You might also like
- Ideal Inpatient Progress Notes Template of Ideal Progress NoteDocument2 pagesIdeal Inpatient Progress Notes Template of Ideal Progress Notebrianzfl100% (1)
- Opeman MIDTERM 2Document2 pagesOpeman MIDTERM 2Michelle Ann WongNo ratings yet
- Running Head: NURSING STANDARDS 1Document20 pagesRunning Head: NURSING STANDARDS 1api-253509573No ratings yet
- Studentassessmentfinal 208Document14 pagesStudentassessmentfinal 208api-305752422No ratings yet
- Patient Flow at Brigham and Women's Hospital Written CaseDocument5 pagesPatient Flow at Brigham and Women's Hospital Written CaseAlimKassymovNo ratings yet
- PHN Bag TechniqueDocument4 pagesPHN Bag TechniquekirbyroohNo ratings yet
- 2nd Semester Reflective JournalsDocument12 pages2nd Semester Reflective Journalsapi-248017509No ratings yet
- Scholarly EssayDocument7 pagesScholarly Essayapi-284041802No ratings yet
- Improving Pressure Ulcer ScreeningDocument5 pagesImproving Pressure Ulcer ScreeningJonathan BieniekNo ratings yet
- BioethicsDocument3 pagesBioethicspaui16No ratings yet
- Registered Nurse Resume SampleDocument1 pageRegistered Nurse Resume SampleAlen Augustine100% (1)
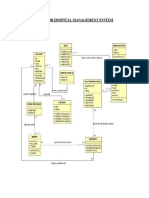
- Uml Diagrams For Hospital Management SystemDocument9 pagesUml Diagrams For Hospital Management Systemjitendra jha100% (1)
- Midpoint Reflection Journal ImmersionDocument3 pagesMidpoint Reflection Journal Immersionapi-433144546No ratings yet
- Ppg-Gdch-Nur-43 Out On Pass PolicyDocument5 pagesPpg-Gdch-Nur-43 Out On Pass PolicyKenny Josef100% (1)
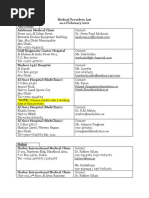
- MetLife Medical Providers List As of 20 Feb 2021 PDFDocument7 pagesMetLife Medical Providers List As of 20 Feb 2021 PDFherra husainNo ratings yet
- Running Head: Reflection in Nursing 1Document21 pagesRunning Head: Reflection in Nursing 1joseeNo ratings yet
- Chengalpet District Healthcare FacilitiesDocument975 pagesChengalpet District Healthcare FacilitiesAshraf Ahmed.B100% (1)
- Clinical Nursing JudgmentDocument5 pagesClinical Nursing Judgmentapi-508051902No ratings yet
- Nurs 208 Final EvaluationDocument11 pagesNurs 208 Final Evaluationapi-351047631No ratings yet
- My Capstone Project Reflection PaperDocument10 pagesMy Capstone Project Reflection Paperapi-223286633100% (1)
- Nur403 IntropagesummaryprojectDocument6 pagesNur403 Intropagesummaryprojectapi-529373199No ratings yet
- Clinical Nursing JudgementDocument7 pagesClinical Nursing Judgementapi-453417498No ratings yet
- Professionaldevelopmentplan ShefferDocument17 pagesProfessionaldevelopmentplan Shefferapi-235387260No ratings yet
- capstone paper 1Document6 pagescapstone paper 1api-732900066No ratings yet
- Self Debriefing Questions - Vsim Week 5Document3 pagesSelf Debriefing Questions - Vsim Week 5api-631170779No ratings yet
- Umhafer Ethics PaperDocument6 pagesUmhafer Ethics Paperapi-444947174No ratings yet
- Weekly Self Evaluation Ms 6Document2 pagesWeekly Self Evaluation Ms 6api-316491996No ratings yet
- Clinical Nursing Judgement Paper - Emily HakesDocument7 pagesClinical Nursing Judgement Paper - Emily Hakesapi-545031607No ratings yet
- clinical nursing judgment paper 1Document5 pagesclinical nursing judgment paper 1api-740431489No ratings yet
- RiverspdpDocument15 pagesRiverspdpapi-241413796No ratings yet
- Relationshipbasedcarepaper - NSG 4040-1Document13 pagesRelationshipbasedcarepaper - NSG 4040-1api-314231356No ratings yet
- Assignment 1Document2 pagesAssignment 1Ella B. CollantesNo ratings yet
- 1000words 044811Document2 pages1000words 044811Joshua AladenikaNo ratings yet
