet
- Learners Record BookDocument11 pagesLearners Record BookMarjhun Flores GuingayanNo ratings yet
- Pediatrician Report: Questions Relating To Proposed InsuredDocument2 pagesPediatrician Report: Questions Relating To Proposed InsuredSincerely ReynNo ratings yet
- Students Medical Examination FormDocument3 pagesStudents Medical Examination FormJoril MayendeNo ratings yet
- Medical Form Malaysian 1314Document6 pagesMedical Form Malaysian 1314A’ayisha SiddiqaNo ratings yet
- Wolff y Kennedy 1994Document81 pagesWolff y Kennedy 1994Juan francisco GarastoNo ratings yet
- Proformas For Certificates Etc.Document6 pagesProformas For Certificates Etc.Sahil KhanNo ratings yet
- Chapter IIIDocument18 pagesChapter IIICelina Dela CruzNo ratings yet
- Monthly / Annual Health Services Accomplishment Report: Department of EducationDocument5 pagesMonthly / Annual Health Services Accomplishment Report: Department of EducationJean Antoniet Acopiado LegadosNo ratings yet
- TM 1 Port Compilation 1Document71 pagesTM 1 Port Compilation 1John Mike DolotNo ratings yet
- PWD Id GuideDocument3 pagesPWD Id GuideErickson MasNo ratings yet
- Notice DR Aww Bkpu CDocument8 pagesNotice DR Aww Bkpu Cduttabishal712No ratings yet
- Nursing Assessment Template 09Document3 pagesNursing Assessment Template 09jolibeecaldonaNo ratings yet
- Inside the Eye Disease Just the Facts: A Resource Manual for the Vision Rehabilitation ProfessionalsFrom EverandInside the Eye Disease Just the Facts: A Resource Manual for the Vision Rehabilitation ProfessionalsNo ratings yet
- Notice: Urgent Attention CandidatesDocument1 pageNotice: Urgent Attention CandidatesBholaNathNo ratings yet
- Affidavit ManfDocument1 pageAffidavit ManfRais IqbalNo ratings yet
- What Would You Like To Show? Let Your Data Speak: ChartDocument1 pageWhat Would You Like To Show? Let Your Data Speak: ChartManuel Andres Camposano Recalde100% (1)
- Clinical Management Protocol: Covid-19Document23 pagesClinical Management Protocol: Covid-19Gokul ChandolaNo ratings yet
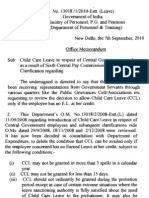
- 1 2010-Estt.-LeaveDocument3 pages1 2010-Estt.-LeavePawan SalujaNo ratings yet
- 1 2010-Estt.-LeaveDocument3 pages1 2010-Estt.-LeavePawan SalujaNo ratings yet
- Important Message From Organizing Committee IAPSMUP-UK Conference 2020Document1 pageImportant Message From Organizing Committee IAPSMUP-UK Conference 2020BholaNathNo ratings yet
- ShowPdf PDFDocument1 pageShowPdf PDFBholaNathNo ratings yet
- ShowPdf PDFDocument1 pageShowPdf PDFBholaNathNo ratings yet
- Fokkiu La ( K% 07@Ch&2020 Izksqslj Ds in GsrqaDocument16 pagesFokkiu La ( K% 07@Ch&2020 Izksqslj Ds in GsrqaBholaNathNo ratings yet
- ShowPdf PDFDocument1 pageShowPdf PDFBholaNathNo ratings yet
- Patient-Led Active Tuberculosis Case-Finding in The Democratic Republic of The CongoDocument9 pagesPatient-Led Active Tuberculosis Case-Finding in The Democratic Republic of The CongoBholaNathNo ratings yet
- AHPCON-2020 First Announcement Brochure 18th Nov 2019Document3 pagesAHPCON-2020 First Announcement Brochure 18th Nov 2019BholaNathNo ratings yet
- Number 2Document1 pageNumber 2BholaNathNo ratings yet
- Package /bibliography For LaTeXDocument21 pagesPackage /bibliography For LaTeXVicente JorgeNo ratings yet
- AHPCON-2020 First Announcement Brochure 18th Nov 2019Document3 pagesAHPCON-2020 First Announcement Brochure 18th Nov 2019BholaNathNo ratings yet
