You might also like
- Hereditary Spherocytosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHereditary Spherocytosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- 5.2 Renal Masses and Congenital AnomaliesDocument9 pages5.2 Renal Masses and Congenital AnomaliesMaria roxanne HernandezNo ratings yet
- Causes of Peptic Ulcers:: Helicobacter Pylori (H. Pylori)Document4 pagesCauses of Peptic Ulcers:: Helicobacter Pylori (H. Pylori)jessie monroeNo ratings yet
- RCJ Finals - Non Epithelial Ovarian CaDocument4 pagesRCJ Finals - Non Epithelial Ovarian CaJohn Paulo Catacutan100% (1)
- EARLY CRC (Peran Bedah Dokter Dalam Diagnosis Dini Karsinoma Kolo-Rectal) Prof - Dr.dr. Ing - Riwanto, SPB-KBDDocument31 pagesEARLY CRC (Peran Bedah Dokter Dalam Diagnosis Dini Karsinoma Kolo-Rectal) Prof - Dr.dr. Ing - Riwanto, SPB-KBDHengky TanNo ratings yet
- Clinical Management: PGI Eileen Andres PediatricsDocument9 pagesClinical Management: PGI Eileen Andres PediatricsMichael BonillaNo ratings yet
- Case Presentation:: DR - Amra Farrukh PG.T Su.IDocument75 pagesCase Presentation:: DR - Amra Farrukh PG.T Su.IpeeconNo ratings yet
- Degeneration and Regenration of Nerve Fibers by Dr. RoomiDocument11 pagesDegeneration and Regenration of Nerve Fibers by Dr. RoomiMudassar RoomiNo ratings yet
- Acute Abdominal Pain MS LectureDocument63 pagesAcute Abdominal Pain MS Lectureheka_amrongNo ratings yet
- CARCINOGENESIS CRC Prof RiwantoDocument48 pagesCARCINOGENESIS CRC Prof Riwantoand3sgr3atNo ratings yet
- Hemorrhagic Conditions in Neonates: DR Hodan Ahmed, Department of Pediatrics and Child Health, Amoud Medical School, AUDocument27 pagesHemorrhagic Conditions in Neonates: DR Hodan Ahmed, Department of Pediatrics and Child Health, Amoud Medical School, AUAbdisalan hassanNo ratings yet
- Surgical Nutritions: Prepared By: Lilibeth C.Tenorio, M.DDocument33 pagesSurgical Nutritions: Prepared By: Lilibeth C.Tenorio, M.DLilibeth Tenorio De Leon100% (1)
- Liver Tumors BasicDocument37 pagesLiver Tumors BasicSahirNo ratings yet
- PR BleedDocument20 pagesPR BleedCathy KayNo ratings yet
- Chest Trauma55Document60 pagesChest Trauma55micheal1960No ratings yet
- Peptic ulcer disease: causes, symptoms, diagnosis and treatmentDocument24 pagesPeptic ulcer disease: causes, symptoms, diagnosis and treatmentms khan100% (1)
- Abdominal Pain: Resources: Murtagh, John. General Practice 5 EdDocument26 pagesAbdominal Pain: Resources: Murtagh, John. General Practice 5 EdDewanti PermatasariNo ratings yet
- Case Presentation: Lump Right HypochondriumDocument22 pagesCase Presentation: Lump Right HypochondriumNANDAN RAINo ratings yet
- Bladder Cancer Treatment Regimens: Clinical Trials, Chemotherapy OptionsDocument4 pagesBladder Cancer Treatment Regimens: Clinical Trials, Chemotherapy Optionsc.ramNo ratings yet
- Colon, Rectum and Anus-Dr. SigitDocument121 pagesColon, Rectum and Anus-Dr. SigitYuliana Latif100% (1)
- Upper Gi BleedDocument20 pagesUpper Gi BleedNaeem Shehzad100% (1)
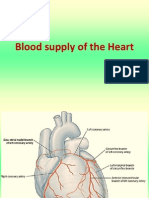