- Madeline Foran - Project NarrativeDocument3 pagesMadeline Foran - Project Narrativeapi-519051717No ratings yet
- Practice Summary Paper 1Document7 pagesPractice Summary Paper 1api-593090065No ratings yet
- Hart Mariah Finalpractice Summary Paper 1Document14 pagesHart Mariah Finalpractice Summary Paper 1api-655030354No ratings yet
- Professional Progress SummaryDocument16 pagesProfessional Progress Summaryapi-272878167No ratings yet
- Evaluating Current Practice Patti Graded 1Document6 pagesEvaluating Current Practice Patti Graded 1api-240095350No ratings yet
- Clinical Nursing Judgement Paper CapstoneDocument6 pagesClinical Nursing Judgement Paper Capstoneapi-663065092No ratings yet
- Advocacy in Nursing: Promoting Patient-Centered CareDocument6 pagesAdvocacy in Nursing: Promoting Patient-Centered CareShadow RazeNo ratings yet
- Running Head: Practice Summary Paper 1Document8 pagesRunning Head: Practice Summary Paper 1api-257720093No ratings yet
- Test Bank For Medical Surgical Nursing Preparation For Practice 1st Edition OsbornDocument18 pagesTest Bank For Medical Surgical Nursing Preparation For Practice 1st Edition OsbornMaryJohnsonafrz100% (39)
- Clinical Nursing JudgmentDocument6 pagesClinical Nursing Judgmentapi-662892413No ratings yet
- Capstone PaperDocument6 pagesCapstone Paperapi-455623284No ratings yet
- Senior Capstone Scholarly PaperDocument5 pagesSenior Capstone Scholarly Paperapi-663499263No ratings yet
- Nur 460 Practicum DocumentationsDocument9 pagesNur 460 Practicum Documentationsapi-597634889No ratings yet
- Professional Development PlanDocument19 pagesProfessional Development Planapi-242114301No ratings yet
- Tajuddin Wound Care Reflection PaperDocument4 pagesTajuddin Wound Care Reflection Paperapi-465165917No ratings yet
- C489 Task1 CompletedDocument4 pagesC489 Task1 CompletedSteven SteveNo ratings yet
- Nur403 Intropage2Document4 pagesNur403 Intropage2api-529373199No ratings yet
- adult health reflective journalDocument11 pagesadult health reflective journalapi-721737905No ratings yet
- final draft reflection paperDocument8 pagesfinal draft reflection paperapi-679429352No ratings yet
- Ritchey Nurs660 ReflectionpaperDocument7 pagesRitchey Nurs660 Reflectionpaperapi-284230154No ratings yet
- Weekly Eval April 6thDocument4 pagesWeekly Eval April 6thapi-253711614No ratings yet
- Learning Activities - Docx FinaleDocument8 pagesLearning Activities - Docx FinaleKrisia CastucianoNo ratings yet
- And Utilization of Nursing ResourcesDocument10 pagesAnd Utilization of Nursing ResourcesSimran ChauhanNo ratings yet
- Final Reflection DkropaczekDocument3 pagesFinal Reflection Dkropaczekapi-294937204No ratings yet
- Nurs 151 Final EvaluationDocument11 pagesNurs 151 Final Evaluationapi-351047631No ratings yet
- Scholarly Paper - CapstoneDocument6 pagesScholarly Paper - Capstoneapi-736949349No ratings yet
- Recomendation Report-MurdockDocument10 pagesRecomendation Report-Murdockapi-340998643No ratings yet
- Teaching Project Summary PaperDocument11 pagesTeaching Project Summary Paperapi-630699625No ratings yet
- Intro Page - Practice Summary PaperDocument4 pagesIntro Page - Practice Summary Paperapi-467110214No ratings yet
- Assignment 1Document4 pagesAssignment 1Ochieng BrianNo ratings yet
- Theory Application PaperDocument13 pagesTheory Application Paperapi-295425485No ratings yet
- Clinical Nursing Judgement Scholarly PaperDocument5 pagesClinical Nursing Judgement Scholarly Paperapi-663561390No ratings yet
- Nur 460 PGC Reflection PaperDocument14 pagesNur 460 PGC Reflection Paperapi-598192448No ratings yet
