You might also like
- Inflammation and RepairDocument5 pagesInflammation and RepairDENILLE AIRA NOGOYNo ratings yet
- Detoxing Secrets For Vibrant Health TTAC QFTCDocument26 pagesDetoxing Secrets For Vibrant Health TTAC QFTCNikola RatkovićNo ratings yet
- Chapter 42 - Sepsis, Septic Shock, and Multiple Organ FailureDocument15 pagesChapter 42 - Sepsis, Septic Shock, and Multiple Organ FailureWorrawalun FuktongNo ratings yet
- Gusto Magazine - Issue 5Document8 pagesGusto Magazine - Issue 5Gusto MagazineNo ratings yet
- Chlorine Dioxide in Covid19 Mechanism of Molecular Action in Sarscov2Document8 pagesChlorine Dioxide in Covid19 Mechanism of Molecular Action in Sarscov2mauricio lopezNo ratings yet
- Lesson: Dr. Leon Hammer, M.DDocument14 pagesLesson: Dr. Leon Hammer, M.DRocío JMNo ratings yet
- Raya Pharmaceuticals Co. LTD: Cataflam®Document8 pagesRaya Pharmaceuticals Co. LTD: Cataflam®Mayson BaliNo ratings yet
- NCP - PainDocument3 pagesNCP - PainAdrian Mallar100% (2)
- Acidified Sodium Chlorite Solution A Potential Prophylaxis To Mitigate Impact of Multiple Exposures To COVID 19 in Frontline Health Care ProvidersDocument5 pagesAcidified Sodium Chlorite Solution A Potential Prophylaxis To Mitigate Impact of Multiple Exposures To COVID 19 in Frontline Health Care ProvidersGerardo de Gyves AvilaNo ratings yet
- Redox Biology: SciencedirectDocument13 pagesRedox Biology: SciencedirectLin LINo ratings yet
- Journal Pre-Proof: International Journal of Antimicrobial AgentsDocument32 pagesJournal Pre-Proof: International Journal of Antimicrobial AgentsAngel de Jesus Lugo ZazuetaNo ratings yet
- Nasal Irrigation Clo2Document4 pagesNasal Irrigation Clo2Candela VidalNo ratings yet
- Bio Zone Cold Oxygen Plasma TechDocument6 pagesBio Zone Cold Oxygen Plasma TechcklaiNo ratings yet
- Presentation CovidDocument22 pagesPresentation Covidmiddleclassboy62No ratings yet
- Effect of Sodium Bicarbonate 8.4% On Respiratory Tract PathogensDocument5 pagesEffect of Sodium Bicarbonate 8.4% On Respiratory Tract PathogensKiran DangolNo ratings yet
- Tian 2012Document10 pagesTian 2012Clovis Moreira JrNo ratings yet
- MikropartikelDocument9 pagesMikropartikelRirin AptNo ratings yet
- 2017 Fosfato de CalcioDocument9 pages2017 Fosfato de CalcioAngy ÑacatoNo ratings yet
- TMP 4 EF7Document11 pagesTMP 4 EF7FrontiersNo ratings yet
- Research ArticleDocument19 pagesResearch Articleshrooq sweilamNo ratings yet
- Read Discussion 27hydroxycholesterol Inhibit SARS-Cov-2 and Is Reduced in COVID-19 PatientsDocument11 pagesRead Discussion 27hydroxycholesterol Inhibit SARS-Cov-2 and Is Reduced in COVID-19 PatientsAhmedNo ratings yet
- Research in MicrobiologyDocument3 pagesResearch in MicrobiologyJeanny ANo ratings yet
- Bpoc Studiu 3Document7 pagesBpoc Studiu 3Claudia SofroniaNo ratings yet
- Aspergillus Jurnal EnglishDocument5 pagesAspergillus Jurnal EnglishSyafiraNo ratings yet
- Effects of Whole Cigarette Smoke On Human Beta Defensins Expression and Secretion by Oral Mucosal Epithelial CellsDocument10 pagesEffects of Whole Cigarette Smoke On Human Beta Defensins Expression and Secretion by Oral Mucosal Epithelial CellsMirela TomaNo ratings yet
- N.K. Oliveira Et Al. 2021Document9 pagesN.K. Oliveira Et Al. 2021Fabian DavidNo ratings yet
- Lock Therapy CandidaDocument8 pagesLock Therapy CandidaMarcos StivanelloNo ratings yet
- Kadota 2024 JVMS ClO2 Liquid Gas Virucide Avian Flu Infect BronchitisDocument7 pagesKadota 2024 JVMS ClO2 Liquid Gas Virucide Avian Flu Infect BronchitisstflockNo ratings yet
