Professional Documents
Culture Documents
Stroke Seminar 2016 PDF
Stroke Seminar 2016 PDF
Uploaded by
Salomón León Beaumont-BlancoOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Stroke Seminar 2016 PDF
Stroke Seminar 2016 PDF
Uploaded by
Salomón León Beaumont-BlancoCopyright:
Available Formats
Seminar
Stroke
Graeme J Hankey
In the past decade, the definition of stroke has been revised and major advances have been made for its treatment and Published Online
prevention. For acute ischaemic stroke, the addition of endovascular thrombectomy of proximal large artery occlusion September 13, 2016
http://dx.doi.org/10.1016/
to intravenous alteplase increases functional independence for a further fifth of patients. The benefits of aspirin in S0140-6736(16)30962-X
preventing early recurrent ischaemic stroke are greater than previously recognised. Other strategies to prevent recurrent
School of Medicine &
stroke now include direct oral anticoagulants as an alternative to warfarin for atrial fibrillation, and carotid stenting as Pharmacology, The University
an alternative to endarterectomy for symptomatic carotid stenosis. For acute intracerebral haemorrhage, trials are of Western Australia, Perth,
ongoing to assess the effectiveness of acute blood pressure lowering, haemostatic therapy, minimally invasive surgery, WA, Australia
(Prof G J Hankey MD);
anti-inflammation therapy, and neuroprotection methods. Pharmacological and stem-cell therapies promise to facilitate
Department of Neurology,
brain regeneration, rehabilitation, and functional recovery. Despite declining stroke mortality rates, the global burden of Sir Charles Gairdner Hospital,
stroke is increasing. A more comprehensive approach to primary prevention of stroke is required that targets people at Perth, WA, Australia
all levels of risk and is integrated with prevention strategies for other diseases that share common risk factors. (Prof G J Hankey); and Western
Australian
Neuroscience Research
Introduction the brain, retina, or spinal cord. Stroke is distinguished Institute (WANRI), Perth, WA,
The world is facing an epidemic of stroke. Despite stable from transient ischaemic attack (TIA) if the symptoms Australia (Prof G J Hankey)
incidence rates and declining mortality rates over the past persist longer than 24 h (or lead to earlier death). An Correspondence to:
two decades, the number of incident strokes, prevalent updated definition of stroke is an acute episode of focal Prof Graeme J Hankey, School of
Medicine and Pharmacology,
stroke survivors, disability-adjusted life-years (DALYs) lost dysfunction of the brain, retina, or spinal cord lasting
The University of Western
due to stroke, and stroke-related deaths is increasing.1 This longer than 24 h, or of any duration if imaging (CT or Australia, Perkins Institute of
Seminar highlights recent developments in the definition, MRI) or autopsy show focal infarction or haemorrhage Medical Research, QEII Medical
treatment, and prevention of stroke to help clinicians to relevant to the symptoms.3 The definition includes Centre, Perth, WA 6009,
Australia
manage stroke and reduce its impact on affected subarachnoid haemorrhage.3 A TIA has been redefined
graeme.hankey@uwa.edu.au
individuals, their carers, and the population as a whole. as focal dysfunction of less than 24 h duration and with
no imaging evidence of infarction.3
Epidemiology
In 2010, an estimated 16·9 million incident strokes Diagnosis of stroke
occurred, which added to a pool of 33 million stroke Typical symptoms of stroke include sudden unilateral
survivors worldwide (table 1).1 There were 5·9 million weakness, numbness, or visual loss; diplopia; altered
deaths and 102 million DALYs lost due to stroke, making speech; ataxia; and non-orthostatic vertigo.4 Associated
stroke the second leading cause of death after ischaemic symptoms (eg, headache) vary and usually reflect the
heart disease and third leading cause of DALYs lost cause or consequences of the stroke. Atypical symptoms
worldwide. Most of the global burden of stroke, in terms of stroke include isolated vertigo, binocular blindness,
of deaths and DALYs lost, was borne by low-income and amnesia, anosognosia, dysarthria, dysphagia, stridor,
middle-income countries (LMICs) and caused by foreign accent, or headache; hemiballismus; alien hand
haemorrhagic stroke.2 syndrome; confusion; and altered consciousness.4
Between 1990 and 2010, the global incidence rate of Diagnostically, the Face Arm and Speech Test (FAST)
stroke remained stable but the number of incident first aids screening for stroke and is as sensitive and specific
strokes increased by 68%. The prevalence of stroke as the Recognition of Stroke in the Emergency Room
increased slightly, yet the number of stroke survivors (ROSIER) score.4,5 Non-contrast cranial CT scan has
increased by 84%. The number of DALYs lost per stroke near-perfect sensitivity to detect fresh intracranial
decreased, but the total number of DALYs lost increased haemorrhage, but its sensitivity for diagnosis of
by 12%. The mortality rate fell, but the number of ischaemic stroke is poor if ischaemia is recent, small, or
stroke-related deaths increased by 26% (table 1).1 The in the posterior fossa. Diffusion weighted MRI
reduction in rates can probably be attributed to improved
prevention and management of stroke, particularly in
high-income countries. The increase in numbers, despite Search strategy and selection criteria
reductions in rates, probably reflects global population I searched the Cochrane Library, PubMed, and MEDLINE using
growth, increasing life expectancy, and a change in the the search term “stroke” in combination with the terms
age structure of most populations. “diagnosis”, “risk factors”, “prognosis”, “treatment”, and
“prevention” for articles published between Jan 1, 2010, and
Definition of stroke and transient ischaemic attack June 1, 2016. I also searched the reference lists of articles
The traditional definition of stroke is clinical and based identified by the search. I selected mainly articles published in
on the sudden onset of loss of focal neurological function the past 5 years, but included older key publications.
due to infarction or haemorrhage in the relevant part of
www.thelancet.com Published online September 13, 2016 http://dx.doi.org/10.1016/S0140-6736(16)30962-X 1
Seminar
1990 2005 2010 Change from 1990–2010
Number of Rate per 100 000 Number of Rate per 100 000 Number of Rate per 100 000 Change in Change in rate in HICs Change in rate in LMICs
events person-years events person-years events person-years number of
events
All stroke
Incidence 10 078 935 251 (230–273) 14 734 124 256 (232–284) 16 894 536 258 (234–284) 68% increase 12% (6 to 17) decrease 12% (–3 to 22) increase
Prevalence 17 915 338 435 (389–497) 28 495 582 490 (437–558) 33 024 958 502 (451–572) 84% increase ·· ··
DALYs lost 86 010 384 2063 (1950–2280) 101 951 696 1750 (1569–1831) 102 232 304 1554 (1374–1642) 12% increase ·· ··
Deaths 4 660 449 117 (112–130) 5 684 970 99 (89–104) 5 874 182 88 (80–94) 26% increase 37% (31 to 41) decrease 20% (15 to 30) decrease
Ischaemic stroke
Incidence 7 238 758 181 (167–196) 10 097 297 175 (160–192) 11 569 538 176 (161–192) 37% increase 13% (6 to 18) decrease 6% (–7 to 18) increase
DALYs lost 32 128 220 796 (734–906) 38 571 908 668 (617–774) 39 389 408 598 (560–692) 18% increase 34% (16 to 36) decrease 16% (1 to 35) decrease
Deaths 2 241 077 58 (54–64) 2 701 873 47 (44–54) 2 835 419 42 (40–49) 21% increase 37% (19 to 39) decrease 14% (9 to 19) decrease
Haemorrhagic stroke
Incidence 2 840 177 69 (62–77) 4 636 828 80 (71–92) 5 324 997 82 (72–93) 47% increase 8% (1 to 15) decrease 22% (5 to 30) increase
DALYs lost 53 882 164 1267 (1068–1484) 63 379 792 1081 (935–1234) 62 842 896 956 (828–1104) 14% increase 39% (32 to 44) decrease 25% (7 to 38) decrease
Deaths 2 419 372 60 (51–70) 2 983 097 52 (45–59) 3 038 763 46 (40–53) 20% increase 38% (32 to 43) decrease 23% (–7 to 36) decrease
Data in parentheses are 95% CI. HIC=high-income country. LMIC=low-income and middle-income country. DALY=disability-adjusted life-year.
Table 1: Age-adjusted annual incidence and mortality rates, prevalence, and DALYs lost for all stroke, ischaemic stroke, and haemorrhagic stroke1,2
(DWI-MRI) detects acute brain ischaemia in about 90% Causative Classification System.12 A third of ischaemic
of patients with ischaemic stroke and about a third of strokes remain of undetermined cause (ie, cryptogenic),
patients with transient symptoms lasting less than 24 h.6,7 of which a subgroup is now defined as having embolic
DWI-MRI can be suggestive of stroke in patients with a strokes of undetermined source.13
stroke mimic (eg, seizures, migraine, hypoglycaemia, Haemorrhagic stroke is classified according to its
tumour, encephalitis, abscess, and multiple sclerosis). anatomical site or presumed aetiology. The most
Gradient-echo T2-weighted susceptibility MRI is as common sites of intracerebral haemorrhage are
sensitive as CT for acute haemorrhage and more sensitive supratentorial (85–95%), including deep (50–75%) and
for previous haemorrhage. About 20–25% of patients lobar (25–40%).14 The most common causes are
presenting with a stroke syndrome have a stroke mimic; hypertension (30–60%), cerebral amyloid angiopathy
most commonly seizures, syncope, sepsis, peripheral (10–30%), anticoagulation (1–20%), and vascular
vestibulopathy, and toxic or metabolic encephalopathy.8 structural lesions (3–8%); the cause is undetermined in
The diagnosis of stroke is most difficult in the initial about 5–20% of cases.14
hours, particularly if the onset is uncertain, the features
are atypical or changing, the patient is unwell or agitated, Risk factors
access to imaging is delayed, or brain imaging is normal. Hypertension, hypercholesterolaemia, carotid stenosis,
and atrial fibrillation are known to be causal risk factors
Subtypes of stroke for stroke because clinical trials have shown that
Clinical ischaemic stroke syndromes include total treatment of these conditions reduces the incidence of
anterior circulation syndrome, partial anterior circulation stroke.15–18 Cigarette smoking, excessive alcohol use,
syndrome, lacunar syndrome, and posterior circulation insulin resistance, and diabetes mellitus are also likely
syndrome.9 Pathological subtypes comprise ischaemic causal risk factors.19–22 Other risk factors that, if modified,
stroke (cerebral, retinal, and spinal infarction) and could reduce the incidence of stroke include
haemorrhagic stroke (intracerebral haemorrhage and environmental air pollution, childhood health
subarachnoid haemorrhage). The proportions of circumstances and fitness, high-risk diet and poor
pathological and aetiological subtypes of stroke vary nutrition, physical inactivity, obesity, blood pressure
among populations of different age, race, ethnic origin, variability, sleep-disordered breathing, chronic inflam-
and nationality. mation, chronic kidney disease, migraine, hormonal
Aetiologically, ischaemic stroke is caused by embolism contraception or hormone replacement therapy,
from the heart, artery-to-artery embolism, and in-situ psychosocial stress, depression, job strain, and long
small vessel disease. Aetiological subtypes of ischaemic working hours.23,24
stroke are classified according to the TOAST Besides rare highly penetrant mendelian mutations
classification,10 the ASCOD phenotyping system that cause early-onset stroke, several genetic loci have
(A: atherosclerosis; S: small-vessel disease; C: cardiac been associated with ischaemic stroke (eg, chromosome
pathology; O: other cause; D: dissection),11 and the 12q24.12 near ALDH2) and its subtypes—eg, the ZFHX3
2 www.thelancet.com Published online September 13, 2016 http://dx.doi.org/10.1016/S0140-6736(16)30962-X
Seminar
gene on chromosome 16q22 and PITX2 gene on
Score for
chromosome 4q25 for cardioembolic stroke; the HDAC9 characteristic
gene on chromosome 7p21 and locus on chromosome
ABCD³-I score32*
1p13.2 near the TSPAN2 gene for large-vessel stroke; and
Age ≥60 years 1
chromosome 6p25 near the FOXF2 gene for small-vessel
Blood pressure ≥140/90 mm Hg 1
disease.25,26 Genetic variants ε2 and ε4 within the
Clinical features
apolipoprotein E (APOE) gene are risk factors for lobar
Speech impairment without weakness 1
intracerebral haemorrhage.