- Blood Supply of HeartDocument7 pagesBlood Supply of Heartmariposa_0612No ratings yet
- Extrahepatic CholestasisDocument31 pagesExtrahepatic CholestasismackieccNo ratings yet
- Vitamin B12 Deficiency and A Patient Case StudyDocument36 pagesVitamin B12 Deficiency and A Patient Case Studynherm6425100% (1)
- Neuro General Neuro: Proptosis/ Exophthalmos ChemosisDocument4 pagesNeuro General Neuro: Proptosis/ Exophthalmos ChemosisShakina FareedNo ratings yet
- Acute Abdominal Pain: Associate Professor, Dept. of Surgery Mti, KMC, KTHDocument45 pagesAcute Abdominal Pain: Associate Professor, Dept. of Surgery Mti, KMC, KTHWaleed MaboodNo ratings yet
- AthetosisDocument2 pagesAthetosisapi-19973386No ratings yet
- Directions: Each Question Below Contains Five Suggested Answers. Choose The One Best Response ToDocument3 pagesDirections: Each Question Below Contains Five Suggested Answers. Choose The One Best Response ToTrottTamilNo ratings yet
- PancreatitisDocument51 pagesPancreatitisMizrab NadeemNo ratings yet
- Current Trends in Management of CholedocholithiasisDocument35 pagesCurrent Trends in Management of Choledocholithiasisrajan kumar100% (6)
- SAGES Gallbladder CBDDocument54 pagesSAGES Gallbladder CBDSAGESWeb100% (1)
- TB in Children: Department of Pediatrics College of Medicine Cagayan State UniversityDocument49 pagesTB in Children: Department of Pediatrics College of Medicine Cagayan State UniversityyayayanizaNo ratings yet
- Poorly Differentiated Thyroid CarcinomaDocument67 pagesPoorly Differentiated Thyroid Carcinomaperie_md100% (1)
- Etiology and Diagnosis of Bile Duct StonesDocument8 pagesEtiology and Diagnosis of Bile Duct Stoneskuncupcupu1368No ratings yet
- Pancreatic Cancer: Early Detection Offers Best Chance of CureDocument18 pagesPancreatic Cancer: Early Detection Offers Best Chance of Curemywifenoor1983No ratings yet
- Advances in Surgical NutritionDocument42 pagesAdvances in Surgical NutritionpratoshNo ratings yet
- Jaundice: Seminar Under The Guidance Of-Dr. Shiva NarangDocument47 pagesJaundice: Seminar Under The Guidance Of-Dr. Shiva NarangMiguel MansillaNo ratings yet
- Benign Prostate Hyperplasia: Div. of Urology, Dept. Surgery Medical Faculty, University of Sumatera UtaraDocument56 pagesBenign Prostate Hyperplasia: Div. of Urology, Dept. Surgery Medical Faculty, University of Sumatera UtaraJessica PurbaNo ratings yet
- Alvin B. Vibar, M.D.Document49 pagesAlvin B. Vibar, M.D.Ditas ChuNo ratings yet
- Anemia in CKD Patient On HeamodialysisDocument32 pagesAnemia in CKD Patient On HeamodialysisEditor IJTSRDNo ratings yet
- Palliative EnciesDocument96 pagesPalliative EnciesnandanNo ratings yet
- LIVERDISEASEDocument82 pagesLIVERDISEASEHervis FantiniNo ratings yet
- Colon cancer screening recommendations and barriersDocument7 pagesColon cancer screening recommendations and barriersKen Ancheta LagayadaNo ratings yet
- Post Gastrectomy SyndromeDocument34 pagesPost Gastrectomy SyndromeWasim R. IssaNo ratings yet