- Al-Akidi Therapeutic Protocol For Severe Infections Associated With Covid-19: Potential and Effective Treatment by Levofloxacin and Vitamin D3 and Zinc (Part 1)Document14 pagesAl-Akidi Therapeutic Protocol For Severe Infections Associated With Covid-19: Potential and Effective Treatment by Levofloxacin and Vitamin D3 and Zinc (Part 1)Sabrina JonesNo ratings yet
- New Insights On The Antiviral Effects of Chloroquine Against Coronavirus What To Expect For COVID19 PDFDocument32 pagesNew Insights On The Antiviral Effects of Chloroquine Against Coronavirus What To Expect For COVID19 PDFHendry HuangNo ratings yet
- New Insights On The Antiviral Effects of Chloroquine Against Coronavirus What To Expect For Covid 19 Christian A Devaux Full ChapterDocument29 pagesNew Insights On The Antiviral Effects of Chloroquine Against Coronavirus What To Expect For Covid 19 Christian A Devaux Full Chapternorman.pregler293100% (10)
- Acetic Acid Disinfection As A Potential Adjunctive Therapy For Non Severe COVID 19Document4 pagesAcetic Acid Disinfection As A Potential Adjunctive Therapy For Non Severe COVID 19Intan AyuNo ratings yet
- Communication: Multidrug Treatment For COVID-19Document3 pagesCommunication: Multidrug Treatment For COVID-19احمد عرفاتNo ratings yet
- Medical Hypotheses: SciencedirectDocument4 pagesMedical Hypotheses: SciencedirectDaniel ChávezNo ratings yet
- A Systematic Review On Effects of Chloroquine As A Antiviral Against Covid-19Document7 pagesA Systematic Review On Effects of Chloroquine As A Antiviral Against Covid-19International Journal of Innovative Science and Research TechnologyNo ratings yet
- Ebook New Insights On The Antiviral Effects of Chloroquine Against Coronavirus What To Expect For Covid 19 PDF Full Chapter PDFDocument28 pagesEbook New Insights On The Antiviral Effects of Chloroquine Against Coronavirus What To Expect For Covid 19 PDF Full Chapter PDFglenn.mcdonald396100% (19)
- động học quá trình xử lý kháng sinh bằng plasma lạnhDocument15 pagesđộng học quá trình xử lý kháng sinh bằng plasma lạnhkhoaanhletranNo ratings yet
- Are Promising Mechanisms of Hydroxychloroquine Abolish COVID-19 Activity? A Review StudyDocument5 pagesAre Promising Mechanisms of Hydroxychloroquine Abolish COVID-19 Activity? A Review StudyAbdulsalamNo ratings yet
- New Microsoft Word DocumentDocument3 pagesNew Microsoft Word DocumentSWETHA V SNo ratings yet
- 3 RDDocument8 pages3 RDFatmaNo ratings yet
- Antimicribial Activity of Chlorhexidine and BKCDocument11 pagesAntimicribial Activity of Chlorhexidine and BKCm_barrueta_No ratings yet
- BJMP 2012 5 1 A512Document5 pagesBJMP 2012 5 1 A512maslikanNo ratings yet
- Covid 01 00037 v2Document12 pagesCovid 01 00037 v2WestwickateNo ratings yet
- Comparative Study of Levofloxacin and Amoxycillin/clavulanic Acid in Adults With Mild-To-Moderate Community-AcquiredDocument9 pagesComparative Study of Levofloxacin and Amoxycillin/clavulanic Acid in Adults With Mild-To-Moderate Community-Acquiredjuloc34No ratings yet
- 1 s2.0 S1011134422000288 MainDocument8 pages1 s2.0 S1011134422000288 MainLucas S. CostaNo ratings yet
- Jurnal 3Document7 pagesJurnal 3Fida NadhirNo ratings yet
- Clinmed 2020-0351 FullDocument4 pagesClinmed 2020-0351 FullIsro AlhaqiNo ratings yet
- Candidiase Cold AtmosphericDocument20 pagesCandidiase Cold AtmosphericIvan Alves de SouzaNo ratings yet
- Bioorganic & Medicinal Chemistry: Article InfoDocument8 pagesBioorganic & Medicinal Chemistry: Article InfoLeo RuilovaNo ratings yet
- Carbon Trends: Joydip Sengupta, Chaudhery Mustansar HussainDocument4 pagesCarbon Trends: Joydip Sengupta, Chaudhery Mustansar HussainOussama ZeggaiNo ratings yet
- 10 1016@j Ijantimicag 2020 105923Document6 pages10 1016@j Ijantimicag 2020 105923Basilio Papuico RomeroNo ratings yet