Unilateral weakness 2
Ten treatable risk factors account for about 90% of the
Duration
population-attributable risk of stroke.23,24 Stroke can also be
triggered by several activities (eg, neck trauma and coitus) 10–59 min 1
and risk factors (eg, alcohol, amphetamines, infection, and ≥60 min 2
air pollution, and perhaps psychosocial stress).27 Diabetes mellitus present 1
Dual TIA (index TIA plus ≥1 other TIA in preceding 7 days) 2
Prognosis after stroke and TIA Imaging: ipsilateral ≥50% stenosis of internal carotid 2
artery
The case fatality rates after all stroke are about 15% at
Imaging: acute diffusion-weighted imaging 2
1 month, 25% at 1 year, and 50% at 5 years.28 After hyperintensity
intracerebral haemorrhage, the case fatality rates are Recurrence risk estimator at 90 days33 †‡
about 55% at 1 year and 70% at 5 years.29 About 40% of
Clinical
stroke survivors are disabled (modified Rankin Scale
History of TIA or stroke within the preceding month of 1
[mRS] score 3–5) between 1 month and 5 years after index stroke
stroke; 20% are disabled before the stroke.28 Five variables CCS aetiological stroke subtype
(age, verbal component of the Glasgow Coma Scale, arm Large artery atherosclerosis 1
power, ability to walk, and pre-stroke dependency) predict Cardioaortic embolism 0
independent survival at 3 months and 12 months after Small artery occlusion 0
stroke.30 Other prognostic factors include stroke severity, Other causes 1
clinical subtype, employment status, marital status, and Undetermined causes 0
recurrent stroke.28 Brain MRI within first 72 h
After ischaemic stroke and TIA, the risk of recurrent
Multiple acute infarcts 1
stroke without treatment is about 10% at 1 week, 15%
Simultaneous infarcts in different circulations 1
at 1 month, and 18% at 3 months.31 The risk is greater
Multiple infarcts of different ages 1
among individuals with recent symptomatic athero-
Isolated cortical infarcts 1
sclerosis and high ABCD³-I and recurrence risk estimator
scores (table 2);32,33 the ABCD² score does not reliably If the stated criteria are not met, a score of 0 is assigned. NA=not applicable.
discriminate patients at low and high risk.34 With urgent TIA=transient ischaemic attack. CCS=Causative Classification System for Ischemic
Stroke. *Total range 0–13. †Total range 0–6. ‡Available at: http://www.nmr.mgh.
assessment and appropriate treatment, the risk of harvard.edu/RRE-90.
recurrent stroke is 80% lower.35,36
The longer-term risk of recurrent stroke is about 10% Table 2: Scores to identify patients at early risk of recurrent stroke32,33
at 1 year, 25% at 5 years, and 40% at 10 years.37 The risk
is higher among individuals with symptomatic Specific treatment for acute ischaemic stroke
atherosclerotic disease, vascular risk factors, or an active Intravenous alteplase (rtPA), 0·9 mg/kg, administered
source of thrombosis, or who have discontinued within 4·5 h of ischaemic stroke, increases the odds of
antiplatelet and antihypertensive drugs. For patients no significant disability (mRS 0–1) at 3–6 months by
with atrial fibrillation, the risk of stroke increases with about a third and does not affect mortality, despite
higher CHADS2, CHA2DS2-VASc, and ABC (age, increasing the odds of symptomatic intracerebral
biomarkers [N-terminal fragment B-type natriuretic haemorrhage (table 3).40 The proportional benefits of
peptide (NT-proBNP) and cardiac troponin high- alteplase are larger with earlier treatment and the
sensitivity (cTn-hs)], and clinical history [prior stroke or proportional risks of symptomatic intracerebral
TIA]) stroke scores.38 After haemorrhagic stroke, the haemorrhage with alteplase are larger with a high
annual risks of recurrent intracerebral haemorrhage SEDAN score (blood sugar, early infarct signs, [hyper]
and ischaemic stroke are similar, and vary from 1·3% to dense cerebral artery sign, age, and National Institutes of
7·4%.29 The risk of recurrent intracerebral haemorrhage Health Stroke Scale [NIHSS] score). 40,49
is higher after lobar intracerebral haemorrhage than Using a lower dose of alteplase (0·6 mg/kg) reduces the
after non-lobar haemorrhage and in patients with incidence of symptomatic intracerebral haemorrhage but
inadequate blood pressure control than in those in does not lead to better functional outcome at 90 days
whom blood pressure is maintained within prespecified compared with standard-dose alteplase.50 Functional
limits.39 outcome is also not improved by adjunctive transcranial
www.thelancet.com Published online September 13, 2016 http://dx.doi.org/10.1016/S0140-6736(16)30962-X 3
Seminar
alteplase within 6 h of ischaemic stroke doubles the rate
Proportion of patients Odds ratio Absolute
with reported functional (95% CI) difference of angiographic revascularisation at 24 h and functional
outcome (%) independence at 90 days (table 3), and increases the
Treatment Control likelihood of improving by 1 point or more on the mRS
group (%) group (%) by 2·5 times, without increasing risk of symptomatic
Ischaemic stroke intracerebral haemorrhage or all-cause mortality.41,42 The
Thrombolysis with alteplase40 effect is consistent among elderly people (>80 years) and
Good recovery (mRS 0–1) in patients 34% 28% 1·37 (1·20–1·56) 7%
patients ineligible for intravenous alteplase.
who received alteplase 0–4·5 h after Improved outcomes with endovascular thrombectomy
stroke in recent trials can be attributed to improved patient
Good recovery (mRS 0–1) in patients 33% 23% 1·75 (1·35–2·27) 10% selection by CT or MR angiogram to confirm large artery
who received alteplase 0–3 h after occlusion (figure), shorter time to revascularisation, and
stroke
second-generation devices and techniques that enable
Good recovery (mRS 0–1) in patients 35% 30% 1·26 (1·05–1·51) 6%
who received alteplase 3–4·5 h after higher rates of reperfusion.41,42,56 Ongoing trials are
stroke evaluating whether patients with small ischaemic cores
Symptomatic ICH within 7 days 7% 1% 5·55 (4·01–7·70) 5% and substantial salvageable penumbra, as identified by
Fatal ICH within 7 days 3% <1% 7·14 (3·98–12·79) 2% CT or MR perfusion, could benefit from alteplase and
Endovascular thrombectomy41,42 endovascular thrombectomy beyond 6 h (appendix).56
Second-generation devices42 Implementation of endovascular therapy in clinical
Good recovery (mRS 0–1) 27% 13% 2·49 (1·84–3·35) 14% practice will require local algorithms to enable emergency
Independent (mRS 0–2) 46% 26% 2·35 (1·85–2·98) 20% medical services to rapidly and accurately identify, triage,
All devices41 and transport the 10% of stroke patients suitable for
endovascular therapy directly to comprehensive stroke
Independent (mRS 0–2) 43% 32% 1·71 (1·18–2·49) 11%
centres where resourced, accessible, and specialised stroke
Aspirin43
teams can restore reperfusion within 90 min of arrival.57
Independent (mRS 0–2) 55% 54% 1·05 (1·01–1·10) 1%
Death or dependence (mRS 3–6) 45% 46% 0·95 (0·91–0·99) 1%
Specific treatment for acute haemorrhagic
Hemicraniectomy44
stroke
Death (mRS 6) 30% 71% 0·19 (0·12–0·30) 41%
Intensive blood pressure reduction within 3–6 h of onset
Severe disability or death (mRS 5–6) 42% 84% 0·15 (0·09–0·24) 42%
of intracerebral haemorrhage to a systolic target of lower
Major disability or death (mRS 4–6) 73% 87% 0·42 (0·24–0·76) 14%
than 140 mm Hg may not be safe for all patients, nor more
Major or severe disability (mRS 4–5) 62% 55% 1·71 (0·78–3·74) NS; p=0·18
effective in reducing death and disability, compared to a
Intracerebral haemorrhage
systolic target of lower than 180 mm Hg (table 3).45,46
Intensive BP-lowering to target systolic
For intracerebral haemorrhage not associated with
BP <140 mm Hg (vs target
<180 mm Hg)45,46 antithrombotic therapy, recombinant activated factor
Death or dependence (mRS 3–6)45 52% 56% 0·87 (0·76–1·01) NS; p=0·06 VII (rFVIIa) decreases haematoma growth, but increases
Major disability or death (mRS 4–6)46 39% 38% 1·04 (0·85–1·27)* NS; p=0·72 thromboembolic events, and does not improve functional
Surgery for supratentorial ICH47 outcome.58 Platelet transfusion after intracerebral
Unfavourable outcome 59% 66% 0·74 (0·64–0·86) 7%
haemorrhage associated with antiplatelet drugs increases
Surgery for lobar haematoma without intraventricular haemorrhage47
death and dependence at 3 months.59 For spontaneous
Death or disability 62% 68% 0·78 (0·59–1·02) NS; p=0·07
intracerebral haemorrhage associated with vitamin K
All stroke
antagonist anticoagulation, reversal of the INR to lower
than 1·3 and reduction of the systolic blood pressure to
Stroke-unit care
lower than 160 mm Hg within 4 h is associated with
Death or dependence (mRS 3–6)48 56% 61% 0·79 (0·68–0·90) 5%
reduced hematoma enlargement.60 Four-factor
Endovascular thrombectomy given plus thrombolysis and usual care in most participants. mRS=modified Rankin Scale prothrombin complex concentrate seems superior to fresh
score. ICH=intracerebral haemorrhage. NS=not significant. BP=blood pressure. *Risk ratio (95% CI). frozen plasma to normalise the INR and reduce
Table 3: Effect of treatments or care strategies for ischaemic stroke, intracerebral haemorrhage, or all haematoma expansion.61 Management of acute
stroke on functional outcome intracerebral haemorrhage associated with direct
inhibition of thrombin or factor Xa by direct oral
doppler ultrasound,51 hypothermia,52 or desmoteplase.53 anticoagulants requires immediate cessation of the direct
Tenecteplase is being compared with alteplase in several oral anticoagulants, supportive measures, and
See Online for appendix phase 3 trials (appendix).54 Concomitant antithrombotic consideration of specific reversal agents, such as
drugs should be avoided for the first 24 h after alteplase to idarucizumab for dabigatran-associated intracerebral
limit haemorrhagic transformation of any infarcted brain.55 haemorrhage, or non-specific haemostatic agents, such as
The addition of endovascular thrombectomy with prothrombin complex concentrate, that show positive
second-generation devices (eg, stent retrievers) to laboratory results.61–65
4 www.thelancet.com Published online September 13, 2016 http://dx.doi.org/10.1016/S0140-6736(16)30962-X
Seminar
A B C D E
F G H I J
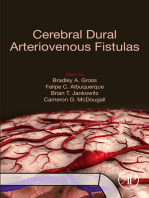
Figure: Imaging in a patient with acute ischaemic stroke treated with endovascular thrombectomy
Plain CT brain scan, axial plane, showing hyperdensity of the intracranial proximal left middle cerebral artery (A). CT angiogram, axial plane, showing a filling defect due to occlusion of the intracranial
proximal left middle cerebral artery (B). CT perfusion, axial plane, showing prolonged time to peak (TTP) cerebral blood flow in most of the territory of supply of the left middle cerebral artery (blue
area; C). CT perfusion, axial plane, showing prolonged mean transit time (MTT) of cerebral blood flow in most of the territory of supply of the left middle cerebral artery (blue area; D). CT perfusion,
axial plane, showing reduced cerebral blood flow (CBF) in most of the territory of supply of the left middle cerebral artery (blue area; E). CT perfusion, axial plane, showing preserved cerebral blood
volume (CBV) in most of the territory of supply of the left middle cerebral artery (F). CT perfusion, axial plane, showing a mismatch between the smaller infarct core in the left putamen and anterior
temporal lobe (red; increased MTT and reduced CBV) and large ischaemic penumbra (green; increased MTT and normal CBV; G). Intra-arterial digital subtraction angiogram, coronal plane, showing a
filling defect, due to occlusion, in the intracranial proximal left middle cerebral artery (H). Intra-arterial digital subtraction angiogram, coronal plane, after endovascular thrombectomy showing
restoration of cerebral blood flow in the left middle cerebral artery territory (I). Plain CT, axial plane, day 1 post-endovascular thrombectomy, showing residual infarction (low density) in the left
putamen and anterior temporal lobe (J).
