You might also like
- Prevention, Preparedness and Response Guidelines for Spodoptera FrugiperdaFrom EverandPrevention, Preparedness and Response Guidelines for Spodoptera FrugiperdaNo ratings yet
- Major Accidents to the Environment: A Practical Guide to the Seveso II-Directive and COMAH RegulationsFrom EverandMajor Accidents to the Environment: A Practical Guide to the Seveso II-Directive and COMAH RegulationsNo ratings yet
- Outbreaks On ShipsDocument12 pagesOutbreaks On ShipscaptkcNo ratings yet
- WHO 2019 NCov IHR Ship Outbreak 2020Document12 pagesWHO 2019 NCov IHR Ship Outbreak 2020Bheru LalNo ratings yet
- 5600 - Updated Interim Guidance For Airlines and Airline Crew - Coronavirus Disease 2019 (COVID-19) - CDCDocument4 pages5600 - Updated Interim Guidance For Airlines and Airline Crew - Coronavirus Disease 2019 (COVID-19) - CDCPutri SyawalNo ratings yet
- WHO 2019 nCoV POEmgmt 2020Document7 pagesWHO 2019 nCoV POEmgmt 2020Bheru LalNo ratings yet
- Technical Circular No076Document5 pagesTechnical Circular No076lukky prasetyoNo ratings yet
- Naming The Coronavirus Disease (COVID-19) and The Virus That Causes ItDocument7 pagesNaming The Coronavirus Disease (COVID-19) and The Virus That Causes ItJay JayNo ratings yet
- An Implementation Guide For The Management of COVID-19 On Board Cargo Ships and Fishing VesselsDocument14 pagesAn Implementation Guide For The Management of COVID-19 On Board Cargo Ships and Fishing VesselsE.Caglar BugraNo ratings yet
- Coronavirus Disease 2019 (COVID-19) - Anesthetic Concerns, Including Airway Management and Infection ControlDocument32 pagesCoronavirus Disease 2019 (COVID-19) - Anesthetic Concerns, Including Airway Management and Infection ControlT GalenNo ratings yet
- Infection Prevention and Control and Preparedness For COVID-19 in Healthcare SettingsDocument20 pagesInfection Prevention and Control and Preparedness For COVID-19 in Healthcare SettingsMatthew DavisNo ratings yet
- Electronic Bulletin: International Civil Aviation OrganizationDocument13 pagesElectronic Bulletin: International Civil Aviation OrganizationRohit JoshiNo ratings yet
- Coronavirus Disease 2019 (COVID-19) : Airway Management, Anesthesia Machine VentiDocument31 pagesCoronavirus Disease 2019 (COVID-19) : Airway Management, Anesthesia Machine Ventisara avendanoNo ratings yet
- Standard Operating ProcedureDocument15 pagesStandard Operating ProcedureAyman AliNo ratings yet
- 22-10 Health Advisory - Guidance For EMS Professionals On Suspected Cases of MonkeypoxDocument4 pages22-10 Health Advisory - Guidance For EMS Professionals On Suspected Cases of MonkeypoxNorth Country EMSNo ratings yet
- Port Health - OverviewDocument30 pagesPort Health - OverviewKay BristolNo ratings yet
- Biological Agents Risk Assessment in Hse Acute HC Facilities Excl Lab During Covid 19Document8 pagesBiological Agents Risk Assessment in Hse Acute HC Facilities Excl Lab During Covid 19visutsiNo ratings yet
- WHO 2019 nCoV Policy Brief Risk Based International Travel 2021.1 EngDocument6 pagesWHO 2019 nCoV Policy Brief Risk Based International Travel 2021.1 EngOsama RathoreNo ratings yet
- Cinema Safety During The COVID-19 Pandemic in The CaribbeanDocument7 pagesCinema Safety During The COVID-19 Pandemic in The CaribbeanNishelle JeffreyNo ratings yet
- IATA Final-Revised-Bulletin-3-Guideline-For-Ground-Handling-In-Case-Of-CovidDocument21 pagesIATA Final-Revised-Bulletin-3-Guideline-For-Ground-Handling-In-Case-Of-CovidToto SubagyoNo ratings yet