- Analysis of The Anti-Viral Potential of Nasal Spray Constituents AgainstDocument16 pagesAnalysis of The Anti-Viral Potential of Nasal Spray Constituents AgainstLes BennettNo ratings yet
- Advances in Pulmonary Drug Delivery: PharmaceuticsDocument7 pagesAdvances in Pulmonary Drug Delivery: PharmaceuticsSamra KhanNo ratings yet
- Artif Cell 24515303Document11 pagesArtif Cell 24515303István PortörőNo ratings yet
- Him Smoke 2Document8 pagesHim Smoke 2Ives GerardoNo ratings yet
- Original Research: COVID-19 Global Pandemic Planning: Decontamination and Reuse Processes For N95 RespiratorsDocument7 pagesOriginal Research: COVID-19 Global Pandemic Planning: Decontamination and Reuse Processes For N95 RespiratorscrisNo ratings yet
- Antiviral GasesDocument37 pagesAntiviral Gasesdrdgrant6055No ratings yet
- Efficacy Octenidine Vs OthersDocument8 pagesEfficacy Octenidine Vs OthersSanti utamiNo ratings yet
- Candida Albicans Biofilm InhibitorsDocument7 pagesCandida Albicans Biofilm InhibitorsSenuke TestNo ratings yet
- Does Zinc Supplementation Enhance The Clinical Efficacy of CHL 2020 MedicalDocument3 pagesDoes Zinc Supplementation Enhance The Clinical Efficacy of CHL 2020 MedicalzarNo ratings yet
- Standardized Comparison of Antiseptic Efficacy ofDocument9 pagesStandardized Comparison of Antiseptic Efficacy ofAnamaria Catalina LeuNo ratings yet
- Vitamin D Deficiency Predicts 30 Day Hospital MortDocument4 pagesVitamin D Deficiency Predicts 30 Day Hospital MortJose VasquezNo ratings yet
- Klaus Jungeblut - 1939 - Vitamin C Poliomyelitis Report ExperimentDocument19 pagesKlaus Jungeblut - 1939 - Vitamin C Poliomyelitis Report ExperimentLuc LiebecqNo ratings yet
- Immune Evasion of Leptospira Species byDocument8 pagesImmune Evasion of Leptospira Species byAnderson SantosNo ratings yet
- Molecular Oral Microbiology - 2023 - D Amico - Efficacy of Cetylpyridinium Chloride Mouthwash Against SARS CoV 2 ADocument10 pagesMolecular Oral Microbiology - 2023 - D Amico - Efficacy of Cetylpyridinium Chloride Mouthwash Against SARS CoV 2 Akatcharles.persoNo ratings yet
- International Journal of PharmaceuticsDocument7 pagesInternational Journal of PharmaceuticsYaninaDeLafuenteNo ratings yet
- Advancing Early Childhood Development: From Science To Scale 3Document16 pagesAdvancing Early Childhood Development: From Science To Scale 3Mayson BaliNo ratings yet
- Compression Parameters Start UpDocument1 pageCompression Parameters Start UpMayson BaliNo ratings yet
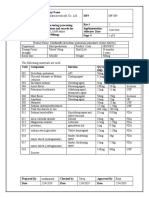
- Sample MFRDocument22 pagesSample MFRMayson BaliNo ratings yet
- You Sent Today at 5:11 AMDocument3 pagesYou Sent Today at 5:11 AMMayson BaliNo ratings yet
- Over-The-Counter Drug Abuse and Misuse in PalestineDocument2 pagesOver-The-Counter Drug Abuse and Misuse in PalestineMayson BaliNo ratings yet
- Communication Important in Medical Labrotory WorkersDocument4 pagesCommunication Important in Medical Labrotory WorkersMayson BaliNo ratings yet
- The Social Determinants of Health: It's Time To Consider The Causes of The CausesDocument13 pagesThe Social Determinants of Health: It's Time To Consider The Causes of The CausesMayson BaliNo ratings yet
- Over-The-Counter Drug Abuse and Misuse in PalestineDocument3 pagesOver-The-Counter Drug Abuse and Misuse in PalestineMayson BaliNo ratings yet
- Structural and Social Determinants of Early Childhood DevelopmentDocument10 pagesStructural and Social Determinants of Early Childhood DevelopmentMayson BaliNo ratings yet
- Structural and Social Determinants of Early Childhood DevelopmentDocument11 pagesStructural and Social Determinants of Early Childhood DevelopmentMayson BaliNo ratings yet
- Novel Pulmonary Drug Delivery MaysDocument20 pagesNovel Pulmonary Drug Delivery MaysMayson BaliNo ratings yet