Early open-surgery evacuation of supratentorial admission, nutrition screening and formal swallow
haematomas might be beneficial for patients with a assessment within 72 h, and antiplatelet therapy and
Glasgow Coma Scale score of 9–12 who are treated within adequate fluids and nutrition in the first 72 h.69 It is
8 h of symptom onset.47,66 Minimally invasive drainage by uncertain whether stroke-unit care is relevant and
catheter holds promise in the treatment of deep applicable to LMIC settings and which components are
haematomas.67 An external ventricular drain combined important in low-technology units.70
with topical fibrinolysis reduces mortality but not There is no reliable evidence to guide the optimum
functional dependence in intraventricular haemorrhage volume, duration, or mode of parenteral fluid delivery for
and hydrocephalus.68 Surgical evacuation of infratentorial patients with poor oral fluid intake. Hypertonic fluids
intracerebral haemorrhage is usually indicated if the (colloids) increase pulmonary oedema compared with
Glasgow Coma Scale score is lower than 14, haematoma isotonic fluids (crystalloids).71 For patients with dysphagia,
diameter higher than 30–40 mm, haematoma volume the effect of various swallowing therapies, feeding, and
higher than 7 cm³, or if there is obliteration of the fourth nutritional and fluid supplementation on functional
ventricle. An external ventricular drain is usually inserted outcome is uncertain.72 Nutritional supplementation is
if there is associated hydrocephalus. associated with reduced pressure sores.72
Many neuroprotective drugs have failed to show a
General treatment of acute stroke functional benefit in the treatment of acute stroke,
In high-income countries, stroke-unit care increases the including recent trials of citicoline, high-dose albumin,
likelihood of discharge home and reduces death and and magnesium sulfate.73 Current evidence does not
dependence compared with care in a general ward support routine use of physical or pharmacological
(table 3).48 Processes associated with reduced mortality strategies to reduce temperature in acute stroke; trials
include review by a stroke consultant within 24 h of are ongoing (appendix).
www.thelancet.com Published online September 13, 2016 http://dx.doi.org/10.1016/S0140-6736(16)30962-X 5
Seminar
Lowering blood pressure during the first days after not superior to aspirin in reducing the 90 day rate of
major stroke does not improve functional outcome.74,75 stroke, myocardial infarction, or death.82
There is no urgency to restart pre-existing anti- Dual antiplatelet therapy seems more effective than
hypertensive therapy in the first days, unless for monotherapy in reducing early recurrent stroke
comordid disorders.75 However, lowering of blood (table 4).83 The most effective combination is aspirin and
pressure days to weeks after TIA or minor stroke is safe clopidogrel in Chinese patients with acute TIA or minor
and associated with a low risk of recurrent stroke.35 ischaemic stroke (NIHSS score <3), who are at low risk
Lowering blood glucose to 4·0–7·5 mmol/L in the first of haemorrhagic complications and who are not carriers
24 h after ischaemic stroke by intravenous insulin does of CYP2C19 loss-of-function alleles (*2, *3).99 Trials of
not improve death or dependence but increases dual and triple acute antiplatelet therapy in other
symptomatic hypoglycaemia, particularly if glucose populations are ongoing (appendix).
concentrations are maintained within a tight range.76 Effective long-term antiplatelet regimens for preventing
recurrent stroke include aspirin 75–150 mg a day,
Preventing and managing complications clopidogrel 75 mg a day, aspirin 25 mg twice a day plus
Neurological and medical complications after stroke are extended-release dipyridamole 200 mg twice a day, and
a major cause of morbidity and mortality if they are not cilostazol (table 4).88–92 Long-term triflusal, terutroban,
anticipated, prevented, and managed appropriately. vitamin K antagonists, aspirin plus clopidogrel, and
Preventive antibiotics for 4–7 days in patients with acute vorapaxar plus standard antiplatelet treatment are not as
stroke or associated dysphagia do not reduce post-stroke safe and effective as aspirin or clopidogrel monotherapy
pneumonia or improve functional outcome.77,78 For or aspirin plus extended-release dipyridamole.100
immobile patients, intermittent pneumatic compression Anticoagulation in acute ischaemic stroke does not
with thigh-length sleeves worn on both legs for 30 days reduce early recurrent stroke, mortality, or death or
and nights reduces proximal and symptomatic deep-vein dependency compared with control, even among patients
thrombosis and improves 6 month survival, but does not at higher risk of thrombosis or lower risk of
improve functional outcome.79 Graduated compression haemorrhage.101,102 Anticoagulation is also not more
stockings are ineffective. The benefits of low-dose effective than antiplatelet therapy in reducing 90 day
subcutaneous heparins and heparinoids in reducing stroke or death after recent symptomatic carotid and
venous thromboembolism are offset by haemorrhagic vertebral artery dissection.103
complications.80 Carotid endarterectomy in patients with recent
Cerebral oedema can be a secondary consequence of a symptomatic extracranial atherosclerotic carotid stenosis
large area of brain infarction. Early decompressive reduced the risk of stroke or death at 5 years by half in
hemicraniectomy for malignant middle cerebral artery patients with 70–99% stenosis, and a quarter with 50–69%
infarction significantly decreases 12 month mortality, stenosis, when added to medical therapy 25 years ago
death or severe disability (mRS score >4), and death or (table 4).84,104 The second ECST-2 trial is currently comparing
major disability (mRS score >3), but is associated with the risks and benefits of adding immediate carotid surgery
non-significantly higher major disability (mRS (or stenting) to modern medical therapy (appendix).
score 4–5) among survivors compared with conservative Compared with carotid endarterectomy, carotid artery
treatment (table 3).44 The trade-off between improved stenting has lower risks of periprocedural myocardial
survival at the expense of substantial disability is infarction, cranial nerve palsy, and access-site
greater for patients older than 60 years than for those of haematoma, but, in patients aged 70 years or older, a
a younger age.44 The optimum criteria for patient higher risk of periprocedural stroke or death.85 The
selection, timing of surgery, and acceptable degree of long-term rate of stroke or death is also higher with
disability in survivors remain undefined. However, if carotid artery stenting than carotid endarterectomy due
decompressive hemicraniectomy is to be undertaken, it to the periprocedural differences in risk; the long-term
should be before there is major midline shift causing rates of fatal or disabling stroke, composite of major
secondary ischaemic brain injury and bleeding in vascular events, and functional outcome after carotid
the brainstem. artery stenting and carotid endarterectomy are similar
(table 4).85–87 If carotid revascularisation is to be done, it
Preventing recurrent ischaemic stroke of arterial should be early, within the first week after stroke or TIA,
origin when the risk of recurrent stroke is highest.36,104,105
Urgent initiation of effective secondary prevention after However, the operative risks may be higher if surgery is
TIA and minor ischaemic stroke can reduce the risk of done less than 48 h after symptom onset.105
early recurrent stroke by 80% (table 4).35 Immediate Stenting of recently symptomatic atherosclerotic
aspirin, 160–300 mg a day, reduces the rate and severity intracranial stenosis and extracranial vertebral stenosis is
of early recurrent stroke by at least half within the first associated with unacceptable periprocedural risks of
6–12 weeks (table 4).43,81 Ticagrelor is as safe as aspirin in stroke or death, compared with intensive medical
patients with acute TIA and mild ischaemic stroke, but is therapy.106–108 There is also no benefit of flow-augmentation
6 www.thelancet.com Published online September 13, 2016 http://dx.doi.org/10.1016/S0140-6736(16)30962-X
Seminar
Proportion of patients with outcome Risk ratio (95% CI) Absolute risk
reduction (%)
Treatment group (%) Control (%)
Acute therapy in patients with TIA or ischaemic stroke
Acute specialty unit (vs outpatient clinic)35
Stroke at 90 days 2% 10% 0·20 (0·08–0·49) 12%
Aspirin (vs control)43,81
Stroke at 6 weeks 1% 2% 0·45 (0·35–0·58) 1·3%
Stroke at 12 weeks 2% 4% 0·49 (0·40–0·60)* 1·8%
Disabling or fatal ischaemic stroke at 12 weeks 1% 2% 0·34 (0·25–0·46)* 1·4%
Ticagrelor (vs aspirin)82
Stroke at 90 days 6% 7% 0·86 (0·75–0·99)* 0·9%
Dual antiplatelet therapy (vs single drug)83
Stroke at about 90 days 6% 9% 0·69 (0·60–0·80) 2·8%
Carotid endarterectomy (vs medical therapy)84
Any stroke or operative death at 5 years in patients with 70–99% carotid stenosis 15% 29% 0·53 (0·42–0·67) 13·9%
Any stroke or operative death at 5 years in patients with 50–69% carotid stenosis 17% 23% 0·77 (0·63–0·94) 5·6%
Ipsilateral ischaemic stroke and any operative stroke or death at 5 years in patients with 70–99% carotid stenosis 10% 24% 0·40 (0·30–0·54) 14·2%
Ipsilateral ischaemic stroke and any operative stroke or death at 5 years in patients with 50–69% carotid stenosis 12% 15% 0·82 (0·64–1·05) NS; p=0·11
Carotid stent (vs carotid endarterectomy)85–87
Any stroke or death85 25% 21% 1·41 (1·07–1·84) 4·3%
Any stroke at 5 years86 15% 9% 1·71 (1·28–2·30)* 5·8%
Fatal or disabling stroke at 5 years86 6% 6% 1·06 (0·72–1·57)* NS; p=0·77
Ipsilateral carotid stroke at 5 years†86 5% 3% 1·29 (0·74–2·24) NS; p=0·36
Longer-term therapy in patients with TIA or ischaemic stroke
Aspirin88
Stroke per year 4% 5% 0·83 (0·72–0·96) 0·8%
Clopidogrel (vs aspirin)89
Recurrent stroke at 2 years 11% 12% 0·90 (0·80–1·00)‡ 1%
Aspirin plus ER dipyridamole (vs aspirin)90
Recurrent stroke at 2·6 years 9% 11% 0·78 (0·68–0·90)* 2·3%
Aspirin plus ER dipyridamole (vs clopidogrel)91
Recurrent stroke at 2·5 years 9% 9% 1·01 (0·92–1·11)* NS; p=0·71
Cilostazol (vs aspirin)92
Recurrent stroke at 3 years 5% 8% 0·67 (0·52–0·86) 2·7%
Blood pressure lowering by 5·1/2·5 mm Hg93
Recurrent stroke at 3 years 9% 10% 0·78 (0·68–0·90) ‡ 1·3%
LDL cholesterol lowering by 1 mmol/L94
Recurrent stroke at 5 years 11% 12% 0·88 (0·78–0·99) 1·4%
Pioglitazone for insulin resistance21
Stroke or myocardial infarction 9% 12% 0·76 (0·62–0·93)* 2·8%
Recurrent stroke at 4·8 years 7% 8% 0·82 (0·61–1·10)* NS; p=0·19
Warfarin for atrial fibrillation (vs control)95
Recurrent stroke at 2 years 9% 23% 0·36 (0·22–0·58)‡ 14%
Direct oral anticoagulants (vs warfarin)96
Stroke or systemic embolism at 2 years 5% 6% 0·86 (0·76–0·98) 0·8%
Left atrial appendage closure (vs warfarin)97
Stroke or systemic embolism at 2·7 years 1·75% per year 1·87% per year 1·02 (0·62–1·7)* NS; p=0·94
Patent foramen ovale closure (vs medical therapy)98
Recurrent ischaemic stroke 0·7% per year 1·3% per year 0·58 (0·34–0·99)* 0·6%
TIA=transient ischaemic attack. NS=not significant. ER=extended release. *Hazard ratio and 95% CI. †Ipsilateral carotid-territory stroke from the end of the periprocedural period (30 days after completed
treatment). ‡Odds ratio and 95% CI.