- Metabolism in SurgeryDocument5 pagesMetabolism in Surgeryjc_sibal13No ratings yet
- Carcinoma of The Breast - Bailey & LoveDocument5 pagesCarcinoma of The Breast - Bailey & LoveKeyshia Yazid100% (1)
- Baltarowich ABD pt1 Hepatobiliary US PDFDocument22 pagesBaltarowich ABD pt1 Hepatobiliary US PDFEka KusumaningatiNo ratings yet
- Benign and Malignant Lesion of Lower GIDocument45 pagesBenign and Malignant Lesion of Lower GIAhmad Alzu3beNo ratings yet
- September 2017 QuestionsDocument13 pagesSeptember 2017 QuestionsAllison Eunice ServandoNo ratings yet
- Enterocutaneous FistulasDocument15 pagesEnterocutaneous FistulaslizinkatruyenqueNo ratings yet
- Kholesistis & Kholelitiasis 30-11-14Document67 pagesKholesistis & Kholelitiasis 30-11-14Dian AzhariaNo ratings yet
- Faculty of Medicine NR - Ii Department of Surgery NR - Ii: Diseases of The Biliary TractDocument40 pagesFaculty of Medicine NR - Ii Department of Surgery NR - Ii: Diseases of The Biliary TractGalina LozovanuNo ratings yet
- Ob SGDDocument88 pagesOb SGDFerdinand Luis SuarezNo ratings yet
- Bariatric SurgeryDocument26 pagesBariatric SurgeryAmyandNo ratings yet
- Billiary SystemDocument60 pagesBilliary SystemDONALD UNASHENo ratings yet
- Postcholecystectomy SyndromeDocument27 pagesPostcholecystectomy SyndromeMonica TurnerNo ratings yet
- Stomach and Duodenum 10-27Document32 pagesStomach and Duodenum 10-27Ditas ChuNo ratings yet
- 54.the Gallbladder and Bile DuctsDocument19 pages54.the Gallbladder and Bile DuctsAdenegan Adesola RaymondNo ratings yet
- Colorectal Cancer PDFDocument2 pagesColorectal Cancer PDFElizabeth100% (1)
- Nephrolithiasis: An Overview of Kidney Stone Types and PathogenesisDocument81 pagesNephrolithiasis: An Overview of Kidney Stone Types and PathogenesisOmar Zaman KhanNo ratings yet
- Clinical Management of Type C Hepatic Encephalopathy PDFDocument8 pagesClinical Management of Type C Hepatic Encephalopathy PDFhoneyworksNo ratings yet
- Sarfaraz Jalil Baig, Deepraj Bhandarkar, Pallawi Priya - Newer Concepts and Procedures in Hernia Surgery - An Atlas-Springer (2023)Document258 pagesSarfaraz Jalil Baig, Deepraj Bhandarkar, Pallawi Priya - Newer Concepts and Procedures in Hernia Surgery - An Atlas-Springer (2023)honeyworksNo ratings yet
- NH Protocol For Covid Management FinalDocument7 pagesNH Protocol For Covid Management FinalhoneyworksNo ratings yet
- Options Theory Guide for Professional TradingDocument134 pagesOptions Theory Guide for Professional TradingVibhats VibhorNo ratings yet
- Exocrine Pancreatic Insufficiency in AdultsDocument18 pagesExocrine Pancreatic Insufficiency in Adultshoneyworks100% (1)
- 1 DiagnosisDocument3 pages1 DiagnosishoneyworksNo ratings yet
- Wallflexbiliary Productinfo Brochure PDFDocument6 pagesWallflexbiliary Productinfo Brochure PDFhoneyworksNo ratings yet
- Human Pancreatic Exocrine Response To Nutrients in Health and DiseaseDocument28 pagesHuman Pancreatic Exocrine Response To Nutrients in Health and DiseasehoneyworksNo ratings yet
- Role of Liver Biopsy Accuracy2Document3 pagesRole of Liver Biopsy Accuracy2honeyworksNo ratings yet