- Running Head: Quality Improvement Project 1Document9 pagesRunning Head: Quality Improvement Project 1api-379379776No ratings yet
- Observerships InsiderDocument5 pagesObserverships InsiderRaja Shakeel Mushtaque, M.D.100% (2)
- Digital Poster Qi ProjectDocument1 pageDigital Poster Qi Projectapi-447860598No ratings yet
- AdvertisingactivityDocument5 pagesAdvertisingactivityapi-447860598No ratings yet
- Strengths and Leadership Gallup ResultsDocument4 pagesStrengths and Leadership Gallup Resultsapi-447860598No ratings yet
- Zero Based BudgetDocument9 pagesZero Based Budgetapi-447860598No ratings yet
- Running Head: Integrative Literature Review 1Document22 pagesRunning Head: Integrative Literature Review 1api-447860598No ratings yet
- Final Summary Nur 4242Document9 pagesFinal Summary Nur 4242api-447860598No ratings yet
- Running Head: ROOT CAUSE ANALYSIS 1Document8 pagesRunning Head: ROOT CAUSE ANALYSIS 1api-447860598No ratings yet
- Genomics Literacy ProjectDocument14 pagesGenomics Literacy Projectapi-447860598No ratings yet
- Strengthsbasedleadership FinalDocument5 pagesStrengthsbasedleadership Finalapi-447860598No ratings yet
- Nur 4242 Practicum Log 1Document2 pagesNur 4242 Practicum Log 1api-447860598No ratings yet
- IpmsDocument2 pagesIpmsmutu_bunutNo ratings yet
- Breast SpanishDocument236 pagesBreast Spanishelmer.cespedesNo ratings yet
- 2022 07 30NewZealandListenerDocument96 pages2022 07 30NewZealandListenerLuhur KurniantoNo ratings yet
- Assignment Building SystemDocument5 pagesAssignment Building SystemMohd MezlanNo ratings yet
- PCR Testing Centers in The PhilippinesDocument36 pagesPCR Testing Centers in The Philippineskhrayzie bhoneNo ratings yet
- Medical Records: By: Alvin Apriliani 11170004Document11 pagesMedical Records: By: Alvin Apriliani 11170004Alvin aprilianiNo ratings yet
- S.K Patil Hospital: (Municipal Hospital) Live Case StudyDocument6 pagesS.K Patil Hospital: (Municipal Hospital) Live Case StudyAnkit VarmaNo ratings yet
- Equipment Registration FormDocument1 pageEquipment Registration Formjim tauNo ratings yet
- GOING TO THE DOCTOR (Body and Health) : VocabularyDocument2 pagesGOING TO THE DOCTOR (Body and Health) : VocabularyDiana CuleaNo ratings yet
- SPEAKING ROLE PLAY Oet TapescriptDocument6 pagesSPEAKING ROLE PLAY Oet Tapescriptranbirsingh1796No ratings yet
- (B-0155) Ambulatory Care UnitDocument22 pages(B-0155) Ambulatory Care UnitAhmad Gamal Elden MAhanyNo ratings yet
- Mercy Health Case Study Dramatically Reduces ED Wait TimesDocument1 pageMercy Health Case Study Dramatically Reduces ED Wait TimesStacey SalvillaNo ratings yet
- Seat Matrix JENPAS (UG) - 2021Document4 pagesSeat Matrix JENPAS (UG) - 2021Kundan JhaNo ratings yet
- Hospital Cash Treating Doctors CertificateDocument1 pageHospital Cash Treating Doctors Certificatesmallik3No ratings yet
- Hill-Rom Evolution Bed - User Manual PDFDocument60 pagesHill-Rom Evolution Bed - User Manual PDFJulian NovoaNo ratings yet
- Empanelled Hospital Under BSKY-V12Document4 pagesEmpanelled Hospital Under BSKY-V12Bhabanath Sahu LuckyNo ratings yet
- Database Management SystemDocument4 pagesDatabase Management SystemOwen LuzNo ratings yet
- History of Developmrnt of Nursing ProfessionDocument10 pagesHistory of Developmrnt of Nursing ProfessionHanison MelwynNo ratings yet
- PR TanzeemaDocument33 pagesPR Tanzeemazobaida13No ratings yet
- UNIT 4 Personal HygieneDocument24 pagesUNIT 4 Personal HygieneAshaNo ratings yet
- Accreditation and Certification 10 09Document2 pagesAccreditation and Certification 10 09Snegha RajaNo ratings yet