Table 4: Effect of secondary prevention strategies to prevent recurrent stroke
www.thelancet.com Published online September 13, 2016 http://dx.doi.org/10.1016/S0140-6736(16)30962-X 7
Seminar
extracranial to intracranial bypass surgery over medical valves.118 Selection of anticoagulant drugs is individualised
therapy for most patients with internal carotid artery according to hepatic and renal function, potential for
occlusion and severe haemodynamic impairment drug interactions, patient preference, cost, tolerability,
because of the increased perioperative morbidity.109 and, among patients taking warfarin, time in the INR
Sustained lowering of blood pressure by 5·1 mm Hg therapeutic range.
systolic and 2·5 mm Hg diastolic reduces recurrent The optimal time to start oral anticoagulation in acute
stroke by about a fifth (table 4).93 More intensive blood cardioembolic stroke is uncertain and the subject of
pressure lowering further reduces stroke risk.15 The ongoing trials (appendix). However, it is probably
optimal target blood pressure is uncertain, but might be between 4 days and 14 days after stroke onset, depending
120–128 mm Hg systolic and 65–70 mm Hg diastolic on the balance between the risk of recurrent stroke
after lacunar stroke.110 Visit-to-visit blood pressure (CHA2DS2-VASc score) and the risk of haemorrhagic
variability is reduced in a dose-dependent fashion by transformation of the infarcted brain (NIHSS and infarct
calcium-channel blockers and diuretics, and increased by size).119 The longer-term risk of bleeding with
β blockers.111 anticoagulation increases with higher HAS-BLED and
Lowering of LDL cholesterol concentration by about ABC bleeding scores (Age, Biomarkers [haemoglobin,
1 mmol/L with statins reduces the risk of recurrent cTn-hs, and GDF-15 or cystatin C/CKD-EPI] and Clinical
stroke by about 12%.94 More intensive lowering of LDL history of previous bleeding]).120 For anticoagulated
cholesterol concentration is associated with further patients who have serious bleeding or need an urgent
reductions in stroke risk.16 The optimum target LDL procedure, the anticoagulant effects of dabigatran can be
cholesterol concentration (2·59 mmol/L vs 1·8 mmol/L) reversed rapidly by idarucizumab.62 Reversal agents for
is being evaluated in the TST trial (appendix). Xa inhibitors in development include andexanet alfa, a
Long-term intensive glucose lowering does not reduce catalytically inactive recombinant human factor Xa
non-fatal stroke risk compared with standard care in variant that competitively binds Xa inhibitors,63 and
patients with type 2 diabetes.112 Insulin sensitivity can be ciraparantag (aripazine), a synthetic antidote to direct
improved by exercise, diet, weight reduction, and thrombin and Xa inhibitors.64
peroxisome proliferator-activated receptor γ (PPAR-γ) If anticoagulation for atrial fibrillation is contraindicated,
agonists. The PPAR-γ agonist, pioglitazone, reduces the left atrial appendage closure is an option given its comparable
risk of recurrent stroke or myocardial infarction (table 4)21 efficacy to warfarin (table 4).97 The combination of clopidogrel
but might increase the risk of bladder cancer, which and aspirin is less effective than warfarin in patients with
might preclude its use.113 Lowering homocysteine with atrial fibrillation but is more effective than aspirin.
B vitamins has not been proven to significantly reduce Antiplatelet therapy and anticoagulation are associated
the risk of recurrent stroke.114 with similar rates of recurrent stroke in observational
Hormone therapy for post-menopausal women should studies of patients with cryptogenic stroke and patent
probably be stopped, if possible, as it increases the risk of foramen ovale.121 Transcatheter-device patent foramen ovale
stroke by about a quarter.115 Regular physical activity, closure is associated with a marginally reduced rate of
low-risk diet (eg, Mediterranean diet), low alcohol recurrent ischaemic stroke compared with medical therapy
consumption, smoking cessation, avoidance of passive in patients with patent foramen ovale and cryptogenic
smoking, and weight reduction, as appropriate, are stroke or TIA but an increased risk of new-onset atrial
recommended. However, reliable evidence for their fibrillation.98 Ongoing trials are assessing the effectiveness
efficacy to reduce recurrent stroke is not available. of antiplatelet therapy compared with patent foramen
Multimodal interventions that address lifestyle and ovale closure and compared with oral anticoagulants in
behaviour can improve drug compliance and reduce patients with patent foramen ovale-associated cryptogenic
blood pressure, but their effect on major vascular events stroke (appendix).
is not known.116,117
Recovery and rehabilitation
Preventing recurrent ischaemic stroke of cardiac Patients with acute stroke need assessment for the nature
origin and severity of their neurological deficits and the prognosis,
In patients with atrial fibrillation, oral anticoagulation goals, and rehabilitation requirements for recovery. Stroke
with vitamin K antagonists, such as warfarin, to maintain rehabilitation is a progressive, dynamic, goal-orientated
an INR of 2·0–3·0, decreases the odds of recurrent process aimed at enabling a person with impairment to
stroke by two-thirds.95 The four direct oral anticoagulants reach their optimal physical, cognitive, emotional,
that inhibit thrombin (dabigatran etexilate) and factor Xa communicative, social, and functional activity level.122
(rivaroxaban, apixaban, and edoxaban) reduce recurrent Physical rehabilitation improves functional recovery
stroke and systemic embolism by about a sixth, without after stroke, and incorporates functional task training;
increasing major bleeding, compared to warfarin in non- active and passive musculoskeletal, neurophysiological,
valvular atrial fibrillation.96 Dabigatran is not as effective and cardiopulmonary intervention; and assistive devices
or safe as warfarin in patients with mechanical heart and modalities.123
8 www.thelancet.com Published online September 13, 2016 http://dx.doi.org/10.1016/S0140-6736(16)30962-X
Seminar
Very early, high-intensity, and frequent mobilisation stroke140 and stereotactic intracerebral transplantation of
has a less favourable outcome at 3 months after stroke human neural stems cells in patients with chronic
compared with usual care, particularly in patients with (6–60 months) stroke.141 Stem-cell therapy aims to
intracerebral haemorrhage, suggesting that mobilisation protect subacutely ischaemic and surrounding brain by
of patients in the first 24 h after stroke should be cautious suppressing inflammation and apoptosis, and to repair
and restricted to only a few times, each less than 10 min.124 and regenerate chronically damaged brain by
Hand and arm function might be improved by stimulating growth factor secretion, cell replacement,
constraint-induced movement therapy, frequent and biobridge formation.
repetitive task practice, mental practice, mirror therapy, Early supported discharge services that are
interventions for sensory impairment, and virtual reality, appropriately resourced and have a coordinated team
but the quality of the supporting evidence is only can reduce length of hospital stay, admission to
moderate125 and the results not all favourable.126 institutional care, and long-term dependency in elderly
Constraint-induced movement therapy involves stroke patients with mild to moderate disability without
constraining the non-paretic arm (eg, wearing a mitt on adversely affecting the mood or subjective health status
the non-paretic hand) and undertaking graded task- of patients or carers.142 Stroke survivors and their
oriented training of the paretic arm. Robot-assisted, task- caregivers should be encouraged to join their local stroke
orientated, arm training devices could improve muscle support organisation. Support and advice from
strength and function in the paretic arm, but the quality organisations and from other stroke patients and their
of the evidence is low.127 family can reduce social isolation and depression and
Cardiorespiratory fitness training that involves walking improve quality of life.
improves balance and walking speed and capacity, but its
effect on death and dependence is uncertain.128 Treadmill Interventions under investigation and future
training, with or without bodyweight support using a directions
harness, might improve walking speed and walking Several promising interventions are undergoing evaluation
endurance in patients who are able to walk after stroke.129 (appendix). The initial management of acute stroke is
For patients who cannot walk independently, robotic- being extended from hospital emergency departments to
assisted gait training, combined with physical therapy, ambulances where opportunities exist to intervene in the
might increase the odds of walking independently.129 first—so-called golden—hour. Ambulance-based
Rhythmic auditory stimulation (ie, music therapy) could interventions undergoing evaluation include stroke
also help to improve gait parameters in patients with assessment tools for paramedics to reliably identify
stroke.130 patients with large artery occlusion, ambulance-based
Intramuscular injection of botulinum toxin type A is mobile brain imaging and point-of-care laboratory tests to
safe and reduces local muscle tone and pain due to distinguish haemorrhagic from ischaemic stroke,
spasticity for up to 3 months after stroke. However, telemedicine communication with the admitting
whether it improves upper limb capacity or is cost-effective emergency department or stroke team, stroke care
is uncertain.131 Neuromuscular electric stimulation also algorithms, altering head position to optimise brain
reduces spasticity and improves range of motion after perfusion, lowering blood pressure to prevent haematoma
stroke.132 expansion, lowering body temperature to protect ischaemic
Speech and language therapy for post-stroke aphasia brain tissue, starting neuroprotective and anti-
improves functional communication compared with no inflammatory drugs, and starting intravenous thrombolysis
speech and language therapy, but not compared with social or haemostatic therapy in appropriate patients.
support and stimulation.133 Transcranial direct-current Ongoing trials are investigating strategies to improve
stimulation does not seem to improve post-stroke the safety of thrombolysis (eg, by lowering blood pressure
functional communication, language impairment, or and using specific antidotes for patients taking direct oral
cognition.134 Cognitive rehabilitation interventions have not anticoagulants), to improve the efficacy of thrombolysis
proved effective for reducing attentional impairments, (eg, by combining thrombolysis with neuroprotective
executive dysfunction, or spatial neglect.135–137 and anti-inflammatory therapies such as uric acid,
There is insufficient evidence for the efficacy of any minocycline, fingolimod, natalizumab, growth factors,
intervention to treat or prevent fatigue after stroke.138 and hypothermia), to identify more effective thrombolytic
Small trials suggest that neurotrophic drugs, such as drugs (eg, tenecteplase), and to determine the brain
cerebrolysin and selective serotonin-reuptake inhibitors, imaging and threshold measures of volume of core
might improve neurological recovery from stroke but infarction and penumbral mismatch (ratio of ischaemic
the results are inconclusive and subject to evaluation in tissue at risk to core infarction) that might optimise
ongoing trials (appendix).139 Preliminary evidence patient selection and extend the time window for effective
supports the feasibility, tolerability and safety of reperfusion therapy.
intravenous transplantation of autologous bone marrow The evidence base for effective mechanical
mononuclear cells in patients with subacute (7–30 days) thrombectomy has so far been derived from experienced,
www.thelancet.com Published online September 13, 2016 http://dx.doi.org/10.1016/S0140-6736(16)30962-X 9
Seminar
comprehensive stroke centres; therefore, registry studies stimulation, transcranial direct-current stimulation,
are planned in less experienced centres to verify acupuncture, vagus nerve stimulation paired with upper-
generalisability and external validity. The effect of limb rehabilitation, intensive aphasia therapy, hands-on
endovascular thrombectomy also awaits investigation in therapy, music therapy, interventions for sensory
patients with mild ischaemic stroke (eg, NIHSS impairment, pharmacological interventions for recovery
score <10), basilar artery occlusion, or distal occlusions of such as cerebrolysin and fluoxetine, and intrastriatal
the M2 middle cerebral artery segment, as does the injection of allogeneic human neural stem cells.
optimum treatment for patients with concomitant Because most strokes occur in LMICs where access to
(tandem) occlusion of the extracranial internal carotid stroke units and rehabilitation is poor, a trial in India is
artery. It is also uncertain whether proceeding directly to examining whether rehabilitation in the home by a
thrombectomy, and withholding alteplase in alteplase- trained family member is effective and affordable for
eligible patients, in patients with large artery occlusion patients with recent disabling stroke, compared with
will improve safety and efficacy compared with the usual care.
current approach of combined alteplase and endovascular
therapy. Efforts are ongoing to improve the technological Conclusion
aspects of mechanical thrombectomy to further reduce The past decade has seen extraordinary advances in the
procedural time, increase the rate of complete treatment and prevention of stroke. The most exciting
reperfusion, and minimise harm. has been the dramatic effect of endovascular
Ongoing studies in acute haemorrhagic stroke promise thrombectomy in reducing death and dependency
to provide evidence of the clinical effectiveness of for an additional one in five patients with acute large
prehospital blood pressure lowering, neuroprotection vessel ischaemic stroke. This advance reflects a dedicated
and anti-inflammation (eg, fingolimod), non-specific commitment to harmoniously integrating efficient,
haemostatic and antifibrinolytic therapies, specific expert multidisciplinary systems of stroke care with
antidotes to direct oral anticoagulants, and minimally advances in brain imaging and stent-retriever technology.