- Easa Sib 2020-02R2 1Document4 pagesEasa Sib 2020-02R2 1alexis patearroyNo ratings yet
- Infection Prevention and Control For Seasonal Respiratory Infections in Health and Care SettingsDocument29 pagesInfection Prevention and Control For Seasonal Respiratory Infections in Health and Care Settingsmulyono ajiNo ratings yet
- ADA COVID Int Guidance Treat Pts 2 PDFDocument8 pagesADA COVID Int Guidance Treat Pts 2 PDFAnil SukumaranNo ratings yet
- 2019 Novel Coronavirus (COVID-19) : Availability of Personal Protective EquipmentDocument4 pages2019 Novel Coronavirus (COVID-19) : Availability of Personal Protective EquipmentPetroNo ratings yet
- ADA Interim Guidance For Minimizing Risk of COVID-19 TransmissionDocument8 pagesADA Interim Guidance For Minimizing Risk of COVID-19 TransmissionprasaddenNo ratings yet
- ADA COVID Int Guidance Treat Pts PDFDocument8 pagesADA COVID Int Guidance Treat Pts PDFJavier NicolaldeNo ratings yet
- ADA Interim Guidance For Minimizing Risk of COVID-19 TransmissionDocument8 pagesADA Interim Guidance For Minimizing Risk of COVID-19 TransmissionMaria Paula Vanegas ForeroNo ratings yet
- ADA COVID Int Guidance Treat Pts PDFDocument8 pagesADA COVID Int Guidance Treat Pts PDFFavio LunaNo ratings yet
- ADA Interim Guidance For Minimizing Risk of COVID-19 TransmissionDocument8 pagesADA Interim Guidance For Minimizing Risk of COVID-19 TransmissionOTNo ratings yet
- EVD WHO Guidance PoE 14.1 EngDocument11 pagesEVD WHO Guidance PoE 14.1 EngAsri RachmawatiNo ratings yet
- Manual 3rd Edition - enDocument78 pagesManual 3rd Edition - enCarlos BatistaNo ratings yet
- English - EUBS-ECHM Position On Diving and COVID-19 (21st May 2020)Document3 pagesEnglish - EUBS-ECHM Position On Diving and COVID-19 (21st May 2020)dausjkNo ratings yet
- Guidance For Prevention and Management of Cases of COVID-19 On Offshore Installations During The Delay PhaseDocument21 pagesGuidance For Prevention and Management of Cases of COVID-19 On Offshore Installations During The Delay PhaseMOHAMEDNo ratings yet
- Infection Prevention and Control Guideline For Ports of EntryDocument12 pagesInfection Prevention and Control Guideline For Ports of EntryHareth Al NajriNo ratings yet
- IAB Ebola PPE Recommendations - 10 24 14Document11 pagesIAB Ebola PPE Recommendations - 10 24 14Guillermo GarayNo ratings yet
- Interim Guidance For Ships On Managing Cases of COVID19Document15 pagesInterim Guidance For Ships On Managing Cases of COVID19ОлегNo ratings yet
- Anesthesia Management in CovidDocument4 pagesAnesthesia Management in CovidMuhammad Farooq AfzalNo ratings yet
- COVID-19 - Infection Control For Persons With SARS-CoV-2 Infection - UpToDateDocument35 pagesCOVID-19 - Infection Control For Persons With SARS-CoV-2 Infection - UpToDateDuy Hùng HoàngNo ratings yet
- Temporary Covid-19 Precautions During An Inspection: Vers 1 - 8 June 2020Document5 pagesTemporary Covid-19 Precautions During An Inspection: Vers 1 - 8 June 2020KhaledMazenNo ratings yet
- INTERTANKO 2020-Covid Management Plan - 3 - LoDocument17 pagesINTERTANKO 2020-Covid Management Plan - 3 - LoerolNo ratings yet
- 28june2020 20200628 Guidelines For International Departure From Pakistan 02Document5 pages28june2020 20200628 Guidelines For International Departure From Pakistan 02Ozair MansoorNo ratings yet
- Dissertation ProposalDocument3 pagesDissertation ProposalKyle Van RipperNo ratings yet
- PAHOPHEIHMCovid1920002 EngDocument5 pagesPAHOPHEIHMCovid1920002 EngfrehanyaqNo ratings yet