- Dose EscalationDocument14 pagesDose EscalationhoneyworksNo ratings yet
- ReferencesDocument4 pagesReferenceshoneyworksNo ratings yet
- Olympus EndosDocument9 pagesOlympus EndoshoneyworksNo ratings yet
- Subhashitharathnalu PDFDocument57 pagesSubhashitharathnalu PDFhoneyworksNo ratings yet
- He Pa To Renal Syndrome PublishedDocument10 pagesHe Pa To Renal Syndrome PublishedhoneyworksNo ratings yet
- Anal Carcinoma: NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines)Document54 pagesAnal Carcinoma: NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines)honeyworksNo ratings yet
- Indigo Boarding Pass SampleDocument1 pageIndigo Boarding Pass Samplehoneyworks67% (3)
- BSG Guidelines On Inflammatory Bowel Disease BiopsiesDocument57 pagesBSG Guidelines On Inflammatory Bowel Disease BiopsieshoneyworksNo ratings yet
- Dakshinamurthy Stotram Sri Adi Shankaracharya Swami - Telugu - PDF - File1561 PDFDocument19 pagesDakshinamurthy Stotram Sri Adi Shankaracharya Swami - Telugu - PDF - File1561 PDFp_sudheersharmaNo ratings yet
- BSG Guidelines On Inflammatory Bowel Disease Biopsies PDFDocument22 pagesBSG Guidelines On Inflammatory Bowel Disease Biopsies PDFhoneyworksNo ratings yet
- ACG Guideline Focal Liver Lesions September 2014Document20 pagesACG Guideline Focal Liver Lesions September 2014Michael Abel Espinoza SalvatierraNo ratings yet
- Biosimilars: Pros and Cons in Current Practice: MBBS, MRCP (Uk), FRCP (Edin), FamsDocument51 pagesBiosimilars: Pros and Cons in Current Practice: MBBS, MRCP (Uk), FRCP (Edin), FamshoneyworksNo ratings yet
- Isha Upanishad With AccentsDocument2 pagesIsha Upanishad With AccentsbjmfNo ratings yet
- Autoimmune Hepatitis and Overlap Syndromes Diagnosis and ManagementDocument21 pagesAutoimmune Hepatitis and Overlap Syndromes Diagnosis and ManagementhoneyworksNo ratings yet
- BSG Guidelines On Inflammatory Bowel Disease Biopsies PDFDocument22 pagesBSG Guidelines On Inflammatory Bowel Disease Biopsies PDFhoneyworksNo ratings yet
- Devlin 2016Document7 pagesDevlin 2016honeyworksNo ratings yet
- Benign Liver Tumours EASL CPGDocument34 pagesBenign Liver Tumours EASL CPGhoneyworksNo ratings yet
- Ash Sap 2016Document672 pagesAsh Sap 2016honeyworksNo ratings yet
- Pi Is 1542356513007076Document7 pagesPi Is 1542356513007076honeyworksNo ratings yet
- Acercamiento A Paciente Con Ictericia Goldman-Cecil MedicineDocument15 pagesAcercamiento A Paciente Con Ictericia Goldman-Cecil MedicineGeraldine RuizNo ratings yet
- Harrison - Gastroenterology and Hepatology - 2013 Ed 18 PDFDocument784 pagesHarrison - Gastroenterology and Hepatology - 2013 Ed 18 PDFCarmen Elena Plaisanu94% (32)
- Ascending Cholangitis - Pao EditDocument62 pagesAscending Cholangitis - Pao EditSamuel WibowoNo ratings yet
- Obstructive JaundiceDocument54 pagesObstructive JaundiceJenine Ezra M. Conol50% (2)
- Virtual EAV: The Electro-Dermal Screening TestDocument21 pagesVirtual EAV: The Electro-Dermal Screening Testmich100% (1)