invasive surgery via burr hole combined with local The findings present implementation challenges for
thrombolysis. stroke networks. Also salutary are the lower rates of
To prevent recurrent atherothrombotic ischaemic stroke, recurrent stroke in the past decade. The magnitude and
trials are in progress or being planned to assess the nature of the early benefits of immediate aspirin for TIA
incremental benefit of adding aspirin to clopidogrel, and ischaemic stroke are now recognised. Intensive and
cilostazol, a potent selective protease-activated sustained reductions in blood pressure and cholesterol
receptor 4 (PAR4) antagonist, ticagrelor, rivaroxaban, or and carotid revascularisation for select patients with
the combination of clopidogrel and dipyridamole. Trials symptomatic carotid stenosis are associated with rates of
of drugs that inactivate proprotein convertase less than 1% per year of post-procedural recurrent
subtilisin/kexin type 9 (PCSK9) by means of humanised ipsilateral stroke at 5 years after carotid endarterectomy
monoclonal anti-PCSK9 antibodies, and lower or stenting; several-times lower than rates for similar
LDL-cholesterol concentrations by at least 50%, are awaited patients treated medically 25 years ago (table 4).84–87
in patients with ischaemic stroke. Cerebral small-vessel Recent evidence indicates that treating insulin resistance
disease might be prevented by interventions that target also prevents recurrent vascular events. The advent of
brain microvascular endothelium and the blood–brain direct oral anticoagulants has increased the uptake of
barrier, microvascular function, and neuroinflammation. effective anticoagulant thromboprophylaxis among
To prevent embolic stroke of uncertain source, three patients with atrial fibrillation at high risk of recurrent
trials are evaluating the effect of the direct oral cardioembolic stroke. However, despite these advances,
anticoagulants rivaroxaban, dabigatran, and apixaban, the global burden of stroke remains substantial and is
compared with aspirin. To prevent ischaemic events after increasing as populations age. There is no country in
intracerebral haemorrhage, the safety and effectiveness of which the number of people affected by stroke has
starting or restarting antithrombotic treatment is being decreased in the past two decades. The burden of stroke
addressed in ongoing trials. Other potential new strategies is also increasing among young adults and is greatest in
of stroke prevention that are being evaluated include developing countries. An improved understanding of,
ischaemic preconditioning and treating obstructive sleep and commitment to, the disparities in stroke burden
apnoea with continuous positive airway pressure. trends and access to appropriate and affordable stroke
High-quality randomised controlled trials are needed care between countries and regions of different income
to establish the observed benefits of constraint-induced levels is needed to address the increasing global burden
movement therapy, mental practice, mirror therapy, of stroke.
virtual reality and interactive video gaming, and relatively Declaration of interests
intense repetitive task practice. I have received honoraria from AC Immune for chairing the data safety
Trials are also needed to provide more reliable estimates monitoring committee of two clinical trials of vaccines for Alzheimer’s
disease, from Bayer for lecturing about stroke prevention in atrial
of the effects of repetitive transcranial magnetic
10 www.thelancet.com Published online September 13, 2016 http://dx.doi.org/10.1016/S0140-6736(16)30962-X
Seminar
fibrillation at sponsored scientific symposia, and from Medscape, 20 Zhang C, Qin YY, Chen Q, et al. Alcohol intake and risk of stroke:
Web MD, for participating in a discussion about stroke prevention in a dose response meta-analysis of prospective studies.
atrial fibrillation for theheart.org. Int J Cardiol 2014; 174: 669–77.
21 Kernan WN, Viscoli CM, Furie KL, et al, for the IRIS Trial
Acknowledgments
Investigators. Pioglitazone after Ischemic Stroke or Transient
I thank Jeffrey L Saver (University of California, Los Angeles, USA) Ischemic Attack. N Engl J Med 2016; 374: 1321–31.
for helpful comments and suggestions regarding the manuscript.
22 Peters SA, Huxley RR, Woodward M. Diabetes as a risk factor for
References stroke in women compared with men: a systematic review and
1 Feigin VL, Forouzanfar MH, Krishnamurthi R, for the Global meta-analysis of 64 cohorts, including 775 385 individuals and
Burden of Diseases, Injuries, and Risk Factors Study 2010 12 539 strokes. Lancet 2014; 383: 1973–80.
(GBD 2010) and the GBD Stroke Experts Group. Global and 23 O’Donnell MJ, Chin SL, Rangarajan S, et al, for the INTERSTROKE
regional burden of stroke during 1990–2010: findings from the investigators. Global and regional effects of potentially modifiable
Global Burden of Disease Study 2010. Lancet 2014; 383: 245–54. risk factors associated with acute stroke in 32 countries
2 Krishnamurthi RV, Feigin VL, Forouzanfar MH, et al, for the Global (INTERSTROKE): a case-control study. Lancet 2016; 388: 761–75.
Burden of Diseases, Injuries, Risk Factors Study 2010 (GBD 2010), 24 Feigin VL, Roth GA, Naghavi M, for the Global Burden of Diseases,
for the GBD Stroke Experts Group. Global and regional burden of Injuries and Risk Factors Study 2013 and Stroke Experts Writing
first-ever ischaemic and haemorrhagic stroke during 1990–2010: Group. Global burden of stroke and risk factors in 188 countries,
findings from the Global Burden of Disease Study 2010. during 1990–2013: a systematic analysis for the Global Burden of
Lancet Glob Health 2013; 1: e259–81. Disease Study 2013. Lancet Neurol 2016; 15: 913–24.
3 Sacco RL, Kasner SE, Broderick JP, et al. An updated definition of 25 NINDS Stroke Genetics Network (SiGN) and International Stroke
stroke for the 21st century: a statement for healthcare professionals Genetics Consortium. Loci associated with ischaemic stroke and its
from the American Heart Association/American Stroke subtypes (SiGN): a genome-wide association study. Lancet Neurol
Association. Stroke 2013; 44: 2064–89. 2016; 15: 174–84.
4 Hankey GJ, Blacker DJ. Is it a stroke? BMJ 2015; 350: h56. 26 Neurology Working Group of the Cohorts for Heart and Aging Research
5 Whiteley WN, Wardlaw JM, Dennis MS, Sandercock PA. Clinical in Genomic Epidemiology (CHARGE) Consortium; Stroke Genetics
scores for the identification of stroke and transient ischaemic attack Network (SiGN); International Stroke Genetics Consortium (ISGC).
in the emergency department: a cross-sectional study. Identification of additional risk loci for stroke and small vessel disease:
J Neurol Neurosurg Psychiatry 2011; 82: 1006–10. a meta-analysis of genome-wide association studies. Lancet Neurol 2016;
6 Brunser AM, Hoppe A, Illanes S, et al. Accuracy of diffusion- 15: 695–707.
weighted imaging in the diagnosis of stroke in patients with 27 Guiraud V, Amor MB, Mas JL, Touze E. Triggers of ischemic stroke:
suspected cerebral infarct. Stroke 2013; 44: 1169–71. A systematic review. Stroke 2010; 41: 2669–77.
7 Brazzelli M, Chappell FM, Miranda H, et al. Diffusion-weighted 28 Luengo-Fernandez R, Paul NL, Gray AM, et al, for the Oxford Vascular
imaging and diagnosis of transient ischemic attack. Ann Neurol Study. Population-based study of disability and institutionalization
2014; 75: 67–76. after transient ischemic attack and stroke: 10-year results of the Oxford
8 Gibson LM, Whiteley W. The differential diagnosis of suspected Vascular Study. Stroke 2013; 44: 2854–61.
stroke: a systematic review. J R Coll Physicians Edinb 2013; 29 Poon MT, Fonville AF, Al-Shahi Salman R. Long-term prognosis
43: 114–48. after intracerebral haemorrhage: systematic review and
9 Bamford J, Sandercock P, Dennis M, Burn J, Warlow C. meta-analysis. J Neurol Neurosurg Psychiatry 2014; 85: 660–67.
Classification and natural history of clinically identifiable subtypes 30 Ayis SA, Coker B, Rudd AG, Dennis MS, Wolfe CD.
of cerebral infarction. Lancet 1991; 337: 1521–26. Predicting independent survival after stroke: a European study for
10 Adams HP Jr, Bendixen BH, Kappelle LJ, et al. Classification of the development and validation of standardised stroke scales and
subtype of acute ischemic stroke. Definitions for use in a prediction models of outcome. J Neurol Neurosurg Psychiatry 2013;
multicenter clinical trial. TOAST. Trial of Org 10172 in Acute Stroke 84: 288–96.
Treatment. Stroke 1993; 24: 35–41. 31 Coull AJ, Lovett JK, Rothwell PM, for the Oxford Vascular Study.
11 Amarenco P, Bogousslavsky J, Caplan LR, Donnan GA, Wolf ME, Population based study of early risk of stroke after transient
Hennerici MG. The ASCOD phenotyping of ischemic stroke ischaemic attack or minor stroke: implications for public education
(Updated ASCO Phenotyping). Cerebrovasc Dis 2013; 36: 1–5. and organisation of services. BMJ 2004; 328: 326.
12 Ay H, Benner T, Arsava EM, et al. A computerized algorithm for 32 Kiyohara T, Kamouchi M, Kumai Y, et al, for the Fukuoka Stroke
etiologic classification of ischemic stroke: the Causative Registry Investigators. ABCD3 and ABCD3-I scores are superior to
Classification of Stroke System. Stroke 2007; 38: 2979–84. ABCD2 score in the prediction of short- and long-term risks of
stroke after transient ischemic attack. Stroke 2014; 45: 418–25.
13 Hart RG, Diener HC, Coutts SB, et al, and the Cryptogenic
Stroke/ESUS International Working Group. Embolic strokes of 33 Arsava EM, Kim G-M, Oiverira-Filho J, et al. Prediction of Early
undetermined source: the case for a new clinical construct. Recurrence after Acute Ischemic Stroke. JAMA Neurol 2016;
Lancet Neurol 2014; 13: 429–38. 73: 396–401.
14 Rannikmäe L, Woodfield R, Anderson CS, et al. Reliability of 34 Wardlaw JM, Brazzelli M, Chappell FM, et al. ABCD2 score and
intracerebral haemorrhage classification systems: a systematic secondary stroke prevention: meta-analysis and effect per 1000
review. Int J Stroke 2016; 11: 626–36. patients triaged. Neurology 2015; 85: 373–80.
15 Xie X, Atkins E, Lv J, et al. Effects of intensive blood pressure 35 Rothwell PM, Giles MF, Chandratheva A, et al. for the Early use of
lowering on cardiovascular and renal outcomes: updated systematic Existing Preventive Strategies for Stroke (EXPRESS) study. Effect
review and meta-analysis. Lancet 2016; 387: 435–43. of urgent treatment of transient ischaemic attack and minor stroke
on early recurrent stroke (EXPRESS study): a prospective
16 Collins R, Reith C, Emberson J, et al. Interpretation of the evidence for
population-based sequential comparison. Lancet 2007;
the efficacy and safety of statin therapy. Lancet 2016; published online
370: 1432–42.
Sept 8. http://dx.doi.org/10.1016/S0140-6736(16)31357-5.
36 Amarenco P, Lavallée PC, Labreuche J, et al, for the TIAregistry.
17 Raman G, Moorthy D, Hadar N, et al. Management strategies for
org Investigators. One-Year Risk of Stroke after Transient
asymptomatic carotid stenosis: a systematic review and
Ischemic Attack or Minor Stroke. N Engl J Med 2016; 374: 1533–42.
meta-analysis. Ann Intern Med 2013; 158: 676–85.
37 Mohan KM, Wolfe CD, Rudd AG, et al. Risk and cumulative risk of
18 Hart RG, Pearce LA, Aguilar MI. Meta-analysis: antithrombotic
stroke recurrence: a systematic review and meta-analysis. Stroke
therapy to prevent stroke in patients who have nonvalvular atrial
2011; 42: 1489–94.
fibrillation. Ann Intern Med 2007; 146: 857–67.
38 Hijazi Z, Lindbäck J, Alexander JH, et al, for the ARISTOTLE and
19 Mons U, Müezzinler A, Gellert C, et al, for the CHANCES
STABILITY Investigators. The ABC (age, biomarkers, clinical
Consortium. Impact of smoking and smoking cessation on
history) stroke risk score: a biomarker-based risk score for
cardiovascular events and mortality among older adults:
predicting stroke in atrial fibrillation. Eur Heart J 2016;
meta-analysis of individual participant data from prospective cohort
37: 1582–90.
studies of the CHANCES consortium. BMJ 2015; 350: h1551.
www.thelancet.com Published online September 13, 2016 http://dx.doi.org/10.1016/S0140-6736(16)30962-X 11
Seminar
39 Biffi A, Anderson CD, Battey TW, et al. Association between blood 58 Yuan ZH, Jiang JK, Huang WD, Pan J, Zhu JY, Wang JZ.
pressure control and risk of recurrent intracerebral hemorrhage. A meta-analysis of the efficacy and safety of recombinant activated
JAMA 2015; 314: 904–12. factor VII for patients with acute intracerebral hemorrhage without
40 Emberson J, Lees KR, Lyden P, et al, for the Stroke Thrombolysis hemophilia. J Clin Neurosci 2010; 17: 685–93.
Trialists’ Collaborative Group. Effect of treatment delay, age, and 59 Baharoglu MI, Cordonnier C, Salman RA, and the PATCH
stroke severity on the effects of intravenous thrombolysis with Investigators. Platelet transfusion versus standard care after acute
alteplase for acute ischaemic stroke: a meta-analysis of individual stroke due to spontaneous cerebral haemorrhage associated with
patient data from randomised trials. Lancet 2014; 384: 1929–35. antiplatelet therapy (PATCH): a randomised, open-label, phase 3 trial.