- Coronavirus Disease 2019 (COVID-19) GuidelinesDocument13 pagesCoronavirus Disease 2019 (COVID-19) Guidelinesrajesh BNo ratings yet
- Referensi Pembacaan ReferatDocument5 pagesReferensi Pembacaan Referataswad 0008No ratings yet
- Coronavirus GuidelinesDocument24 pagesCoronavirus GuidelinesHugo Vco RvaNo ratings yet
- Covid-19 - General Guidance For The Management of The Dead Icrc Forensic UnitDocument15 pagesCovid-19 - General Guidance For The Management of The Dead Icrc Forensic UnitBOSS 2049No ratings yet
- Via Aerea COVID 19Document3 pagesVia Aerea COVID 19zunarodriguezleoNo ratings yet
- Guidance COVID 19Document3 pagesGuidance COVID 19Fitri Najmi NajidNo ratings yet
- Covid Medical Evidence For Strategies 200423Document11 pagesCovid Medical Evidence For Strategies 200423Sagar KandelNo ratings yet
- Imo Circular Letter No.3484Document7 pagesImo Circular Letter No.3484Thich LikeNo ratings yet
- An Airport Operations Proposal For A Pandemic-Free Air TravelDocument9 pagesAn Airport Operations Proposal For A Pandemic-Free Air TraveldesiNo ratings yet
- Who SSC and SscecDocument16 pagesWho SSC and SscecsupriyodebNo ratings yet
- Intensive Care Unit Setup For COVID-19Document10 pagesIntensive Care Unit Setup For COVID-19BAGUIO CATSNo ratings yet
- Coronavirus COVID 19 Guidance For Ship Operators For The Protection of The Health of Seafarers Fifth EditionDocument62 pagesCoronavirus COVID 19 Guidance For Ship Operators For The Protection of The Health of Seafarers Fifth EditionAtesh RanaNo ratings yet
- Identify The Significance of International Air Transport Association (IATA) in Preventing The Spread of Public Health Events of International ConcernDocument3 pagesIdentify The Significance of International Air Transport Association (IATA) in Preventing The Spread of Public Health Events of International ConcernNedo JnrNo ratings yet
- Brote de COVID-19 en Italia Proteger La Salud de Los Trabajadores y La Respuesta de La Asociación Italiana de Higienistas IndustrialesDocument15 pagesBrote de COVID-19 en Italia Proteger La Salud de Los Trabajadores y La Respuesta de La Asociación Italiana de Higienistas IndustrialesChristian PinoNo ratings yet
- Interim Guidance On Aircraft Cleaning and DisinfectionDocument8 pagesInterim Guidance On Aircraft Cleaning and DisinfectionjarrisonNo ratings yet
- Transportation WhitePaper COVID Response-V2Document18 pagesTransportation WhitePaper COVID Response-V2Amit AgarwalNo ratings yet
- Approaches To The Management of Patients in Oral and Maxillofacial Surgery During COVID-19 PandemicDocument21 pagesApproaches To The Management of Patients in Oral and Maxillofacial Surgery During COVID-19 PandemicYahul MazfarNo ratings yet
- Maritime Security Review (16 - 22 May 2016)Document28 pagesMaritime Security Review (16 - 22 May 2016)Dennis VolodchenkoNo ratings yet
- Guidance For CIC On Safety of Navigation 2017Document19 pagesGuidance For CIC On Safety of Navigation 2017Dennis VolodchenkoNo ratings yet
- Chartpilot 1100 Manual (New UPDATE 2017)Document442 pagesChartpilot 1100 Manual (New UPDATE 2017)Buzatu Mircea100% (6)
- USCG - Foreign Freight Vessel Examination Book PDFDocument47 pagesUSCG - Foreign Freight Vessel Examination Book PDFRahul SinghNo ratings yet
- Hull Inspection ManualDocument92 pagesHull Inspection ManualDennis Volodchenko100% (5)
- ECDIS Guidelines Final 4-Hi-ResDocument36 pagesECDIS Guidelines Final 4-Hi-Resvi83% (6)
- What Exactly Are Period PantiesDocument2 pagesWhat Exactly Are Period PantiesJay Jay KamgaNo ratings yet