- MoM Civil Surgeon 10 Dec 2019 PDFDocument2 pagesMoM Civil Surgeon 10 Dec 2019 PDFBholaNathNo ratings yet
- Zoonoses Strategic Framework For Rabies EliminationDocument60 pagesZoonoses Strategic Framework For Rabies Eliminationhidayat0781No ratings yet
- Drugs of AbuseDocument21 pagesDrugs of AbuseEmily T. NonatoNo ratings yet
- Prova de Proficiência em Leitura - Inglês - UFPA - Modelo 1Document3 pagesProva de Proficiência em Leitura - Inglês - UFPA - Modelo 1DANIELLENo ratings yet
- PsychologicaldisorderprojectDocument4 pagesPsychologicaldisorderprojectapi-280442205No ratings yet
- Treatment of Adult Major Depressive Disorder (MDD) ToolDocument12 pagesTreatment of Adult Major Depressive Disorder (MDD) ToolSubhash SharmaNo ratings yet
- Abnormal Psychology Movie ReviewDocument3 pagesAbnormal Psychology Movie ReviewAthirah NarawiNo ratings yet
- A Review of Literature of Anxiety Amongst AdolescenceDocument3 pagesA Review of Literature of Anxiety Amongst AdolescenceViveca Isabelle NamiaNo ratings yet
- CgiDocument2 pagesCgiPutu Agus GrantikaNo ratings yet
- Insomnia Severity IndexDocument2 pagesInsomnia Severity IndexFurinsuka MoriNo ratings yet
- The Rights of Persons With Disability Act, 2016 .34Document7 pagesThe Rights of Persons With Disability Act, 2016 .34HemantNo ratings yet
- Lesson 1 - Early Intervention Strategies For Children With AutismDocument2 pagesLesson 1 - Early Intervention Strategies For Children With AutismXlian Myzter YosaNo ratings yet
- Toolkit Risk Assessment Final1Document8 pagesToolkit Risk Assessment Final1MalkOo AnjumNo ratings yet
- Frank M. Dattilio, Arthur Freeman (Auth.), Arthur Freeman, Frank M. Dattilio (Eds.) - Comprehensive Casebook of Cognitive Therapy-Springer US (1992)Document390 pagesFrank M. Dattilio, Arthur Freeman (Auth.), Arthur Freeman, Frank M. Dattilio (Eds.) - Comprehensive Casebook of Cognitive Therapy-Springer US (1992)Rey Jerly Duran BenitoNo ratings yet
- Culture and AbnormalityDocument18 pagesCulture and AbnormalityLEE YI TING -No ratings yet
- Exam 3 JeopardyDocument4 pagesExam 3 JeopardyDiya AggarwalNo ratings yet
- Comprehensive Case StudyDocument11 pagesComprehensive Case Studyapi-546503916No ratings yet
- AnxietyDocument23 pagesAnxietyJanette DickersonNo ratings yet
- NCP and Fdar: Data Goals/ Expected Outcomes Action/ Nursing Interventions Rationale Response & EvaluationDocument3 pagesNCP and Fdar: Data Goals/ Expected Outcomes Action/ Nursing Interventions Rationale Response & EvaluationKristian Karl Bautista Kiw-isNo ratings yet
- Crim211 PrelimsDocument9 pagesCrim211 PrelimsPatricia ParicoNo ratings yet
- Ege Land 2009Document5 pagesEge Land 2009RavennaNo ratings yet
- Understanding The Disease of Addiction: Kathy Bettinardi-Angres, MS, RN, APN, CADC, and Daniel H. Angres, MDDocument7 pagesUnderstanding The Disease of Addiction: Kathy Bettinardi-Angres, MS, RN, APN, CADC, and Daniel H. Angres, MDESTHER OGODONo ratings yet
- Literature Review-3Document5 pagesLiterature Review-3api-519320140No ratings yet
- Carcinosin Single RubricsDocument5 pagesCarcinosin Single RubricsAzaz QureshiNo ratings yet
- CHAPTER 16 - Schizophrenia 2Document15 pagesCHAPTER 16 - Schizophrenia 2RebeccaNo ratings yet
- Journal of Psychiatric Research: SciencedirectDocument7 pagesJournal of Psychiatric Research: SciencedirectAzisahhNo ratings yet
- Mental HealthDocument24 pagesMental HealthAnnapurna DangetiNo ratings yet