41 Badhiwala JH, Nassiri F, Alhazzani W, et al. Endovascular Lancet 2016; 387: 2605–13.
thrombectomy for acute ischemic stroke: a meta-analysis. 60 Kuramatsu JB, Gerner ST, Schellinger PD, et al. Anticoagulant
JAMA 2015; 314: 1832–43. reversal, blood pressure levels, and anticoagulant resumption in
42 Goyal M, Menon BK, van Zwam WH, et al, for the HERMES patients with anticoagulation-related intracerebral hemorrhage.
collaborators. Endovascular thrombectomy after large-vessel JAMA 2015; 313: 824–36.
ischaemic stroke: a meta-analysis of individual patient data from 61 Steiner T, Poli S, Griebe M, et al. Fresh frozen plasma versus
five randomised trials. Lancet 2016; 387: 1723–31. prothrombin complex concentrate in patients with intracranial
43 Sandercock PA, Counsell C, Tseng MC, Cecconi E. Oral antiplatelet haemorrhage related to vitamin K antagonists (INCH):
therapy for acute ischaemic stroke. Cochrane Database Syst Rev 2014; a randomised trial. Lancet Neurol 2016; 15: 566–73.
3: CD000029. 62 Pollack CV Jr, Reilly PA, Eikelboom J, et al. Idarucizumab for
44 Yang MH, Lin HY, Fu J, Roodrajeetsing G, Shi SL, Xiao SW. dabigatran reversal. N Engl J Med 2015; 373: 511–520.
Decompressive hemicraniectomy in patients with malignant 63 Siegal DM, Curnutte JT, Connolly SJ, et al. Andexanet alfa for the
middle cerebral artery infarction: A systematic review and reversal of factor Xa inhibitor activity. N Engl J Med 2015;
meta-analysis. Surgeon 2015; 13: 230–40. 373: 2413–24.
45 Tsivgoulis G, Katsanos AH, Butcher KS, et al, Intensive blood 64 Ansell JE, Bakhru SH, Laulicht BE, et al. Use of PER977 to reverse
pressure reduction in acute intracerebral hemorrhage: the anticoagulant effect of edoxaban. N Engl J Med 2014; 371: 2141–42.
a meta-analysis. Neurology 2014; 83: 1523–29. 65 Aronis KN, Hylek EM. Who, when, and how to reverse non-vitamin
46 Qureshi AI, Palesch YY, Barsan WG, et al, and the ATACH-2 Trial K oral anticoagulants. J Thromb Thrombolysis 2016; 41: 253–72.
Investigators and the Neurological Emergency Treatment Trials 66 Gregson BA, Broderick JP, Auer LM, et al. Individual patient data
Network. Intensive blood-pressure lowering in patients with acute subgroup meta-analysis of surgery for spontaneous supratentorial
cerebral hemorrhage. N Engl J Med 2016 June 8. DOI:10.1056/ intracerebral hemorrhage. Stroke 2012; 43: 1496–504.
NEJMoa1603460. 67 Mould WA, Carhuapoma JR, Muschelli J, et al. Minimally invasive
47 Mendelow AD, Gregson BA, Rowan EN, et al. Early surgery versus surgery plus recombinant tissue-type plasminogen activator for
initial conservative treatment in patients with spontaneous intracerebral hemorrhage evacuation decreases perihematomal
supratentorial lobar intracerebral haematomas (STICH II): edema. Stroke 2013; 44: 627–34.
a randomised trial. Lancet 2013; 382: 397–408. 68 Ziai WC, Tuhrim S, Lane K, for the CLEAR III Investigators.
48 Stroke Unit Trialists’ Collaboration. Organised inpatient (stroke unit) A multicenter, randomized, double-blinded, placebo-controlled
care for stroke. Cochrane Database Syst Rev 2013; 9: CD000197. phase III study of Clot Lysis Evaluation of Accelerated Resolution of
49 Strbian D, Michel P, Seiffge DJ, et al. Symptomatic intracranial Intraventricular Hemorrhage (CLEAR III). Int J Stroke
hemorrhage after stroke thrombolysis: comparison of prediction 2014; 9: 536–42.
scores. Stroke 2014; 45: 752–58. 69 Bray BD, Ayis S, Campbell J, et al. Associations between the
50 Anderson CS, Robinson T, Lindley RI, et al, for the ENCHANTED organisation of stroke services, process of care, and mortality in
Investigators and Coordinators. Low-Dose versus standard-dose England: prospective cohort study. BMJ 2013; 346: f2827.
intravenous alteplase in acute ischemic stroke. N Engl J Med 2016; 70 Langhorne P, de Villiers L, Pandian JD. Applicability of stroke-unit
374: 2313–23. care to low-income and middle-income countries. Lancet Neurol
51 Schellinger PD, Alexandrov AV, Barreto AD, for the CLOTBUSTER 2012; 11: 341–48.
Investigators. Combined lysis of thrombus with ultrasound and 71 Visvanathan A, Dennis M, Whiteley W. Parenteral fluid regimens
systemic tissue plasminogen activator for emergent for improving functional outcome in people with acute stroke.
revascularization in acute ischemic stroke (CLOTBUST-ER): Cochrane Database Syst Rev 2015; 9: CD011138.
design and methodology of a multinational phase 3 trial. Int J Stroke 72 Cohen DL, Roffe C, Beavan J, et al. Post-stroke dysphagia: a review
2015; 10: 1141–48. and design considerations for future trials. Int J Stroke 2016;
52 Lyden PD, Hemmen TM, Grotta J, Rapp K, Raman R. Endovascular 11: 399–411.
therapeutic hypothermia for acute ischemic stroke: ICTuS 2/3 73 Chamorro Á, Dirnagl U, Urra X, Planas AM. Neuroprotection in
protocol. Int J Stroke 2014; 9: 117–25. acute stroke: targeting excitotoxicity, oxidative and nitrosative stress,
53 Albers GW, von Kummer R, Truelsen T, et al, for the DIAS-3 and inflammation. Lancet Neurol 2016; 15: 869–81.
Investigators. Safety and efficacy of desmoteplase given 3–9 h 74 Bath PM, Krishnan K. Interventions for deliberately altering blood
after ischaemic stroke in patients with occlusion or high-grade pressure in acute stroke. Cochrane Database Syst Rev 2014;
stenosis in major cerebral arteries (DIAS-3): a double-blind, 10: CD000039.
randomised, placebo-controlled phase 3 trial. Lancet Neurol 2015;
75 Bath PM, Woodhouse L, Scutt P, et al, for the ENOS Trial
14: 575–84.
Investigators Efficacy of nitric oxide, with or without continuing
54 Huang X, MacIsaac R, Thompson JL, et al. Tenecteplase versus antihypertensive treatment, for management of high blood pressure
alteplase in stroke thrombolysis: an individual patient data in acute stroke (ENOS): a partial-factorial randomised controlled
meta-analysis of randomized controlled trials. Int J Stroke 2016; trial. Lancet 2015; 385: 617–28.
11: 534–43.
76 Bellolio MF, Gilmore RM, Ganti L. Insulin for glycaemic control in
55 Zinkstok SM, Roos YB, for the ARTIS investigators. Early acute ischaemic stroke. Cochrane Database Syst Rev 2014;
administration of aspirin in patients treated with alteplase for 1: CD005346.
acute ischaemic stroke: a randomised controlled trial. Lancet 2012;
77 Westendorp WF, Vermeij JD, Zock E, et al, for the PASS
380: 731–37.
investigators. The Preventive Antibiotics in Stroke Study (PASS):
56 Warach SJ, Luby M, Albers GW, et al, for the Stroke Imaging a pragmatic randomised open-label masked endpoint clinical trial.
Research (STIR) and VISTA-Imaging Investigators. Acute stroke Lancet 2015; 385: 1519–26.
imaging research roadmap III imaging selection and outcomes in
78 Kalra L, Irshad S, Hodsoll J, et al, for the STROKE-INF
acute stroke reperfusion clinical trials: consensus recommendations
Investigators. Prophylactic antibiotics after acute stroke for
and further research priorities. Stroke 2016; 47: 1389–98.
reducing pneumonia in patients with dysphagia (STROKE-INF):
57 Goyal M, Yu AY, Menon BK, et al. Endovascular therapy in acute a prospective, cluster-randomised, open-label, masked endpoint,
ischemic stroke: challenges and transition from trials to bedside. controlled clinical trial. Lancet 2015; 386: 1835–44.
Stroke 2016; 47: 548–53.
12 www.thelancet.com Published online September 13, 2016 http://dx.doi.org/10.1016/S0140-6736(16)30962-X
Seminar
79 CLOTS (Clots in Legs Or sTockings after Stroke) Trials 98 Kent DM, Dahabreh JH, Ruthazer R, et al. Device closure of patent
Collaboration. Effect of intermittent pneumatic compression on foramen ovale after stroke: Pooled analysis from all completed
disability, living circumstances, quality of life, and hospital costs randomized trials. J Am Coll Cardiol 2016; 67: 907–17.
after stroke: secondary analyses from CLOTS 3, a randomised trial. 99 Wang Y, Zhao X, Lin J, et al for the CHANCE investigators.
Lancet Neurol 2014; 13: 1186–92. Loss-of-function allele status and efficacy of clopidogrel for risk
80 Geeganage CM, Sprigg N, Bath MW, Bath PMW. Balance of reduction among patients with minor stroke or transient ischemic
symptomatic pulmonary embolism and symptomatic attack. JAMA 2016; 316: 70–78.
intracerebral hemorrhage with low-dose anticoagulation in recent 100 Lee M, Saver JL, Hong KS, Rao NM, Wu YL, Ovbiagele B.
ischemic stroke: a systematic review and meta-analysis of Risk-benefit profile of long-term dual- versus single-antiplatelet
randomized controlled trials. J Stroke Cerebrovasc Dis 2013; therapy among patients with ischemic stroke: a systematic review
22: 1018–27. and meta-analysis. Ann Intern Med 2013; 159: 463–70.
81 Rothwell PM, Algra A, Chen Z, Diener H-C, Norrving B, Mehta Z. 101 Sandercock PA, Counsell C, Kane EJ. Anticoagulants for acute
Effects of aspirin on risk and severity of early recurrent stroke after ischaemic stroke. Cochrane Database Syst Rev 2015; 3: CD000024.
transient ischaemic attack and ischaemic stroke: time-course 102 Whiteley WN, Adams HP Jr, Bath PM, et al. Targeted use of heparin,
analysis of randomised trials. Lancet 2016; 388: 365–75. heparinoids, or low-molecular-weight heparin to improve outcome
82 Johnston SC, Amarenco P, Albers GW, et al, for the SOCRATES after acute ischaemic stroke: an individual patient data meta-analysis
Steering Committee and Investigators. Ticagrelor versus aspirin in of randomised controlled trials. Lancet Neurol 2013; 12: 539–45.
acute stroke or transient ischemic attack. N Engl J Med 2016; 103 Markus HS, Hayter E, Levi C, Feldman A, Venables G, Norris J, for
375: 35–43. the CADISS trial investigators. Antiplatelet treatment compared
83 Wong KS, Wang Y, Leng X, et al. Early dual versus mono with anticoagulation treatment for cervical artery dissection
antiplatelet therapy for acute non-cardioembolic ischemic stroke or (CADISS): a randomised trial. Lancet Neurol 2015; 14: 361–67.
transient ischemic attack: an updated systematic review and 104 Rothwell PM, Mehta Z, Howard SC, et al. From subgroups to
meta-analysis. Circulation 2013; 128: 1656–66. individuals: general principles and the example of carotid
84 Rerkasem K, Rothwell PM. Carotid endarterectomy for symptomatic endarterectomy. Lancet 2005; 365: 256–65.
carotid stenosis. Cochrane Database Syst Rev 2011; 4: CD001081. 105 De Rango P, Brown MM, Chaturvedi S, et al. Summary of
85 Bonati LH, Lyrer P, Ederle J, Featherstone R, Brown MM. evidence on early carotid intervention for recently symptomatic
Percutaneous transluminal balloon angioplasty and stenting for stenosis based on meta-analysis of current risks. Stroke 2015;
carotid artery stenosis. Cochrane Database of Syst Rev 2012; 46: 3423–36.