- HPLC Lab RepDocument11 pagesHPLC Lab RepMayson BaliNo ratings yet
- Lec 12 - Drugs Used in PTDocument14 pagesLec 12 - Drugs Used in PTAiqa QaziNo ratings yet
- Pathophysiology QBDocument5 pagesPathophysiology QBVimlesh PalNo ratings yet
- Opath Lab. Pulp Periapical Diseases CompleteDocument3 pagesOpath Lab. Pulp Periapical Diseases CompleteJaira LaguidaoNo ratings yet
- Fact SheetDocument2 pagesFact SheetGeorge DupontNo ratings yet
- Chuko YyDocument1 pageChuko YyIanjames BenedictoNo ratings yet
- იმუნოს ზეპირი 1 1Document65 pagesიმუნოს ზეპირი 1 1Levani KartvelishviliNo ratings yet
- Maternal Respiratory Sars-Cov-2 Infection in Pregnancy Is Associated With A Robust Inflammatory Response at The Maternal-Fetal InterfaceDocument31 pagesMaternal Respiratory Sars-Cov-2 Infection in Pregnancy Is Associated With A Robust Inflammatory Response at The Maternal-Fetal InterfaceAllan Depieri CataneoNo ratings yet
- A Clinical Study On Durdagdhaw.s.r To Second Degree Superficial Burn and Its Management With Indigenous Drugs.)Document3 pagesA Clinical Study On Durdagdhaw.s.r To Second Degree Superficial Burn and Its Management With Indigenous Drugs.)KrishnaNo ratings yet
- Heart Rate Variability Measurement and Emerging UsDocument11 pagesHeart Rate Variability Measurement and Emerging UsDario GerpeNo ratings yet
- Microbiolgy PPT Wuchereria BancroftiDocument17 pagesMicrobiolgy PPT Wuchereria BancroftiBeerasandrapalyaRangaiahRavikumar100% (1)
- The Clinical Complications of Asthma and Its Pharmacotherapy PDFDocument30 pagesThe Clinical Complications of Asthma and Its Pharmacotherapy PDFHow ToNo ratings yet
- Food and Chemical Toxicology: Can Ali Agca, Mehmet Tuzcu, Armagan Hayirli, Kazim SahinDocument6 pagesFood and Chemical Toxicology: Can Ali Agca, Mehmet Tuzcu, Armagan Hayirli, Kazim SahinΔημητρης ΦιλιογλουNo ratings yet
- 6 Helpful Ways To Boost Immune HealthDocument6 pages6 Helpful Ways To Boost Immune HealthDennis Noel BejerNo ratings yet
- Eular References For Website 2015Document240 pagesEular References For Website 2015Antonio BernalNo ratings yet
- How Magnetic Therapy & Negative Ion Technology Can Aid Well-Being & Exercise RecoveryDocument9 pagesHow Magnetic Therapy & Negative Ion Technology Can Aid Well-Being & Exercise RecoveryDilpreet SinghNo ratings yet
- Molecular Mechanism of Radicular Cyst FormationDocument10 pagesMolecular Mechanism of Radicular Cyst FormationMustaida 910No ratings yet
- Test Bank For Essentials of Human Diseases and Conditions 4th Edition FrazierDocument6 pagesTest Bank For Essentials of Human Diseases and Conditions 4th Edition Frazierbevisphuonglc1u5No ratings yet
- (Lung Biology in Health and Disease, V. 137) Richard D Bland - Jacqueline J Coalson-Chronic Lung Disease in Early Infancy-Marcel Dekker (2000)Document1,080 pages(Lung Biology in Health and Disease, V. 137) Richard D Bland - Jacqueline J Coalson-Chronic Lung Disease in Early Infancy-Marcel Dekker (2000)Uri MoraNo ratings yet
- Chapter 6 - Inflammation, Tissue Repair & FeverDocument8 pagesChapter 6 - Inflammation, Tissue Repair & FeverChrista CastorNo ratings yet
- Case PresentationDocument39 pagesCase PresentationAnni BarbaNo ratings yet
- 5 Stages of FastingDocument7 pages5 Stages of FastingMahdiNo ratings yet
- Circulating Myeloid-Derived MMP8 in Stress Susceptibility and DepressionDocument35 pagesCirculating Myeloid-Derived MMP8 in Stress Susceptibility and Depressionnishantbhardwaj104No ratings yet
- Type 2 Diabetes - Term PaperDocument10 pagesType 2 Diabetes - Term Paperapi-581991695No ratings yet
- Tugas Giving AdviceDocument9 pagesTugas Giving Adviceputri rahayuNo ratings yet