You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5819)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Unseen Side of Pregnancy: Non-Communicable Diseases and Maternal HealthDocument28 pagesThe Unseen Side of Pregnancy: Non-Communicable Diseases and Maternal HealthThe Wilson Center100% (2)
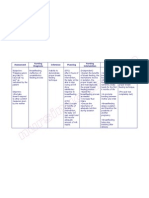
- Nursing Care Plan Breast Feeding IneffectiveDocument1 pageNursing Care Plan Breast Feeding Ineffectivederic88% (8)
- June 2012 (v3) QP - Paper 3 CIE Biology IGCSE PDFDocument24 pagesJune 2012 (v3) QP - Paper 3 CIE Biology IGCSE PDFAli AshrafNo ratings yet
- Reproduction (Multiple Choice) 1 QP PDFDocument20 pagesReproduction (Multiple Choice) 1 QP PDFCollins JimNo ratings yet
- Polycystic Ovarian Syndrome: Anna Lissa J. Bernadas, M.D., F.P.O.G.SDocument39 pagesPolycystic Ovarian Syndrome: Anna Lissa J. Bernadas, M.D., F.P.O.G.SJerahmeel Sombilon GenillaNo ratings yet
- ACOBA BiblioDocument2 pagesACOBA BiblioOliver Cortes AcobaNo ratings yet
- FM - TBC NCM 108 ModuleDocument23 pagesFM - TBC NCM 108 ModuleJoy B. DaladagNo ratings yet
- Mohammed AwelDocument63 pagesMohammed Awelnasru hajiNo ratings yet
- Codorniz Joshua Isaiah M. BSCS3A Learning Output 6Document1 pageCodorniz Joshua Isaiah M. BSCS3A Learning Output 6Joshua CodornizNo ratings yet
- 3 Shub Niggurath, The Empress (Lib - Wildla.in)Document14 pages3 Shub Niggurath, The Empress (Lib - Wildla.in)KLKTZNo ratings yet
- Surrogacy Regulation Act 2021 Central38408com420450Document20 pagesSurrogacy Regulation Act 2021 Central38408com420450Ayushman DubeyNo ratings yet
- Chlamydia Gonorrhea Treatment ChartDocument1 pageChlamydia Gonorrhea Treatment ChartdoodrillNo ratings yet
- From PMS To MenopauseDocument196 pagesFrom PMS To MenopauseWeemizo تNo ratings yet
- 11.4 Sexual ReproductionDocument29 pages11.4 Sexual ReproductionteddyenNo ratings yet
- Care of Mother, Child, Adolescent: GoalsDocument8 pagesCare of Mother, Child, Adolescent: GoalschelseyNo ratings yet
- Objective Structured Clinical Examination On PartographDocument58 pagesObjective Structured Clinical Examination On PartographMd AliNo ratings yet
- Antenatal Complications Acute ChronicDocument10 pagesAntenatal Complications Acute ChronicJennie KimNo ratings yet
- Case Study - Piramal Swasthya - v2.0Document10 pagesCase Study - Piramal Swasthya - v2.0Vivek Rana100% (1)
- The Istanbul Consensus Workshop On Embryo Assessment: Proceedings of An Expert MeetingDocument13 pagesThe Istanbul Consensus Workshop On Embryo Assessment: Proceedings of An Expert MeetingchristopherNo ratings yet
- OB GYN Mock Board QuestionnaireDocument12 pagesOB GYN Mock Board QuestionnairejampogaottNo ratings yet
- Case Scenario Drug Study - VicenteDocument4 pagesCase Scenario Drug Study - VicenteLouraine VicenteNo ratings yet
- VulvaDocument35 pagesVulvaKu NiniNo ratings yet
- Child Development From Infancy To Adolescence An Active Learning Approach 1St Edition Levine Test Bank Full Chapter PDFDocument36 pagesChild Development From Infancy To Adolescence An Active Learning Approach 1St Edition Levine Test Bank Full Chapter PDFmatthew.templeton879100% (13)
- Historical Perspectiv Obg Nursing PDF Midwifery MidwifeDocument1 pageHistorical Perspectiv Obg Nursing PDF Midwifery MidwifeEsther Opoku AfosaahNo ratings yet
- BHC LT1 Ncm107ceDocument2 pagesBHC LT1 Ncm107ceLeah Reese VersonNo ratings yet
- Summary of Product Characteristics: Rowachol CapsulesDocument3 pagesSummary of Product Characteristics: Rowachol CapsulesasdwasdNo ratings yet
- Zainab ProjectDocument35 pagesZainab ProjectOpeyemi JamalNo ratings yet
- Atlas of Obstetric UltrasoundDocument48 pagesAtlas of Obstetric UltrasoundSanchia Theresa100% (1)
- Pregnancy Nutrition - QUIZDocument4 pagesPregnancy Nutrition - QUIZriann leigh TrangiaNo ratings yet
- Chemical Coordination and Integration by - Dr. Sunita SaxenaDocument66 pagesChemical Coordination and Integration by - Dr. Sunita SaxenaDivya AgarawalNo ratings yet