9: CD000515. 106 Derdeyn CP, Chimowitz MI, Lynn MJ, et al. and the Stenting and
86 Bonati LH, Dobson J, Featherstone RL, et al, for the International Aggressive Medical Management for Preventing Recurrent Stroke
Carotid Stenting Study investigators. Long-term outcomes after in Intracranial Stenosis Trial Investigators. Aggressive medical
stenting versus endarterectomy for treatment of symptomatic treatment with or without stenting in high-risk patients with
carotid stenosis: the International Carotid Stenting Study (ICSS) intracranial artery stenosis (SAMMPRIS): the final results of a
randomised trial. Lancet 2015; 385: 529–38. randomised trial. Lancet 2014; 383: 333–41.
87 Brott TG, Howard G, Roubin GS, et al. Long-term results of 107 Zaidat OO, Fitzsimmons BF, Woodward BK, et al, for the VISSIT
stenting versus endarterectomy for carotid-artery stenosis. Trial Investigators. Effect of a balloon-expandable intracranial stent
N Engl J Med 2016; 374: 1021–31. vs medical therapy on risk of stroke in patients with symptomatic
88 Baigent C, Blackwell L, Collins R, et al, for the Antithrombotic intracranial stenosis: the VISSIT randomized clinical trial. JAMA
Trialists’ (ATT) Collaboration, Aspirin in the primary and secondary 2015; 313: 1240–48.
prevention of vascular disease: collaborative meta-analysis of 108 Compter A, van der Worp HB, Schonewille WJ, et al, for the VAST
individual participant data from randomised trials. Lancet 2009; investigators. Stenting versus medical treatment in patients with
373: 1849–60. symptomatic vertebral artery stenosis: a randomised open-label
89 Sudlow CL, Mason G, Maurice JB, Wedderburn CJ, Hankey GJ. phase 2 trial. Lancet Neurol 2015; 14: 606–14.
Thienopyridine derivatives versus aspirin for preventing stroke and 109 Esposito G, Amin-Hanjani S, Regli L. Role of and indications for
other serious vascular events in high vascular risk patients. bypass surgery after Carotid Occlusion Surgery Study (COSS)?
Cochrane Database Syst Rev 2009; 4: CD001246. Stroke 2016; 47: 282–90.
90 Halkes PH, Gray LJ, Bath PM, et al. Dipyridamole plus aspirin versus 110 Odden MC, McClure LA, Sawaya BP, et al. Achieved Blood Pressure
aspirin alone in secondary prevention after TIA or stroke: and Outcomes in the Secondary Prevention of Small Subcortical
a meta-analysis by risk. J Neurol Neurosurg Psychiatry 2008; Strokes Trial. Hypertension 2016; 67: 63–69.
79: 1218–23. 111 Webb AJ, Rothwell PM. Effect of dose and combination of
91 Sacco RL, Diener HC, Yusuf S, for the PRoFESS Study Group. antihypertensives on interindividual blood pressure variability:
Aspirin and extended-release dipyridamole versus clopidogrel for a systematic review. Stroke 2011; 42: 2860–65.
recurrent stroke. N Engl J Med 2008; 359: 1238–51. 112 Seidu S, Achana FA, Gray LJ, Davies MJ, Khunti K. Effects of
92 Kamal AK, Naqvi I, Husain MR, Khealani BA. Cilostazol versus glucose-lowering and multifactorial interventions on cardiovascular
aspirin for secondary prevention of vascular events after stroke of and mortality outcomes: a meta-analysis of randomized control
arterial origin. Cochrane Database Syst Rev 2011; 1: CD008076. trials. Diabet Med 2016; 33: 280–89.
93 Liu L, Wang Z, Gong L, et al. Blood pressure reduction for the 113 Tuccori M, Filion KB, Yin H, Yu OH, Platt RW, Azoulay L.
secondary prevention of stroke: a Chinese trial and a systematic Pioglitazone use and risk of bladder cancer: population based
review of the literature. Hypertens Res 2009; 32: 1032–40. cohort study. BMJ 2016; 352: i1541.
94 Amarenco P, Labreuche J. Lipid management in the prevention of 114 Martí-Carvajal AJ, Solà I, Lathyris D. Homocysteine-lowering
stroke: review and updated meta-analysis of statins for stroke interventions for preventing cardiovascular events.
prevention. Lancet Neurol 2009; 8: 453–63. Cochrane Database Syst Rev 2015; 1: CD006612.
95 Saxena R, Koudstaal PJ. Anticoagulants for preventing stroke in 115 Boardman HM, Hartley L, Eisinga A, et al. Hormone therapy for
patients with nonrheumatic atrial fibrillation and a history of stroke preventing cardiovascular disease in post-menopausal women.
or transient ischaemic attack. Cochrane Database Syst Rev 2004; Cochrane Database Syst Rev 2015; 3: CD002229.
2: CD000185. 116 Lennon O, Galvin R, Smith K, Doody C, Blake C. Lifestyle
96 Ruff CT, Giugliano RP, Braunwald E, et al. Comparison of the interventions for secondary disease prevention in stroke and
efficacy and safety of new oral anticoagulants with warfarin in transient ischaemic attack: a systematic review. Eur J Prev Cardiol
patients with atrial fibrillation: a meta-analysis of randomised trials. 2014; 21: 1026–39.
Lancet 2014; 383: 955–62. 117 Lawrence M, Pringle J, Kerr S, Booth J, Govan L, Roberts NJ.
97 Holmes DR Jr, Doshi SK, Kar S, et al. Left atrial appendage closure Multimodal secondary prevention behavioral interventions for TIA
as an alternative to warfarin for stroke prevention in atrial and stroke: a systematic review and meta-analysis. PLoS One 2015;
fibrillation: a patient-level meta-analysis. J Am Coll Cardiol 2015; 10: e0120902.
65: 2614–23.
www.thelancet.com Published online September 13, 2016 http://dx.doi.org/10.1016/S0140-6736(16)30962-X 13
Seminar
118 Eikelboom JW, Connolly SJ, Brueckmann M, for the RE-ALIGN 131 Gracies JM, Brashear A, Jech R, et al. for the International
Investigators. Dabigatran versus warfarin in patients with AbobotulinumtoxinA Adult Upper Limb Spasticity Study Group.
mechanical heart valves. N Engl J Med 2013; 369: 1206–14. Safety and efficacy of abobotulinumtoxinA for hemiparesis in adults
119 Paciaroni M, Agnelli G, Falocci N, et al. Early recurrence and with upper limb spasticity after stroke or traumatic brain injury:
cerebral bleeding in patients with acute ischemic stroke and atrial a double-blind randomised controlled trial. Lancet Neurol 2015;
fibrillation: effect of anticoagulation and its timing: the RAF Study. 14: 992–1001.
Stroke 2015; 46: 2175–82. 132 Stein C, Fritsch CG, Robinson C, Sbruzzi G, Plentz RD. Effects of
120 Hijazi Z, Oldgren J, Lindbäck J, et al, for the ARISTOTLE and RE-LY Electrical Stimulation in Spastic Muscles After Stroke: Systematic
Investigators. The novel biomarker-based ABC (age, biomarkers, Review and Meta-Analysis of Randomized Controlled Trials.
clinical history)-bleeding risk score for patients with atrial fibrillation: Stroke 2015; 46: 2197–205.
a derivation and validation study. Lancet 2016; 387: 2302–11. 133 Brady MC, Kelly H, Godwin J, Enderby P, Campbell P. Speech and
121 Kent DM, Dahabreh IJ, Ruthazer R, et al. Anticoagulant vs. language therapy for aphasia following stroke.
antiplatelet therapy in patients with cryptogenic stroke and patent Cochrane Database Syst Rev 2016; 6: CD000425.
foramen ovale: an individual participant data meta-analysis. 134 Elsner B, Kugler J, Pohl M, Mehrholz J. Transcranial direct current
Eur Heart J 2015; 36: 2381–89. stimulation (tDCS) for improving aphasia in patients with aphasia
122 Hebert D, Lindsay MP, McIntyre A, et al. Canadian stroke best after stroke. Cochrane Database Syst Rev 2015; 5: CD009760.
practice recommendations: Stroke rehabilitation practice 135 Loetscher T, Lincoln NB. Cognitive rehabilitation for attention
guidelines, update 2015. Int J Stroke 2016; 11: 459–84. deficits following stroke. Cochrane Database Syst Rev 2013;
123 Pollock A, Baer G, Campbell P, et al. Physical rehabilitation 5: CD002842.
approaches for the recovery of function and mobility following 136 Chung CS, Pollock A, Campbell T, Durward BR, Hagen S.
stroke. Cochrane Database Syst Rev 2014; 4: CD001920. Cognitive rehabilitation for executive dysfunction in adults with
124 Bernhardt J, Langhorne P, Lindley RI, et al, for the AVERT Trial stroke or other adult non-progressive acquired brain damage.
Collaboration group. Efficacy and safety of very early mobilisation Cochrane Database Syst Rev 2013; 4: CD008391.
within 24 h of stroke onset (AVERT): a randomised controlled trial. 137 Bowen A, Hazelton C, Pollock A, Lincoln NB. Cognitive
Lancet 2015; 386: 46–55. rehabilitation for spatial neglect following stroke.
125 Pollock A, Farmer SE, Brady MC, et al. Interventions for improving Cochrane Database Syst Rev 2013; 7: CD003586.
upper limb function after stroke. Cochrane Database Syst Rev 2014; 138 Wu S, Kutlubaev MA, Chun HY, et al. Interventions for post-stroke
11: CD010820. fatigue. Cochrane Database Syst Rev 2015; 7: CD007030.
126 Winstein CJ, Wolf SL, Dromerick AW. Effect of a task-orientated 139 Mead GE, Hsieh CF, Lee R, et al. Selective serotonin reuptake
rehabilitation program on upper extremity recovery following motor inhibitors (SSRIs) for stroke recovery. Cochrane Database Syst Rev
stroke. The ICARE randomised clinical trial. JAMA 2016; 2012; 11: CD009286.
315: 571–81. 140 Prasad K, Sharma A, Garg A, et al, for the InveST Study Group.
127 Mehrholz J, Pohl M, Platz T, Kugler J, Elsner B. Electromechanical Intravenous autologous bone marrow mononuclear stem cell
and robot-assisted arm training for improving activities of daily therapy for ischemic stroke: a multicentric, randomized trial.
living, arm function, and arm muscle strength after stroke. Stroke 2014; 45: 3618–24.
Cochrane Database Syst Rev 2015; 11: CD006876. 141 Kalladka D, Sinden J, Pollock K, et al. Human neural stem cells in
128 Saunders DH, Sanderson M, Brazzelli M, Greig CA, Mead GE. patients with chronic ischaemic stroke (PISCES): a phase 1,
Physical fitness training for stroke patients. first-in-man study. Lancet 2016; 388: 787–96.
Cochrane Database Syst Rev 2013; 10: CD003316. 142 Fearon P, Langhorne P, for the Early Supported Discharge Trialists.
129 Mehrholz J, Pohl M, Elsner B. Treadmill training and body weight Services for reducing duration of hospital care for acute stroke
support for walking after stroke. Cochrane Database Syst Rev 2014; patients. Cochrane Database Syst Rev 2012; 9: CD000443.
1: CD002840.
130 Bradt J, Magee WL, Dileo C, Wheeler BL, McGilloway E. Music
therapy for acquired brain injury. Cochrane Database Syst Rev 2010;
7: CD006787.