- Abdominal UltrasoundDocument15 pagesAbdominal UltrasoundAmin100% (2)
- Donor Liver and Kidney Frozen Section Evaluation CriteriaDocument7 pagesDonor Liver and Kidney Frozen Section Evaluation CriteriaJose SirittNo ratings yet
- Kidney and Liver FunctionDocument6 pagesKidney and Liver FunctionAhmad Ripani Musyaffa AhdanLabNo ratings yet
- Lecture 22 - The Digestive TractDocument32 pagesLecture 22 - The Digestive TractCarl Agape DavisNo ratings yet
- Hepatitis: Jump To Navigation Jump To SearchDocument11 pagesHepatitis: Jump To Navigation Jump To SearchZely ApriantiNo ratings yet
- ELSA 2019 Program Scientific ProgramDocument22 pagesELSA 2019 Program Scientific ProgramShinta DeboraNo ratings yet
- Lecturio 3663 JaundiceDocument12 pagesLecturio 3663 JaundicePranjali WeladiNo ratings yet
- All Shifting Final Exam Questions Complete First Shift: M Ultiple C HoiceDocument11 pagesAll Shifting Final Exam Questions Complete First Shift: M Ultiple C HoicejuliusNo ratings yet
- The Complete Abstract Book PDFDocument536 pagesThe Complete Abstract Book PDFPradeep AggarwalNo ratings yet
- A Woman, Age 35, With New-Onset Ascites: Symptoms To DiagnosisDocument6 pagesA Woman, Age 35, With New-Onset Ascites: Symptoms To DiagnosisnaveenNo ratings yet
- JaundiceDocument30 pagesJaundiceNorakmal Andika YusriNo ratings yet
- Pigment Disorders and Their PathologyDocument53 pagesPigment Disorders and Their PathologyRushi VaghelaNo ratings yet
- Bile Duct Injuries: Hiwot Fentahun (MD) Year II Surgery ResidentDocument47 pagesBile Duct Injuries: Hiwot Fentahun (MD) Year II Surgery ResidentTsega WesenNo ratings yet
- 2005 AHPBA CONGRESS ABSTRACTS—FREE PAPERS AND VIDEOSDocument100 pages2005 AHPBA CONGRESS ABSTRACTS—FREE PAPERS AND VIDEOSDrAmmar MagdyNo ratings yet
- Heaptic EncephalopathyDocument16 pagesHeaptic Encephalopathydk.clinicalresearchNo ratings yet
- Approaches To Abdominal MassDocument49 pagesApproaches To Abdominal MassPatrick JohnNo ratings yet
- Anatomy and Physiology of Biliary TreeDocument48 pagesAnatomy and Physiology of Biliary TreeKamalakanta Das100% (1)
- Medical Surgical Nursing - Lecture Notes, Study Materials and Important Questions AnswersDocument40 pagesMedical Surgical Nursing - Lecture Notes, Study Materials and Important Questions AnswersBrainKart Com73% (11)
- I-Exposure by Island Hospital - Volume 12Document16 pagesI-Exposure by Island Hospital - Volume 12Island HospitalNo ratings yet
- Ni Hms 267898Document20 pagesNi Hms 267898Thesar WaldiNo ratings yet
- Acute Liver Failure-1Document40 pagesAcute Liver Failure-1elizabethNo ratings yet
- Internal Diagnosis II Good NotesDocument83 pagesInternal Diagnosis II Good Notesbjpalmer100% (2)
- Sgot & SGPTDocument2 pagesSgot & SGPT우영박No ratings yet
- Aura Scanner Manual: by Mangalm Vastu CONTACT NUMBER-9760110246, 8273431122Document11 pagesAura Scanner Manual: by Mangalm Vastu CONTACT NUMBER-9760110246, 8273431122Venkatesha Rao100% (1)
- Anatomy of the SpleenDocument18 pagesAnatomy of the Spleenزين العابدين محمد عويش100% (1)