- The Three Modern Relationship Models and Why They Are All FlawedDocument5 pagesThe Three Modern Relationship Models and Why They Are All FlawedBingoNo ratings yet
- Aaron Magana's Resume, Business AnalystDocument3 pagesAaron Magana's Resume, Business AnalystEmiNo ratings yet
- SAVULESCU, Julian - A Simple Solution To The Puzzles of End of LifeDocument5 pagesSAVULESCU, Julian - A Simple Solution To The Puzzles of End of Lifediradosta_1992No ratings yet
- Science 10 Q3 - M2Document14 pagesScience 10 Q3 - M2Avha CortesNo ratings yet
- Huanyang Inverter Instruction (Eng) .300dpi.67pages - OcrDocument70 pagesHuanyang Inverter Instruction (Eng) .300dpi.67pages - Ocrkyuwan kimNo ratings yet
- Formulating A Dental Treatment Plan: DR Tashnim BagusDocument33 pagesFormulating A Dental Treatment Plan: DR Tashnim BagustarekrabiNo ratings yet
- Material Data Sheet Durapro Asa: DescriptionDocument1 pageMaterial Data Sheet Durapro Asa: DescriptionAlexandru NeacsuNo ratings yet
- Income Taxation Module Compilation FinalsDocument107 pagesIncome Taxation Module Compilation FinalsJasmine CardinalNo ratings yet
- PR Project - 3rd FinalDocument26 pagesPR Project - 3rd FinalLavish ChanodiaNo ratings yet
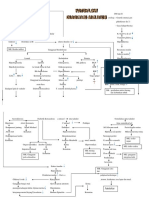
- Patoflow DMDocument2 pagesPatoflow DMAngel da CostaNo ratings yet
- WaveLab - BUC Datasheet - Ku Band 80W 100WDocument4 pagesWaveLab - BUC Datasheet - Ku Band 80W 100WLeonNo ratings yet
- Reading Passage 1: IELTS Recent Actual Test With Answers Volume 1Document17 pagesReading Passage 1: IELTS Recent Actual Test With Answers Volume 1Amogha GadkarNo ratings yet
- 10 Achievement ChartDocument3 pages10 Achievement ChartLyka ollerasNo ratings yet
- RPLB NewDocument22 pagesRPLB NewMeta learnNo ratings yet
- Pengertian Recount Text Kls 9Document26 pagesPengertian Recount Text Kls 9MARINDRA RETNONo ratings yet
- Jeremiah's Law, Introduced by Assemblywoman Rodneyse BichotteDocument2 pagesJeremiah's Law, Introduced by Assemblywoman Rodneyse BichotteCity & State NYNo ratings yet
- Department of Civil Engineering Uttara University: LaboratoryDocument102 pagesDepartment of Civil Engineering Uttara University: LaboratorytaniaNo ratings yet
- Batch Records HandoDocument39 pagesBatch Records HandoNiranjan SinghNo ratings yet
- EVVO 10-15KW-G2 - IEC 61727 - ReportDocument25 pagesEVVO 10-15KW-G2 - IEC 61727 - ReportRadhwen ZayoudNo ratings yet
- Offshore Drilling Operation in East Indonesia Oil and Gas FieldsDocument3 pagesOffshore Drilling Operation in East Indonesia Oil and Gas FieldsMuhammad Galih Eko SaputroNo ratings yet
- Chapter 10 Fitness Training PrinciplesDocument80 pagesChapter 10 Fitness Training Principlesapi-115744109No ratings yet
- 2 TABLE 1.1. Key Events in The Development of Cell and Tissue CultureDocument1 page2 TABLE 1.1. Key Events in The Development of Cell and Tissue CultureCatalina ColoradoNo ratings yet
- Problems SetDocument10 pagesProblems SetSajith KurianNo ratings yet
- A Report About Cavitation Phenomenon-By Murtadha Adil Tahir jassim - مرتضى عادل طاهر جاسمDocument15 pagesA Report About Cavitation Phenomenon-By Murtadha Adil Tahir jassim - مرتضى عادل طاهر جاسمAnmar HamidNo ratings yet
- Know Your Customer BrochureDocument4 pagesKnow Your Customer BrochureTEL COMENo ratings yet
- Blood Stasis and What Does That MeanDocument2 pagesBlood Stasis and What Does That MeanCarl MacCordNo ratings yet
- Anesthesiology GuideDocument4 pagesAnesthesiology GuideGeorge Wang100% (1)
- Kyocera Fs 1118mfpKm1820Document200 pagesKyocera Fs 1118mfpKm1820Jane VinuyaNo ratings yet