14 www.thelancet.com Published online September 13, 2016 http://dx.doi.org/10.1016/S0140-6736(16)30962-X
You might also like
- Management of Analgesia and Sedation in the Polytraumatized patientFrom EverandManagement of Analgesia and Sedation in the Polytraumatized patientNo ratings yet
- Secondary Fracture Prevention: An International PerspectiveFrom EverandSecondary Fracture Prevention: An International PerspectiveMarkus J. SeibelNo ratings yet
- CT in Acute Ischemic StrokeDocument0 pagesCT in Acute Ischemic StrokeLaurensia Erlina NataliaNo ratings yet
- Tuberculous Meningitis: Manual of Diagnosis and TherapyFrom EverandTuberculous Meningitis: Manual of Diagnosis and TherapyJerome ChinNo ratings yet
- Inflammatory and Autoimmune Disorders of the Nervous System in ChildrenFrom EverandInflammatory and Autoimmune Disorders of the Nervous System in ChildrenNo ratings yet
- Neuroimaging of Acute Ischemic StrokeDocument28 pagesNeuroimaging of Acute Ischemic StrokeLuisa Fda Castillo SalazarNo ratings yet
- Aicardi’s Diseases of the Nervous System in Childhood, 4th EditionFrom EverandAicardi’s Diseases of the Nervous System in Childhood, 4th EditionAlexis ArzimanoglouNo ratings yet
- Assessment of bleeding Shock in a Politraumatized PatientFrom EverandAssessment of bleeding Shock in a Politraumatized PatientNo ratings yet
- Etiology, Classification, and Epidemiology of StrokeDocument33 pagesEtiology, Classification, and Epidemiology of StrokeRenato VelitNo ratings yet
- Imaging in Acute Stroke FinallDocument73 pagesImaging in Acute Stroke FinallsriramNo ratings yet
- Brain Metastases from Primary Tumors, Volume 3: Epidemiology, Biology, and Therapy of Melanoma and Other CancersFrom EverandBrain Metastases from Primary Tumors, Volume 3: Epidemiology, Biology, and Therapy of Melanoma and Other CancersNo ratings yet
- 2015 Update AHA-ASA Early Acute Stroke Guidelines PDFDocument28 pages2015 Update AHA-ASA Early Acute Stroke Guidelines PDFIvan Yoseph SaputraNo ratings yet
- Interventional Neuroradiology A Complete Guide - 2020 EditionFrom EverandInterventional Neuroradiology A Complete Guide - 2020 EditionNo ratings yet
- Liquid Biopsy in Urogenital Cancers and its Clinical UtilityFrom EverandLiquid Biopsy in Urogenital Cancers and its Clinical UtilitySeyed Mohammad Kazem AghamirNo ratings yet
- Blood Transfusion Services in Sub Saharan Africa: Challenges and ConstraintsFrom EverandBlood Transfusion Services in Sub Saharan Africa: Challenges and ConstraintsNo ratings yet
- Abdominal Organ Transplantation: State of the ArtFrom EverandAbdominal Organ Transplantation: State of the ArtNizam MamodeNo ratings yet
- Cracking Chests: How Thoracic Surgery Got from Rocks to SticksFrom EverandCracking Chests: How Thoracic Surgery Got from Rocks to SticksNo ratings yet
- Major Incident Medical Management and Support: The Practical Approach at the SceneFrom EverandMajor Incident Medical Management and Support: The Practical Approach at the SceneNo ratings yet
- Advances in Cattle WelfareFrom EverandAdvances in Cattle WelfareCassandra TuckerNo ratings yet
- Comprehensive Overview of Modern Surgical Approaches to Intrinsic Brain TumorsFrom EverandComprehensive Overview of Modern Surgical Approaches to Intrinsic Brain TumorsKaisorn ChaichanaNo ratings yet
- Endovascular Treatment of Acute Ischemic Stroke.7 PDFDocument22 pagesEndovascular Treatment of Acute Ischemic Stroke.7 PDFchristinaNo ratings yet
- Consent Carotid StentingDocument13 pagesConsent Carotid StentingAbhinav GuptaNo ratings yet
- Cerebrovascular Ultrasound in Stroke Prevention and TreatmentFrom EverandCerebrovascular Ultrasound in Stroke Prevention and TreatmentRating: 5 out of 5 stars5/5 (1)
- Atlas of Hybrid Imaging Sectional Anatomy for PET/CT, PET/MRI and SPECT/CT Vol. 2: Thorax Abdomen and Pelvis: Sectional Anatomy for PET/CT, PET/MRI and SPECT/CTFrom EverandAtlas of Hybrid Imaging Sectional Anatomy for PET/CT, PET/MRI and SPECT/CT Vol. 2: Thorax Abdomen and Pelvis: Sectional Anatomy for PET/CT, PET/MRI and SPECT/CTNo ratings yet
- Vasculitis and NeuropathiesDocument14 pagesVasculitis and Neuropathiesjawad.melhem100% (1)
- Patent Foramen Ovale Closure for Stroke, Myocardial Infarction, Peripheral Embolism, Migraine, and HypoxemiaFrom EverandPatent Foramen Ovale Closure for Stroke, Myocardial Infarction, Peripheral Embolism, Migraine, and HypoxemiaM. Khalid MojadidiNo ratings yet
- Dual Antiplatelet Therapy for Coronary and Peripheral Arterial DiseaseFrom EverandDual Antiplatelet Therapy for Coronary and Peripheral Arterial DiseaseSorin BrenerNo ratings yet
- Anesthesia for Congenital Heart DiseaseFrom EverandAnesthesia for Congenital Heart DiseaseStephen A. StayerNo ratings yet
- Cerebral Dural Arteriovenous FistulasFrom EverandCerebral Dural Arteriovenous FistulasBradley A. GrossNo ratings yet
- CENTRAL RETINAL ARTERY OCCLUSION (CRAO) Final OphthalmologyDocument24 pagesCENTRAL RETINAL ARTERY OCCLUSION (CRAO) Final OphthalmologyAravind MahendranNo ratings yet
- Scrotal Wall LesionsDocument15 pagesScrotal Wall LesionsHarsha VijaykumarNo ratings yet
- Doppler SymeDocument12 pagesDoppler SymedoktoreluNo ratings yet
- Stroke and Its Imaging EvaluationDocument38 pagesStroke and Its Imaging EvaluationAnggi KusumawardaniNo ratings yet
- Neurovascular DisordersDocument42 pagesNeurovascular DisordersAlexandra Nedelcoff-GhiranlieffNo ratings yet
- 5 Evropske Preporuke Za Dijagnostiku I Lecenje AkutnogDocument53 pages5 Evropske Preporuke Za Dijagnostiku I Lecenje AkutnogvetvetNo ratings yet
- CT Brain Part II-AnatomyDocument65 pagesCT Brain Part II-AnatomyXhenni XhenniNo ratings yet
- Carotid Stenosis CriteriaDocument50 pagesCarotid Stenosis CriteriafiuliaNo ratings yet
- Infection: By: Dr. Abdullah NouhDocument5 pagesInfection: By: Dr. Abdullah NouhMajid Khan100% (1)
- Brain ImagingDocument56 pagesBrain ImagingAnant PachisiaNo ratings yet
- Clinical Neurology Answers OnlyDocument68 pagesClinical Neurology Answers Onlyanas kNo ratings yet
- Main Stroke Protocol - Use For All Suspected Stroke-TIA PatientsDocument2 pagesMain Stroke Protocol - Use For All Suspected Stroke-TIA PatientsRivulet1No ratings yet
- Misra U, Kalita J Dan Dubey D. A Study of Super Refractory Status Epilepticus From IndiaDocument10 pagesMisra U, Kalita J Dan Dubey D. A Study of Super Refractory Status Epilepticus From IndiasitialimahNo ratings yet
- An Overview of Autoimmune and Paraneoplastic EncefaliteDocument14 pagesAn Overview of Autoimmune and Paraneoplastic Encefaliterafael rocha novaesNo ratings yet
- Peripheral NeuropathyDocument8 pagesPeripheral NeuropathyJessica Alejandra Razo100% (1)
- Electrographic and Electroclinical Seizures BirdsDocument50 pagesElectrographic and Electroclinical Seizures BirdsNEUROMED NEURONo ratings yet
- Prepared By: Ulfat Amin MSC Pediatric NursingDocument25 pagesPrepared By: Ulfat Amin MSC Pediatric NursingAngelic khanNo ratings yet
- Indicators of DifficultyDocument2 pagesIndicators of DifficultyJose Angelo Soler NateNo ratings yet
- Daftar Diagnosa Penyakit Beserta Kode Icd 10Document1 pageDaftar Diagnosa Penyakit Beserta Kode Icd 10suci fauziNo ratings yet
- Heat Illnes Ped Rev 2019Document13 pagesHeat Illnes Ped Rev 2019Sandra A. Sánchez GarcíaNo ratings yet
- Diagnosis and Management of Glutaric Aciduria Type I - Revised RecommendationsDocument18 pagesDiagnosis and Management of Glutaric Aciduria Type I - Revised RecommendationsMoroianu Irina-GabrielaNo ratings yet
- Management of Facial Fractures1Document279 pagesManagement of Facial Fractures1مهند الوادعيNo ratings yet
- Reflection #2Document16 pagesReflection #2Stephanie MckeeNo ratings yet
- Comprehensive Review Of Infectious Diseases 1St Edition Andrej Spec full chapter pdf docxDocument69 pagesComprehensive Review Of Infectious Diseases 1St Edition Andrej Spec full chapter pdf docxjeydeltaive100% (5)
- Collecting Subjective Data: Health AssessmentDocument83 pagesCollecting Subjective Data: Health AssessmentChriscell Gipanao Eustaquio100% (1)
- Sahaja Yoga Meditation PresentationDocument37 pagesSahaja Yoga Meditation Presentationpoonamt2001100% (5)
- Jenny LeafletDocument2 pagesJenny Leafletجني رمضانNo ratings yet
- Walter Modell M. D., F.A.C.P., Doris J. Place R. N. (Auth.) - The Use of Drugs - Principles of Pharmacology and Therapeutics For Nurses (1957, Springer-Verlag Berlin Heidelberg) PDFDocument350 pagesWalter Modell M. D., F.A.C.P., Doris J. Place R. N. (Auth.) - The Use of Drugs - Principles of Pharmacology and Therapeutics For Nurses (1957, Springer-Verlag Berlin Heidelberg) PDFbluegreenalgaNo ratings yet
- CuminDocument4 pagesCuminDr. Anjali RaoNo ratings yet
- A Case of DepressionDocument11 pagesA Case of DepressionKabilan R100% (2)
- Causes of Acute Abdominal Pain in Children and Adolescents - UpToDateDocument25 pagesCauses of Acute Abdominal Pain in Children and Adolescents - UpToDateლელა ნიშნიანიძეNo ratings yet
- DATA SENSUS - POLIKLINIK UMUM - 02 Januari 2019 00 - 00 - 02 Januari 2019 23 - 59Document35 pagesDATA SENSUS - POLIKLINIK UMUM - 02 Januari 2019 00 - 00 - 02 Januari 2019 23 - 59jarotNo ratings yet
- Medical Microbiology and Immunology Flash Cards - Sample ChapterDocument250 pagesMedical Microbiology and Immunology Flash Cards - Sample Chapterleh.mo931580% (5)
- Drug Description: Reductions in Risk of CHD Mortality and Cardiovascular EventsDocument9 pagesDrug Description: Reductions in Risk of CHD Mortality and Cardiovascular EventsCARINAMHNo ratings yet
- Shock Pathophysiology and ManagementDocument27 pagesShock Pathophysiology and ManagementAadal NayyarNo ratings yet
- Magnitude of Maternal and Child Health Problems: Qudrat Un Nissa MSC Nursing OBGDocument71 pagesMagnitude of Maternal and Child Health Problems: Qudrat Un Nissa MSC Nursing OBGQudrat Un Nissa100% (2)
- Date Assessment Nursing Diagnosis Background Knowledge Planning Intervention Rationale Evaluation Objective SubjectiveDocument2 pagesDate Assessment Nursing Diagnosis Background Knowledge Planning Intervention Rationale Evaluation Objective SubjectivePauline CañoNo ratings yet
- Grave DiseaseDocument6 pagesGrave DiseaseFakrocev Charlie GuloNo ratings yet
- What Are The KidneysDocument4 pagesWhat Are The KidneysKathiresan KathirNo ratings yet
- SABER-Nursing Care Plan #1 - JGDocument7 pagesSABER-Nursing Care Plan #1 - JGJessica MontoyaNo ratings yet
- Masten Ordinary MagicDocument20 pagesMasten Ordinary MagicgrechianNo ratings yet
- Herbal Meds. Bayabas and Niyug NoyoganDocument5 pagesHerbal Meds. Bayabas and Niyug NoyoganJames Edward CalmaNo ratings yet
- MeningitisDocument1 pageMeningitisKRCG 13No ratings yet
- Chapter 3 - Diagnosis - 2002 - Contemporary Chinese Medicine and AcupunctureDocument18 pagesChapter 3 - Diagnosis - 2002 - Contemporary Chinese Medicine and Acupuncturetian xuNo ratings yet
- Communicable & Non-Communicable Disease: CreatedbyDocument17 pagesCommunicable & Non-Communicable Disease: CreatedbyRATNA NOVITANo ratings yet
- Texila American University: Case Report FormatDocument7 pagesTexila American University: Case Report FormatShahzad AhmadNo ratings yet